🆕 #CardioPODCAST | Balón de contrapulsación intraaórtico: ¿sigue teniendo espacio en la UCIC?
🎙️ Ángel Hernández conversa con Pablo Antúnez, Pablo Pastor y Ana Viana sobre el papel actual del balón de contrapulsación intraaórtico en shock cardiogénico y los escenarios en los que puede seguir siendo útil frente a otras asistencias como Impella.
🎧 Escúchalo aquí: https://t.co/4PXmSkeyub
@AngelHdez13, @pjantunez, @Ana_Viana_T, @PolShepherd@AgudosSEC
📄 Can we finally measure RV volume accurately with simple echocardiography?
🔗 DOI: https://t.co/cHII0FgTLH
🫀 The right ventricle (RV) remains one of the most challenging chambers to assess—especially in congenital heart disease (CHD).
👉 Gold standard? Cardiac MRI
❗ But: expensive, time-consuming, and often requires sedation
✨ This study proposes a simple, fast, and accurate 2D echo-based method for RV volumetry—bringing us closer to true bedside quantification.
✨ The key idea:
👉 Model the RV using a cone-based geometric approach
➡️ Using only 2 standard echo views:
Apical 4-chamber (A4CH)
Parasternal short-axis (SAX)
📐 With just a few parameters:
✔ Cross-sectional areas (A4CH, ASAX)
✔ Tricuspid valve diameter
📊 Performance vs MRI:
🔥 Excellent agreement:
Systolic volume → ICC 0.98
Diastolic volume → ICC 0.96
📉 Minimal bias:
Δ systolic volume ≈ 0.1 mL
Δ diastolic volume ≈ 5.2 mL
➡️ Clearly outperforms traditional 2D models
💡 Why this matters clinically:
👉 Enables:
✔ Rapid bedside RV assessment
✔ Reduced need for repeated MRI
✔ Easier follow-up in paediatric & CHD patients
👉 Particularly valuable in:
Post-operative monitoring
Serial evaluations
Resource-limited settings
🚀 Key innovation:
👉 A mathematically robust yet practical model
➡️ Balancing accuracy + simplicity
➡️ Adaptable to different RV shapes
🚨 Bottom line:
2D echocardiography—when combined with smart modelling—can approach MRI-level accuracy for RV volumetry.
#Cardiology #Echocardiography #RightVentricle #CongenitalHeartDisease #CardiacImaging #CMR #Innovation #MedTech #PediatricCardiology 🫀📊
About that, I've got a query. Some centers consider counter-intuitive giving betablockers (as GDMT) soon after stabilization of HF-CS even if patients are receiving dobutamine but some of them still do it. Is not that down-regulation a limit for the beneficial effect of bblock? 🤔
Congratulations to the leadership and members of the Society of Critical Care Cardiology (SoCCC) on the publication of this important new scientific statement in the American Heart Association🫀
This statement proposes a practical framework for CICU admission decisions grounded in the potential benefit of critical care therapies and monitoring, patient goals of care, and the risk of early adverse cardiovascular events across common cardiovascular conditions. The work represents an important step toward more patient-centered, evidence-informed, and resource-conscious cardiovascular critical care.
Read the statement here: https://t.co/bZSGPBzwRE
Congratulations to the outstanding leadership involved in advancing the field of critical care cardiology:
@seanvandiepen@AnnGageMD@AdrianaCLuk@PennyRampersad@garimadahiyamd@ChrisBarnettMD, @carlosalviar, @emilyzernMD, Erin Bohula
#CriticalCareCardiology #Cardiology #CICU #CardiovascularCare #AHA #SoCCC #CriticalCare #HeartHealth
🔍 Volumen de casos en centros ECMO y mortalidad en el shock cardiogénico por infarto de miocardio
Juan Martin Hurtado Felipe @_JMartinHF
Lee el análisis completo y descubre qué factores marcan la diferencia en la supervivencia: https://t.co/e6FKsDkrmo
💔 La mortalidad a 30 días en pacientes con shock cardiogénico tratados con ECMO fue significativamente mayor en centros de bajo volumen frente a los de alto volumen (63,1% vs 40,3%), diferencia que se mantiene al año de seguimiento.
📊 En el análisis multivariado, los centros de bajo volumen mostraron hasta el doble de riesgo de muerte a 30 días en comparación con los de alto volumen (HR: 2,16; IC95% 1,47–3,17).
