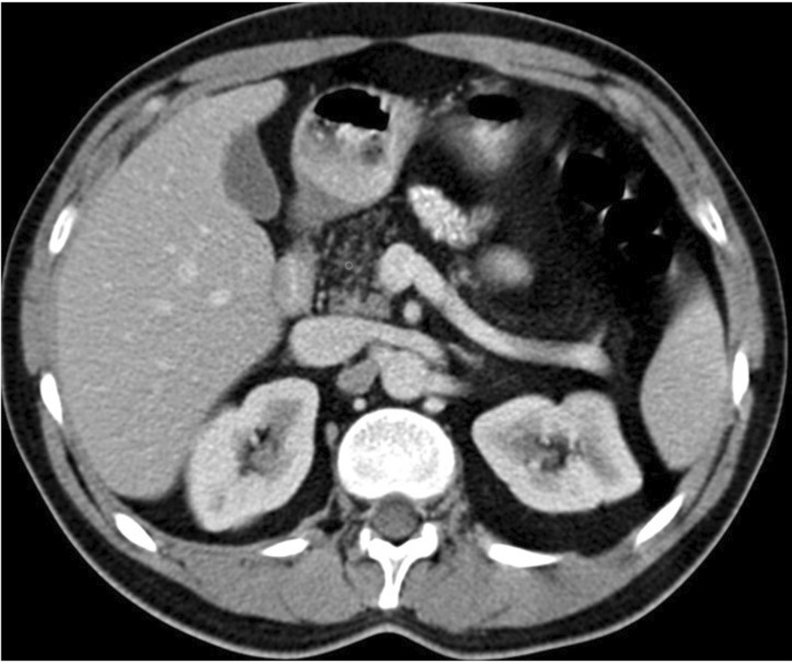
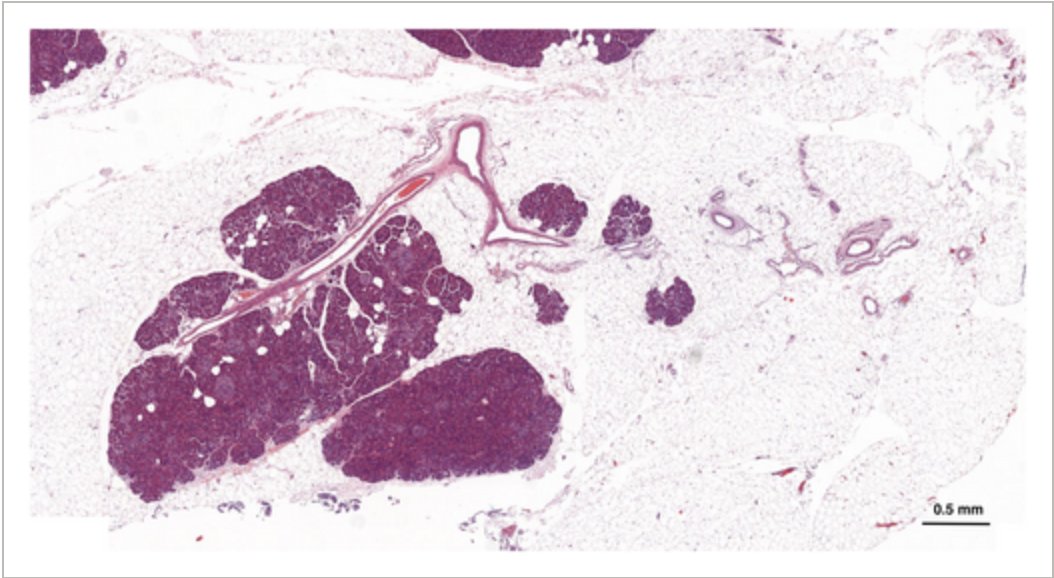
International Multidisciplinary 🤝 Consenus on #Fatty#Pancreas 🧈 is now published in @UEGJournal 🇪🇺
🚨 Fatty pancreas is associated with pancreatitis, metabolic disorders, and possible neoplastic changes
This landmark paper is 🆓 full access
https://t.co/dPJ1Tao5UL
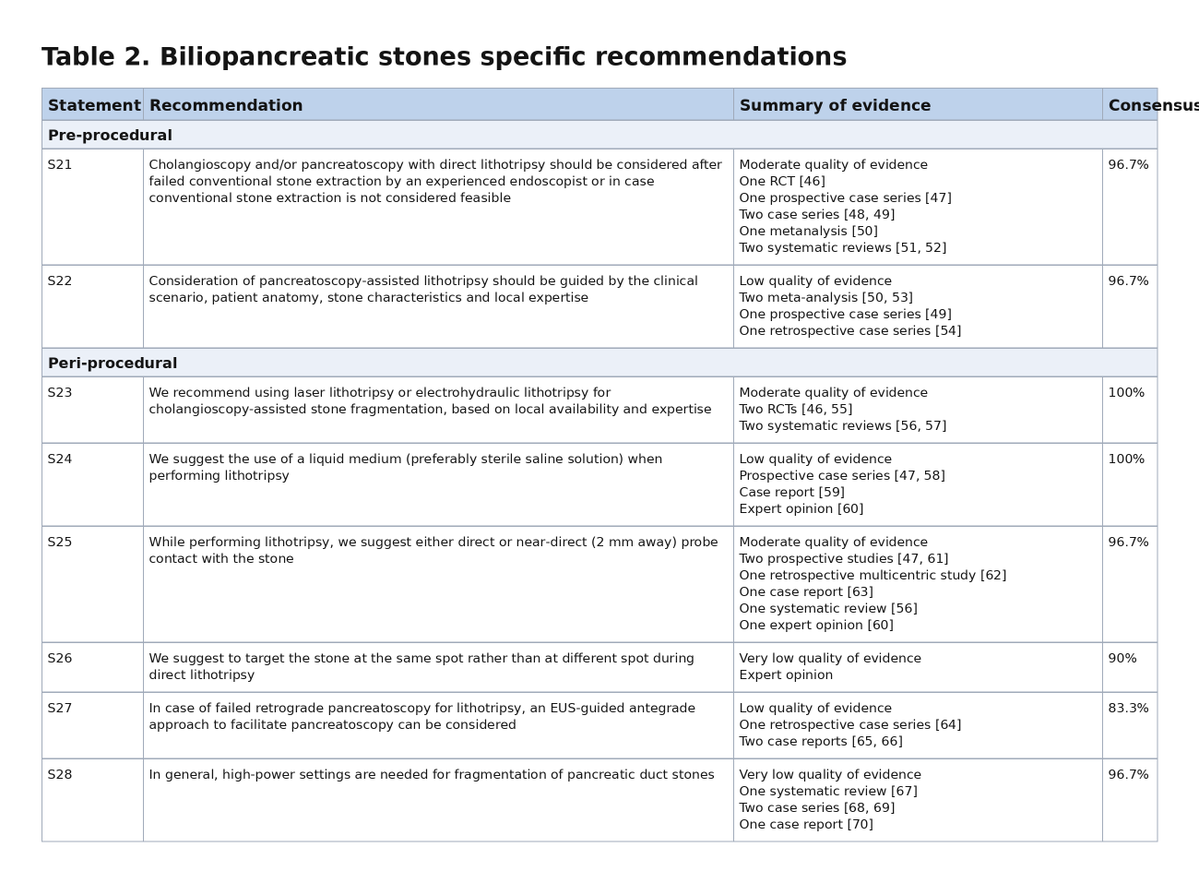
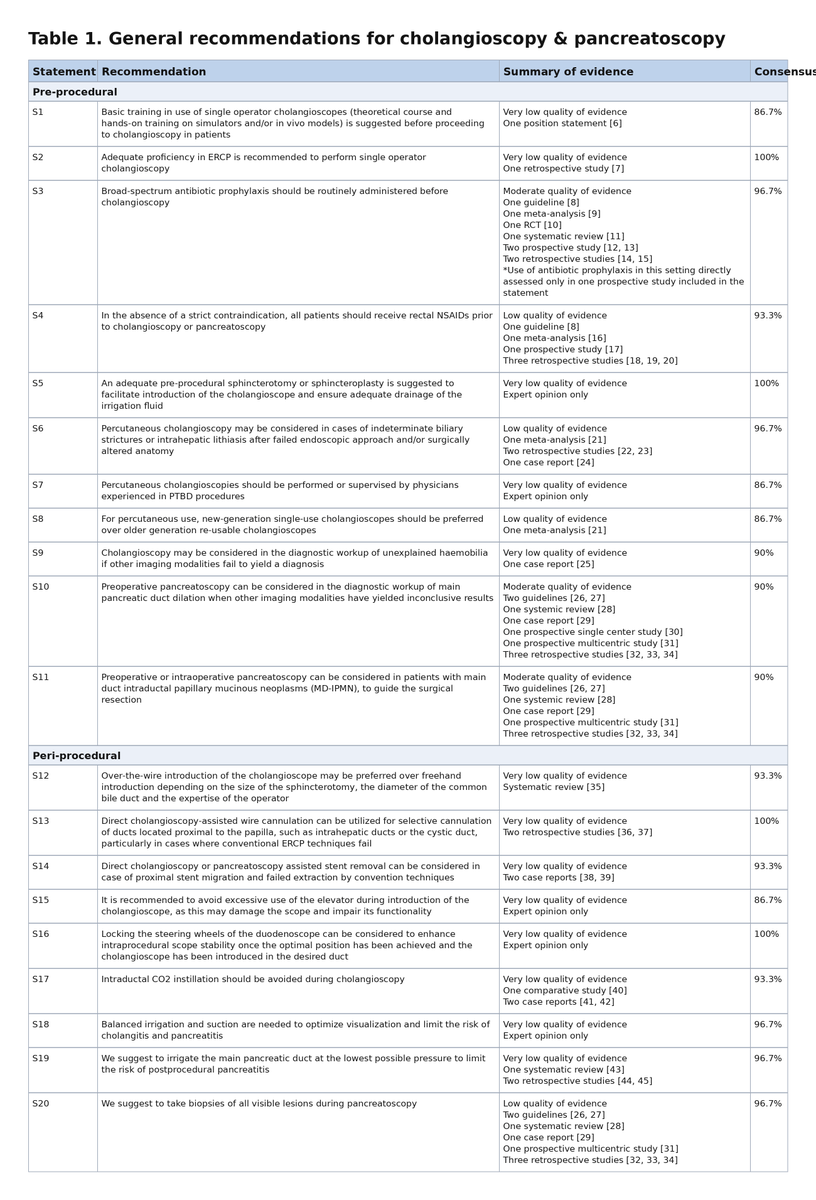
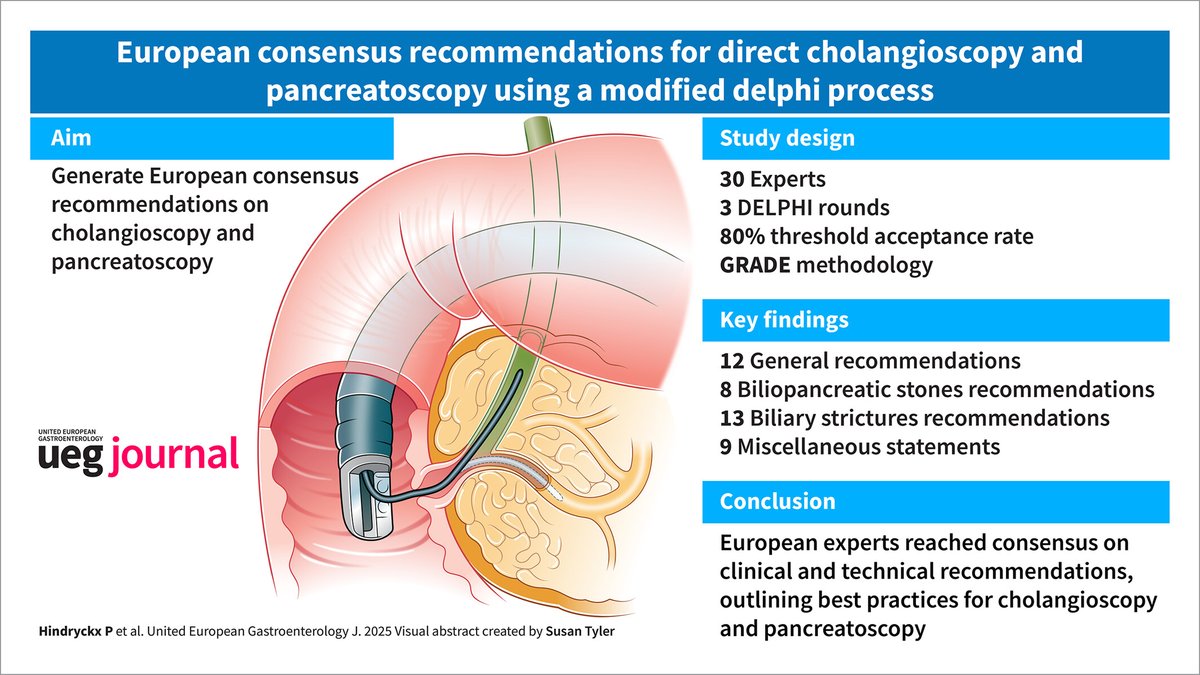
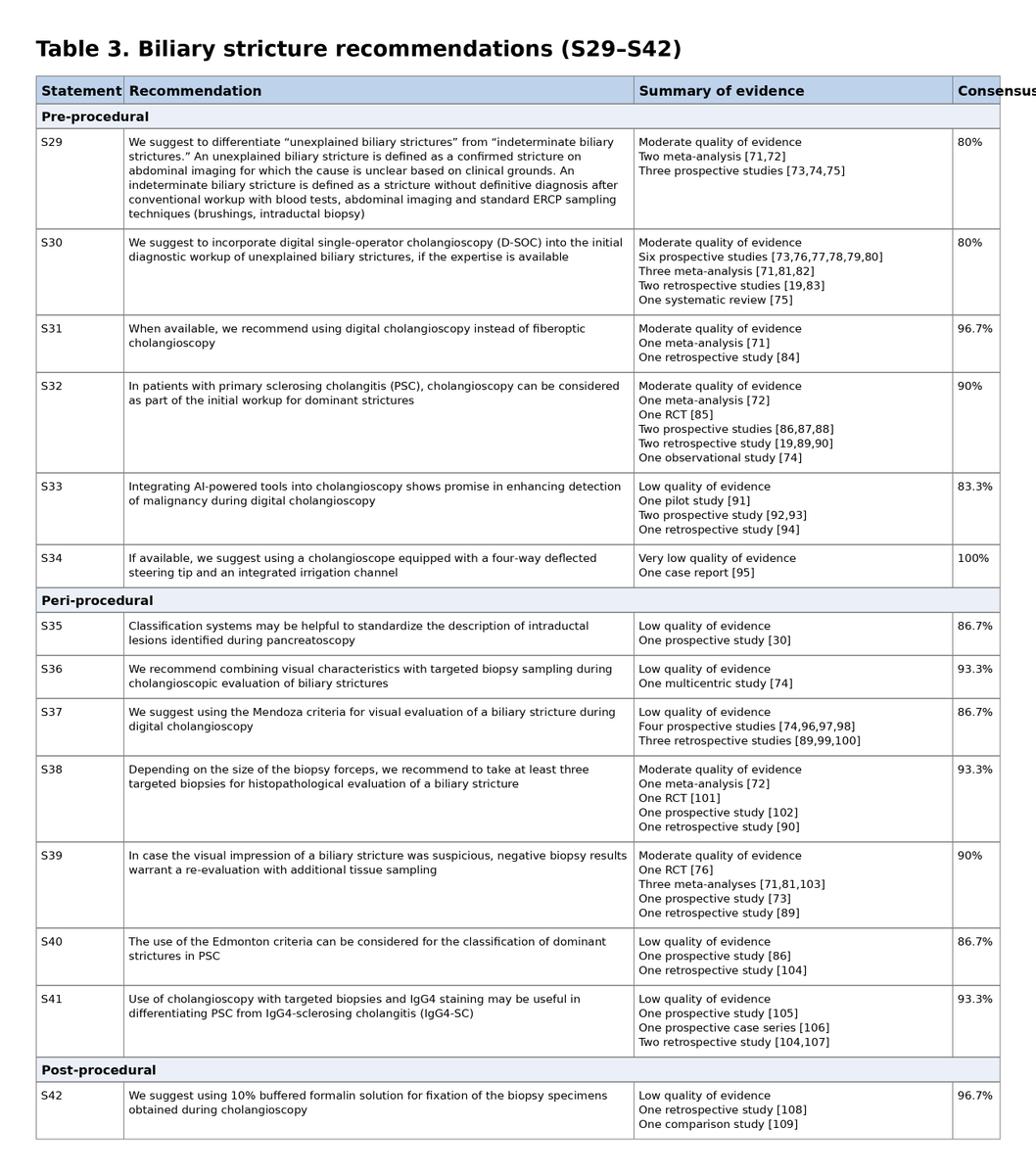
European Consensus Recommendations for Direct Cholangioscopy and Pancreatoscopy just for YOU:
🪩 42 recommendations at a glance
⬇️⬇️
🔗:https://t.co/0fSpATO7Wa
