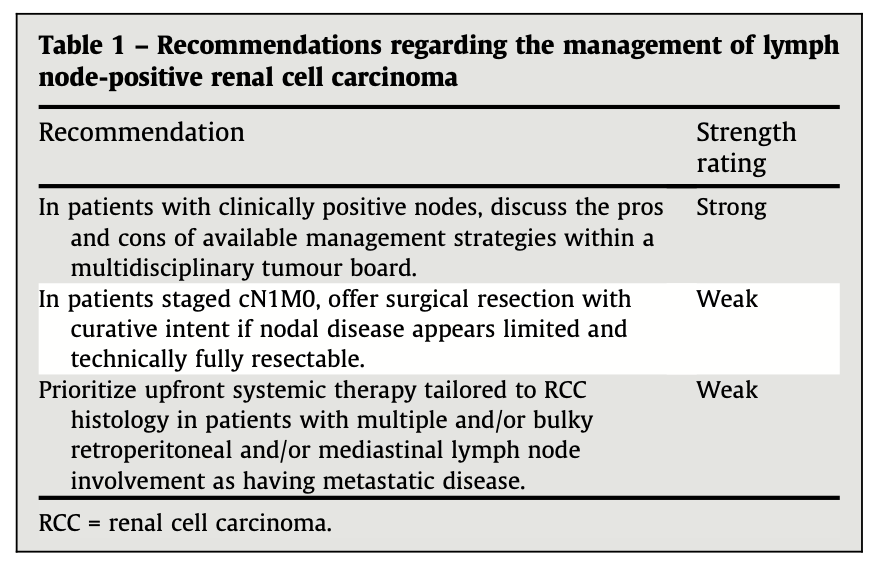
Management of Lymph Node–Positive Renal Cell Carcinoma: Updated Recommendations from the European Association of Urology Renal Cell Carcinoma Guidelines Panel
https://t.co/SsOMGbgV1j
Renal cell carcinoma with regional lymph node involvement presents a major clinical challenge, bridging localized and systemic disease. Outcomes are highly variable due to biological heterogeneity and staging limitations. Evidence remains limited, prompting individualized management.
These recommendations highlight prognostic importance of nodal invasion and risks of over- or undertreatment.
#KidneyCancer
@u_capitanio@Ric_Campi@Yasminabugh@steph_bonn@milanhoraplzen@Lorenzo_marconi@PignotG@MaxineGBTran@CrisSuFe@tompowles1@Zondervan_AUMC@drdabestani@Dr_Klatte
Chemotherapy-induced anemia as a prognostic factor for overall survival in patients with bladder cancer treated with neoadjuvant cisplatin-based chemotherapy and cystectomy
https://t.co/70SNvo2oPx
In this retrospective study of 175 patients with muscle-invasive #BladderCancer treated with cisplatin 🧪 based neoadjuvant chemotherapy followed by radical cystectomy, preoperative anemia was highly prevalent, affecting 95% of patients. Moderate-to-severe anemia (grade >1) was independently associated with significantly worse overall, relapse-free, and specific survival outcomes, whereas red blood cell 🩸 transfusions showed no prognostic impact. Additional adverse prognostic factors included elevated neutrophil count and nodal involvement after surgery. These findings highlight preoperative anemia as a potential therapeutic target warranting further investigation. #BladderCancer
@PignotG
@DrSpratticus It basically confirms the ENZARAD observation that adding an ARPI in an unselected high-risk group has minimal benefit. And yet doesn't answer the RT/RP question.
100% agree. Perhaps stated better is one of the key reasons patients choose RP is to avoid ADT and use the information from surgery and PSA to inform subsequent management.
If we blanket give them doublets and they still need postop RT people will avoid RP when outcomes may be similar or even better with postop personalized tx.
12/12 #ASCO26
Look forward to @declangmurphy@declangmurphy and Dr. Taplin's presentations later today.
I hope they present or ask what:
- the sexual function outcomes
- the incontinence rates
- the utilization of ART and SRT
- the information on true conventional MFS
- the reason they changed the endpoint and expanded the trial size (fairly obvious)
- data on PCSM and OS critically needed
End of the day I want patients to live life better. Lets make sure the data is presented and shared in a way we are confident this will happen.
Enjoy ASCO everyone!
9/n #ASCO26
In PROTEUS it is likely only a subset of MFS events were called based on PET, but unknown at this time breakdown:
-EFS: HR 0.71 (0.63-0.80); fairly modest relative benefit for a BCR driven endpoint; that is far above the STE to translate to an OS benefit.
-MFS (includes PET): HR 0.80 (0.67-0.96) exceeds the EFS STE as well as the 95%CI exceeds the ICECaP STE for conventional imaging MFS (ie STE is 0.81 and CI is 0.96).
End of the day the effect size is too small to confidently state it would later improve OS.
8/n #ASCO26
The largest issue with the PROTEUS trial is that it changed its primary endpoint of MFS by conventional imaging to now allow PET imaging. Without understanding the breakdown, they potentially changed it to effectively EFS.
We all know that adding ADT/ARPI should suppress PSA more effectively, which will delay BCR, which will improve EFS....but it has morbidity and does it help men experience life better or longer?
@US_FDA
7/n #ASCO26
You can see how in RTOG 9202 for example the DFS w/ conventional imaging translated to an OS benefit.
However, in POP-RT the huge improvement in MFS by PET did not have any impact on OS. Note the massive effect size in POP-RT MFS of 0.35 (almost at the STE for EFS) and still no signal for OS.
@Dr_RaviMadan@ChadTangMD@fabiomoraesmd@aleberlin2@JoshLangMD@AarmstrongDuke@Silke_Gillessen
6/n #ASCO26
This is the crux of the problem, MFS by PET closely mirrors EFS, and will certainly have a STE below 0.5.
Conventional imaging:
~50% of BCR events with conventional imaging result in positive scans.
- RTOG 9202 with 15+ yr fu: RT+LT-ADT: 45% had BCR at 15yr, but only 17% had DM.
PET imaging:
>95% of BCR events with PET result in positive scans.
-POP-RT w/ 5yr fu: WPRT+LT-ADT: Every BCR correlated to a +PET finding with 6 of the 7 BCR events having corresponding DM events. You can see the KM curves are nearly identical for BCR-free survival and MFS.
@VedangMurthy@DrHowardSandler@DrMHofman@jmmrad
🎥 Join @b_szabados & @PignotG at the Global Forum on GU Oncology!
💬 Dynamic discussions
🔎 Diverse perspectives
💡 Practical takeaways for daily practice
👉 Register now and join on Dec 2-5 in Amsterdam or online: https://t.co/Yi9Ts47p6Z
@OncoAlert #RENALC26 #BLADDR26 #PROSCA26
📣 SAVE THE DATE : 8-9 octobre 2026
Fort de la réussite de ses précédentes éditions, FOCUS s’impose comme un rendez-vous incontournable de l’onco-urologie française et internationale.
Cette année, FOCUS rencontre des experts suisses de renom 🇨🇭
👉https://t.co/4cUHVKBhYG
(Re)Découvrez @FocusMeeting : qualité du programme scientifique, experts nationaux et internationaux, toujours dans cette ambiance conviviale pour échanger sur nos spécialités !
https://t.co/LMpJx8j9lB
A l'année prochaine pour Focus 2026 meets Switzerland 🇨🇭🇫🇷