Visit our YouTube channel to learn more about the five risk factors for cardiovascular disease and strategies for blood-pressure control to reduce morbidity and mortality. https://t.co/j7ybkYcwkE
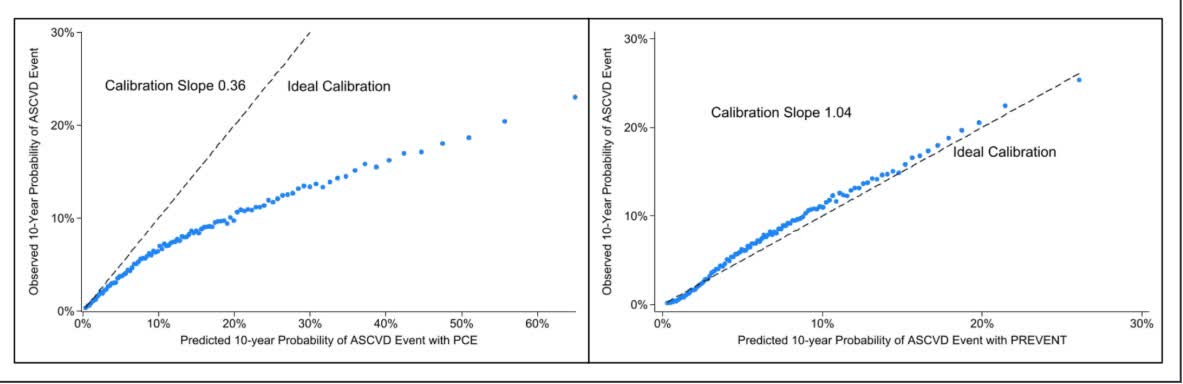
Among the Veterans' Health Administration (VHA), Predicting Risk of cardiovascular disease EVENTs (PREVENT) equation improves calibration and discrimination and can accurately predict 10-year ASCVD risk among Veterans https://t.co/iVM7jSA1DQ
It would be interesting to see what the same analysis would result in different subgroups, such as renal patients and/or hypertensive patients.
SGLT2s Best ARNIs in Frail, Older Adults With HFpEF https://t.co/A5mEiQk9NW
$NTLA News: Intellia announces positive longer-term data from the ongoing Phase 1 trial in #ATTRamyloidosis with polyneuropathy and the company’s latest publication in @NEJM. Read the press release: https://t.co/T94tQhVdEN
Cardio Town Hall: Amyloidosis is June 12, get prepared with NEW CardioBites+: Amyloidosis to learn the different mechanisms of disease and why understanding these differences may impact management decisions for these patients.
13-minute watch >> https://t.co/NibDuJmpaa
Knowledge is power, especially for your heart!🫀 Lipoprotein(a) [Lp(a)] is a genetic risk factor for heart disease & stroke. Identifying high Lp(a) levels early can help individuals take proactive steps to protect their #hearthealth.
📃Learn more: https://t.co/mhYVqPwG6o
Just published: 🫀Coronary Artery Calcium Scoring in the Context of Widespread Lipoprotein(a) Testing: Clinical Considerations and Implications for Lipid-Lowering Therapies🔬
🚨 New insights from Palanisamy, Burka & Blaha (2025) show Lp(a) & CAC aren’t just independent risk factors—they amplify each other! CAC exposes hidden atherosclerosis, while Lp(a) fuels thrombotic risk, making them essential first-line tests for primary prevention.
With Lp(a)-lowering therapies emerging, their role in high-CAC patients needs urgent study. Is CAC-guided Lp(a) therapy the future? #CVprev @foundationofnla@Heart_SCCT@MichaelJBlaha@rblument1@PalanisamySri@SBurkaMD
📖 Read more: https://t.co/UmGicUXJ6M