@my_ueg
Few Key Points on Management of Acute Variceal Bleed (APASL 2025)
•Time-Zero (T0) redefined : T0 = time of first hematemesis, not hospital arrival, to capture the entire pre-hospital course.
•AVB episode duration = 48 hours from T0 (not 5 days as in Baveno VII). Any bleed within these 48 h = same episode.
•“Home-to-Door” time :- ideally 2 hours (acceptable up to 4h in mild cases). Delay >4–6h increases mortality.
•CT scan recommended as a non-invasive diagnostic tool to assess esophageal varices; CECT superior to LSM/MRI for high-risk varices.
•Pre-ER (ambulance) management :- Terlipressin 2 mg bolus can be administered during transport in suspected AVB.
•ER: Start vasoactive agent early : terlipressin/somatostatin/octreotide within 30 min of index bleed (“door-to-needle” time).
•All vasoconstrictors have comparable efficacy in initial control of variceal bleeding. Choice based on availability and comorbidities.
•Prefer terlipressin in AKI :- physiologic benefit and better renal outcomes.
•Continuous terlipressin infusion (4 mg/24h) preferred over intermittent bolus :- higher success, lower dose, fewer complications.
•Tranexamic acid :- may reduce post-EVL ulcer bleeding but does not reduce mortality and carries risk of portal vein thrombosis.
•After endoscopic control, vasoactive drugs may be stopped after 48 h, and NSBB started thereafter.
