Our paper is out!!! #redjournal
-Combination of SABR with immunotherapy in oligoprogressive patients in progression to anti-PD-1
-Multicenter study
-FU: 32.8 m
-Concurrent
-35 Gy/5fx
✅ORR 42%
✅PFS 14.2 m
✅OS 37.4 m
✅✅ Safety
@ZafraMD@delvysra
https://t.co/74pSImuXwk
This JAMA Oncology Patient Page discusses benefits and risks of local consolidative therapy for metastatic #LungCancer and which patients might be considered for this treatment. https://t.co/8DAUoBMfLh
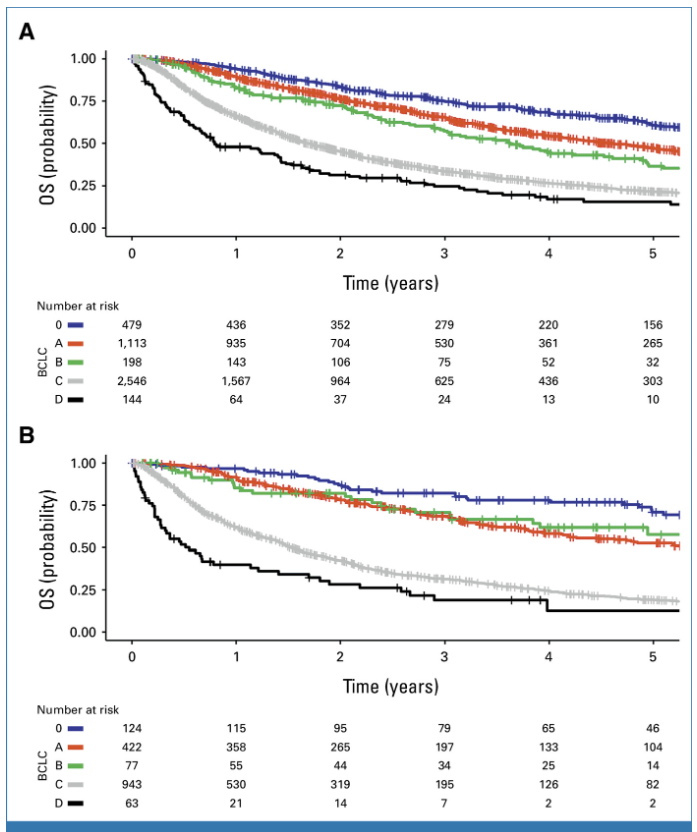
So thrilled to see our collaborative publication with @tedradonc, @ma5RN and many others now online in @JCO_ASCO
These data from a large, multinational cohort provide further support for EBRT's role in the management of HCC.
https://t.co/dJI1SdMwnK
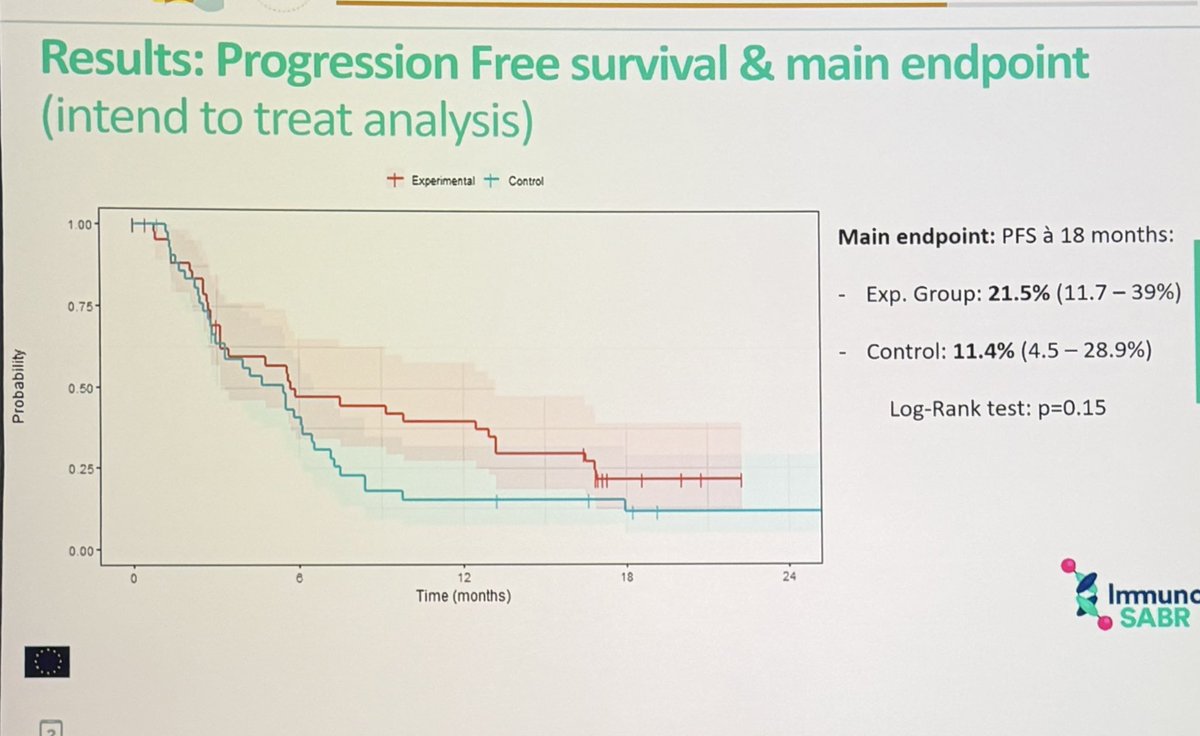
@PhilippeLambin shows an 🇳🇱 RCT where L19-IL2 immunocytokine (6 cycles) enhancement of SABR in stage IV NSCLC #lungcancer
- trial stopped early during COVID-19
- curves for PFS promising, but n.s.