This picture is so profound. With 10 years of working in the ICU, there were several times when it felt like just because we can doesn’t mean we should. As one nurse put it “you’re slapping back the hand of Jesus” - the crocs are a nice added touch to the picture BTW
In our new study in EJPC, optimal CVD risk factor control was a/w lower risk across Lp(a) levels, though residual risk remains. These results show the importance of aggressive risk factor mgmt in patients with elevated Lp(a). @AlexRazavi@Lpa_Doc
https://t.co/PeVbyxErHz
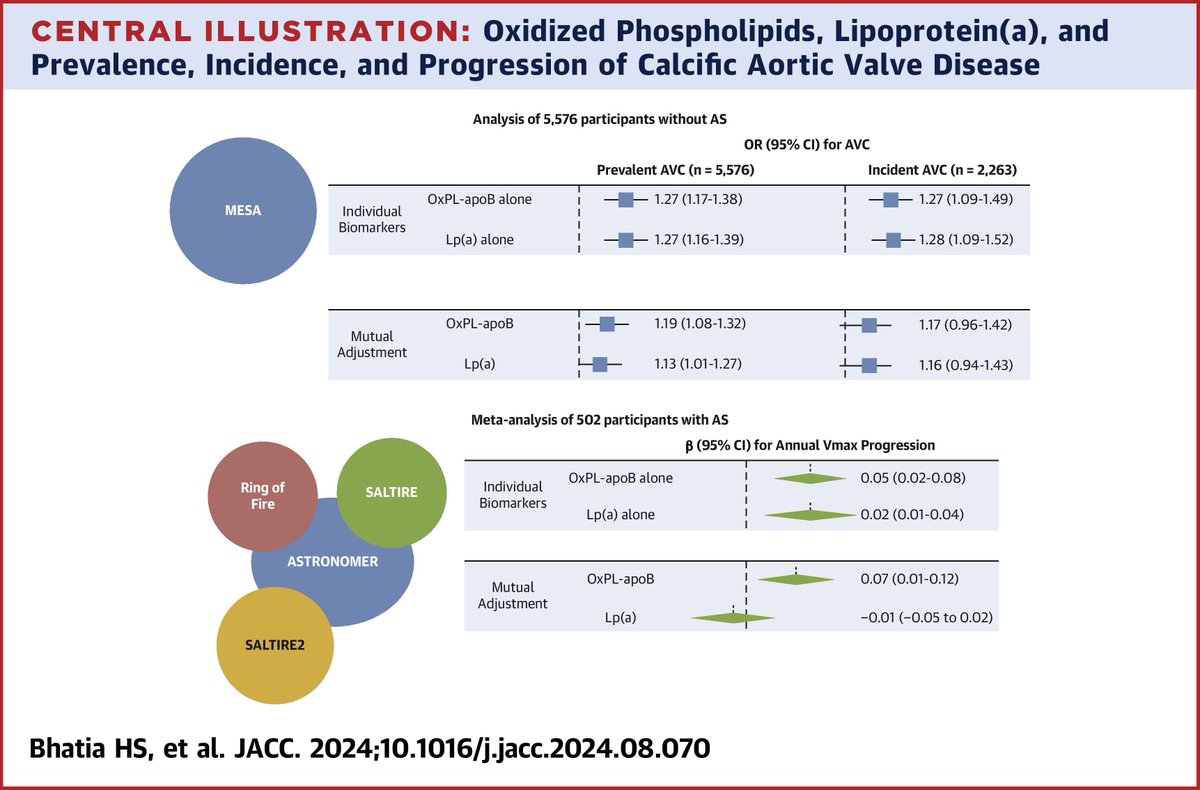
#AHA24 ICYMI: #JACC AE Dr. @MarcBonaca and Dr. @Lpa_Doc discuss new insights from the MESA cohort about OxPL-apoB and risk for calcific aortic valve disease 👇
📄: https://t.co/H57nhevvVf
#AHA24: How does OxPL-apoB affect the risk of calcific aortic valve disease? Using data from MESA, Drs. @hsbhatia, @Lpa_Doc & team show that ⬆️ OxPL-apoB is associated with increased incidence and progression of valve disease https://t.co/H57nhevvVf #JACC
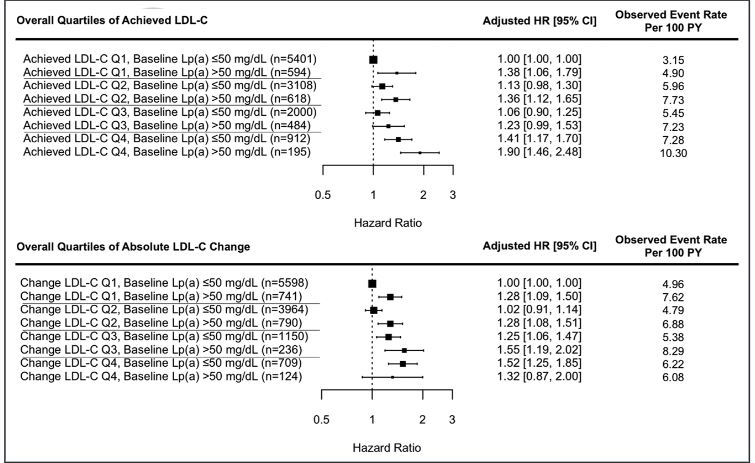
Lipoprotein, Lp(a) and LDL-cholesterol, LDL-C, are independent and additive for cardiovascular risk. Reduction in LDL-C cannot fully offset Lp(a)-mediated risk suggesting a need for targeted therapy for both. @PeterWilleit@hsbhatia@Lpa_doc https://t.co/fca9v6Ksoi
An estimated 1.19 million deaths per year could be prevented with optimal implementation of GDMT for heart failure with reduced ejection fraction globally. @GCFMD
https://t.co/hquWUNIYfD
Our new expert consensus document justifies why Indian and other South Asian patients at extreme ASCVD risk need to have LDL-C targets of 30 mg/dl and even lower to 10-15 mg/dl in those still suffering recurrent events.





























![foundationofnla's tweet photo. Knowledge is power, especially for your heart!🫀 Lipoprotein(a) [Lp(a)] is a genetic risk factor for heart disease & stroke. Identifying high Lp(a) levels early can help individuals take proactive steps to protect their #hearthealth.
📃Learn more: https://t.co/mhYVqPwG6o https://t.co/E7qScJRCR2](https://pbs.twimg.com/media/GkBYHavWsAAOn24.jpg)