•Antibiotics : Ceftriaxone preferred; duration can be shortened to 2 days if endoscopic hemostasis is successful (vs 5 days).
•If both EV and GV present, obliterate gastric varices first even if no stigmata of recent bleed on GV.
•Gastric varices bleed less often but more severely; can bleed even when HVPG <12 mmHg due to large blood flow causing rapid and profuse bleeding.
•Key TIPS points :-
•Rescue option for failure to control bleeding.
•Consider early TIPS in high-risk patients (hemodynamic and endoscopic predictors).
•Preferred rescue therapy for refractory GV or PHG bleeding when endoscopic or radiologic options fail.
•Antibiotics are not recommended for acute variceal bleed in non-cirrhotic portal hypertension :- no evidence available.
#GITwitter
اول مرة انزل فيديوهات لحالات اشتغلتها هنا، قلت تبقى فرصة اتكلم اكتر.
دي حالة جت بشتكي بعد عملية #تكميم بكزا سنة باعراض مذكورة في الفيديو وده اللي لقيته اثناء المنظار وكانت الحلول المتاحة للاسف كلها جراحية او محاولة التاقلم مع الادوية لانها Traumatized من اي جراحة اخرى …
Honored to attend the 2nd Egyptian Liver Transplant Conference (ELTS), led by Prof. Dr. Amr Abdelaal. A great platform to share insights & innovations in liver transplant with experts worldwide. Proud to be part of the Egyptian Liver Transplant Community! #LiverTransplant