Imagine if every passenger on an airplane had a direct line to the pilot.
That’s what medicine has become.
We have embraced frictionless communication and that not a good thing.
With things like Epic Chat, every member of the healthcare team has immediate access to the physician.
Now there’s a constant stream of minor questions. It’s discouraged people from thinking critically. “Just ask the doctor,” has replaced any sort of clinical reasoning.
When I was a resident, we had an answering service. Anyone who wanted to reach the doctor needed to go through a third party. This provided triage and accountability. If we were getting called in the middle of the night for stool softener orders, there was a record of that.
A little friction in communication is a good thing.
My Toolkit 🧰⚙️🪛: Self-made steerable catheter to cross the aortic valve in severe aortic stenosis
🔗https://t.co/ZFpZV7gDb6
In this article, @Obisht, Won-Keun Kim and Robert R. Flieger describe a self-made steerable catheter system using a 6F EBU guide and the stiff back end of a 0.035″ wire, combined with a hydrophilic straight-end crossing wire, to facilitate crossing of severely stenotic or calcified native or prosthetic aortic valves during TAVI.
The technique is particularly useful in horizontal aortas, bicuspid valves, and massively calcified tricuspid or bioprosthetic valves, where the conventional technique repeatedly fails.
Reviewed by Moritz Seiffert
#interventionalcardiology #CardioEd #cardioX
Admin: “we are rolling out Epic Chat!”
Doctor: “ok… how many messages will I be getting”
Admin: “only about 10-20 per hour, 24/7.”
Doctor: “oh… so I need to silence my notifications then”
Admin: “oh heavens no! Then you might miss that one message that is critical. And we will hang you out to dry if you do.”
Doctor: “what about when I sign into epic in my clinic”
Admin: “well that’s a different context for epic. So none of your messages will reach you until you log back into the hospital epic.”
Doctor: “but I’m still responsible for all the messages even when they don’t reach me?”
Admin: “bingo”
Huge thanks to the amazing team at @UChicagoMed
and the one and only Dr. Sandeep Nathan (@SandeepNathanMD) and the incredible team - Dr. Christopher Fernandez, Dr. Kunjan Udani (@KunjanUdani), Dr. Atman Shah (@ShahAtman), Dr. Jay Khambhati (@JKhambhati), Adaeze Emeka, and Kristen Hanauer, for a great Elevate™ case in the ELEVATE III HR-PCI Pivotal Study!
Onward to many more successes together❤️
The Elevate™ pLVAD is 10 Fr, delivered fully sheathed & fully over-the-wire into the LV, provides over 5.4 L/min of mean flow & over 8.4 L/min of peak flow. This year, we celebrate our dedicated medical teams participating in the ELEVATE III HR-PCI Pivotal Study.
#MagenaElevate #ElevatePump #SmallestpLVAD #ELEVATEIII #cardiotwitter
Heartbeat visualized.
A literal, "non-electronic" readout of the engine keeping you alive.
Your heart is literally just doing this all day every day and you don't even notice.
The preventable #death of my dear dad & the disturbing #UnspokenCurriculum shaped me to
- better listen to patients
- pay attention to details
- choose evidence over bravado
- err on the side of caution
- be truthful about mistakes
- forgive
#Lessons
https://t.co/vxkKTIeenh
I looked at Houston Methodist Hospital's IRS 990 filings and I genuinely don't understand what I'm reading.
This "nonprofit hospital" traded $9.3 BILLION in securities in 2021.
Their total patient revenue? $2.5 billion.