- Abscopal responses higher
- increased flu-like AEs with cytokine
👏🏽👏🏽👏🏽 #ESTRO26
We present our results with the single fraction in NSCLC and lung metastases. We highlight the excellent results and convenience in an aging population with comorbidities and geographically dispersed. #ESTRO26#SABR
Plot twist in oncology and metabolism 👀
Not long ago, there was real concern that GLP-1 receptor agonists might increase the risk of rare tumors. Fast forward to ASCO GI, and we’re now seeing a signal that points in the opposite direction for colorectal cancer.
Key takeaways from this real-world head-to-head analysis 🧬
• GLP-1RA use was associated with a ~36% lower risk of colorectal cancer compared with aspirin
• Aspirin users had higher rates of GI bleeding, gastric ulcers, and AKI
• GLP-1RA users had more abdominal pain and diarrhea
• Very large population size, but observational data
It’s hard not to joke that half the country already seems to be on a GLP-1. What’s actually interesting is that a drug class built for metabolic disease may be intersecting with cancer biology in unexpected ways.
Important caveat 🚨
This is not a randomized trial. Confounding and selection bias are real, and this should not change prescribing behavior for cancer prevention.
But if this signal holds up in prospective randomized studies, the public health implications could be enormous.
From fears of rare tumors to a possible protective signal in colorectal cancer. Biology keeps humbling us.
#GI26
@OncoAlert@TheGutOncLab
In locally advanced rectal cancer, short course RT (25 Gy/5 fx) was less immunosuppressive than long-course RT, despite more advanced disease. SCRT showed faster lymphocyte recovery, lower NLR and higher intratumoral CD8+ and FOXP3+.
This immune preserving profile provides a biological rationale for SCRT-based radio-immunotherapy strategies.
https://t.co/Rfd0Hhd3d0 @OncoAlert
PLATO ACT5 Ph3 RCT (n=463): 53.2 v 58.8 v 61.6 Gy in T3-4/N+ anal SCC.
No early benefit to dose escalation w similar cCR (65-67%) across dose levels.
More uniform RT dose is not the answer – need better stratification, bio-driven personalization, RT/systemic integration. #GI26
Can we safely combine trastuzumab deruxtecan (T-DXd) with concurrent radiotherapy?
📊 Largest real-world multicentre cohort (n=147, Europe)
🧠 RT given mainly for CNS disease (≈55%)
⏱️ True concomitant RT defined as during or within 10 days of T-DXd
🛡️ Key safety results
✅ Grade ≥3 AEs: No increase with RT (11.9% RT vs 20.0% no RT, p=0.30)
✅ ILD rates similar (~10% both groups)
⚠️ Symptomatic radionecrosis: 1 case only (1.5%) after intracranial RT
🔁 Permanent T-DXd discontinuation: Similar with or without RT (~12-14%)
📈 Efficacy signal
➡️ Concomitant RT did not worsen PFS or OS
💡 Clinical takeaway
For selected patients, T-DXd + concurrent RT appears feasible and well tolerated, including CNS-directed RT. Prospective data still needed, but this supports real-world practice today.
📖 Full paper in comment ⬇️
#BreastCancer #HER2 #OncoTwitter #MedTwitter
@OncoAlert@myesmo@esmo_open@asco
📢 MITO CAÍDO: Los edulcorantes NO causan cáncer 😱
🔬 Revisión sistemática de 90 estudios analizó aspartamo, sucralosa, sacarina, acesulfame-K… y 17 tipos de cáncer.
Hilo 👇🏻👇🏻
If you haven’t heard yet #radonc - courtesy of Snr Ortega, owner/founder of @ZARA, 🇪🇸 is receiving 13 😍 proton machines as a donation to improve access to #radiotherapy. If only we had such philanthropy in Australia!!! 🦘🇦🇺🐨 @SEOR_ESP#simposioSEOR25
📢 📢 NORTHSTAR: Phase II Randomized Study of OSI +/- Local Consolidative Therapy for EGFR + NSCLC @YYElamin. First + RCT using 3rd G TKI + LCT (mPFS 25.3 vs 17.5 mo HR 0.66). Nicely discused by @ZPiotrowskaMD. #ESMO25#ESMOAmbassadors
I am delighted to share this new review in @NatureCancer that I co-author with @AnqiDong18 In which we discuss the different EMT tumor states and their implications for metastasis and cancer therapy.
📢 New in European Urology:
SABR is not just for brain mets. A systematic review shows excellent results in RCC—alone or with IO.
🧠 Local control in primary RCC
🛡️ Delay of systemic therapy in oligomets
⚡ IO + SABR: promising combos
🔗 https://t.co/pQ0xuUEOwY
#RCC#SABR #Immunotherapy #UroOncology
With this being the case, makes it difficult to endorse surgery for any of these stage IA lung cancers. SBRT or ablation is likely more than sufficient. @IPScottOh @IP_DOC@AAB_IP
Excited to be a part of this collaboration with friends and colleagues in Amsterdam. It isn't inspired entirely to advance SABR in place of surgery; instead, it is about identifying how often adrenalectomies end up with positive margins and local recurrence. The preliminary data shows it happens >50% of the time. #radonc https://t.co/Giv9GVBC4b