They traded 3.6x more in securities than they earned treating patients. 🧵
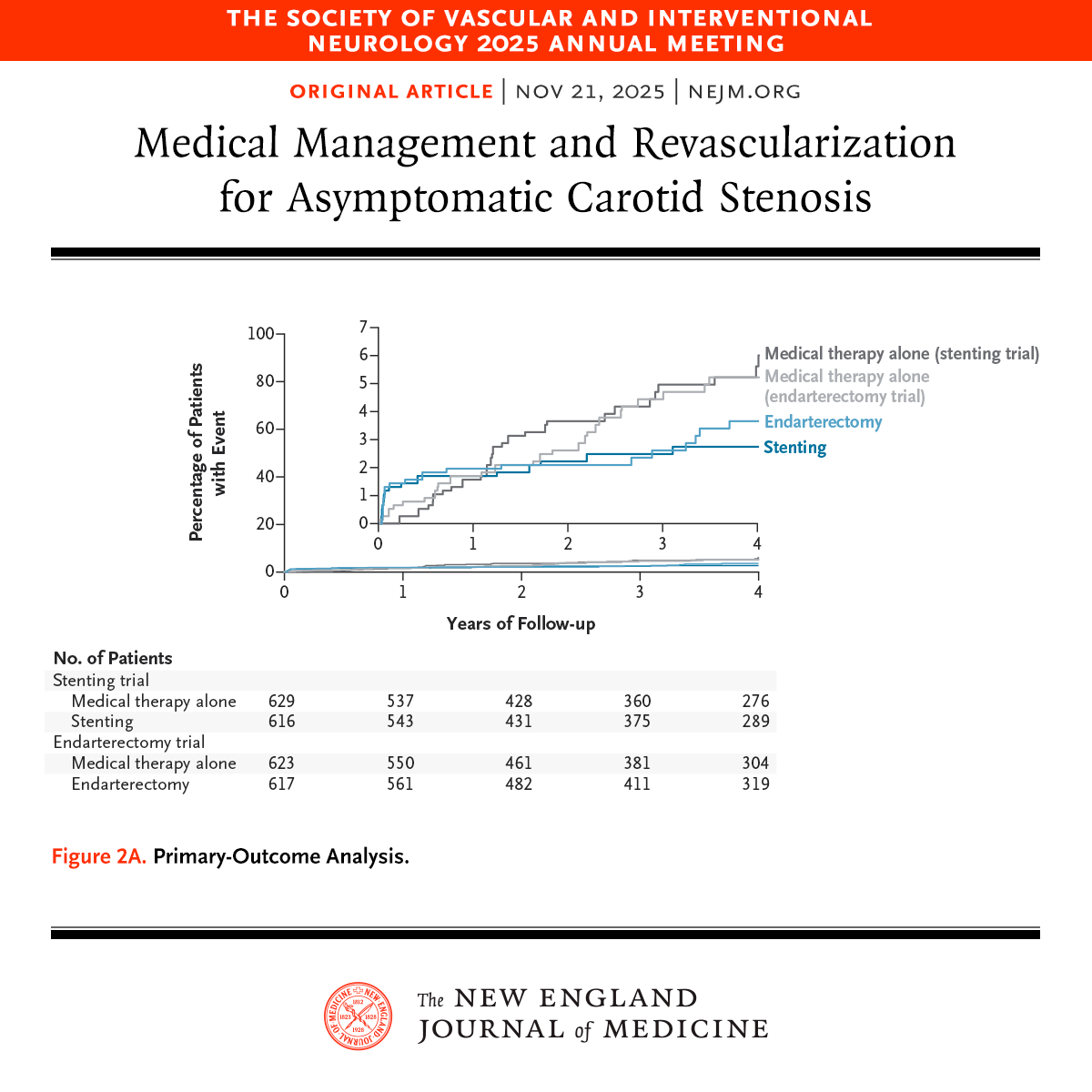
Presented at #SVIN25:
CREST-2: In high-grade asymptomatic carotid stenosis, addition of stenting to medical therapy led to a lower risk of stroke over a 4-year period. Endarterectomy did not lead to a significant benefit. Full results: https://t.co/ojge1CjqiU
Editorial: Managing Asymptomatic Carotid Stenosis https://t.co/D9LH89Edyk
@svinsociety
As redo-TAVI highlights constant under expansion of THVs, double TAP is likely to become the default strategy for both BEV and SEV. Better expansion, improved AR and hemodynamics, less pin-wheeling, better durability… Thoughts ?
https://t.co/ihQtUOp58P
@EuroInterventio@PCRonline
Provocative study from the RENOVATE trialists and Samsung Med Cntr suggesting use of intravascular imaging may eliminate long-term diffs between CABG & PCI. Not definitive absent a powered RCT, but should be enough to mandate IVI in these pts, esp with class I guidelines. Agree?
Remember when they tried to ‘ban’ surgeons caps?!
The AORN decided we all needed to wear lunch lady hats.
But then studies showed it made no difference.
Such a random and wild example nonesense in medicine where doctors get told what to do.
Post CABG Graft Failure Rates At One Year
These are the graft failure rates by conduit and treated vessel from a paper shared by @agtruesdell earlier today.
The numbers for combos listed in parentheses are small <50
Not likelihood ratios, but still food for thought!🤔