🏥 Los centros de bajo volumen presentaron menor uso de acceso radial, mayor tiempo hasta la ICP y mayor necesidad de terapia de reemplazo renal, factores que podrían contribuir a los peores resultados.
⚠️ Los hallazgos sugieren que la experiencia del centro en ECMO —y en el manejo integral del paciente crítico cardiovascular— es un factor determinante en la supervivencia tras el soporte circulatorio mecánico.
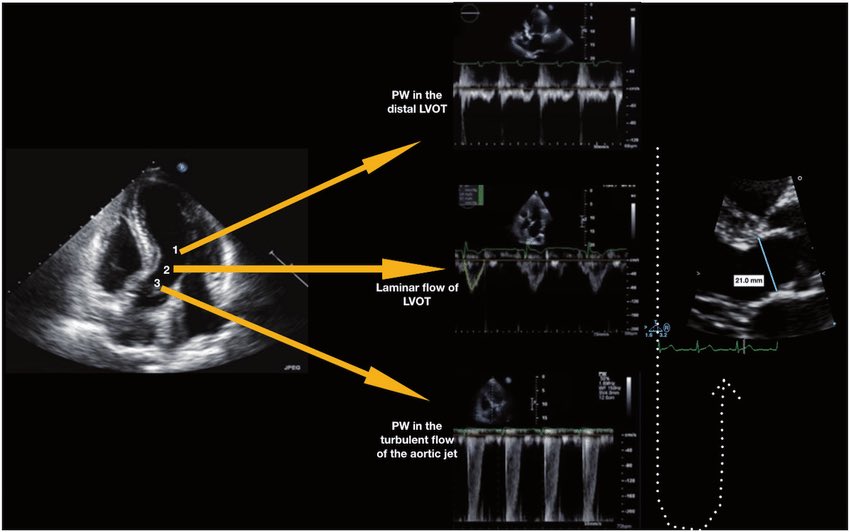
🫀 Did you know where the recommendation to place the pulsed wave Doppler sample volume 0.5–1 cm from the aortic valve to measure LVOT VTI comes from?
The answer is more interesting than it seems. It doesn’t come from a single study or an experiment designed for that purpose. It comes from a historical chain spanning nearly 40 years:
🔬 1982–1984 — The physical foundation
Pasipoularides and Murgo demonstrated using invasive catheters and mathematical models that in aortic stenosis there is a real zone of flow acceleration in the LVOT, just proximal to the valve, without any second anatomic obstruction. Pure hemodynamics — no Doppler yet.
👉 Bird et al. Circulation 1982 → https://t.co/oCXGNgWsPF
👉 Pasipoularides et al. Am J Physiol 1984 → https://t.co/cfvNMpEgzG
📐 1984 — The apical 5-chamber view
Lewis, Kuo and Quinones were the first to validate cardiac output measurement using pulsed wave Doppler from the cardiac apex. They described placing the sample volume “immediately proximal to the aortic valve leaflets” — but without specifying any distance in centimeters.
👉 Lewis et al. Circulation 1984 → https://t.co/lRVjLuYMEs
📏 1985 — The first numerical distance
Skjaerpe, Hegrenaes and Hatle (the Norwegian group) were the first to quantify this in Doppler: they empirically observed that flow acceleration began 0.5 to 1.5 cm proximal to the valve, and placed the sample volume just proximal to that zone. They directly cited Pasipoularides as supporting evidence. This was the first time a numerical distance appeared in the technique.
👉 Skjaerpe et al. Circulation 1985 → https://t.co/rf7l2FQUs4
📊 1986–1988 — Practical consolidation
Otto et al. used ~1.0 cm. Oh, Tajik and the Mayo Clinic group explicitly established the range of 0.5 to 1.0 cm in 100 patients, justifying it as necessary to avoid the subvalvular acceleration zone. This is the figure we all recognize today.
👉 Otto et al. JACC 1986 → https://t.co/avke1qOy4x
👉 Zoghbi et al. Circulation 1986 → https://t.co/KFiChfBNuc
👉 Oh et al. JACC 1988 → https://t.co/1C8sHRSMPq
📋 2002 — It becomes “official”
Quinones, Otto, Zoghbi and colleagues codified it in the ASE guidelines as “~5 mm proximal to the aortic valve”… but without citing any specific study to support it. It had already become expert consensus.
👉 Quiñones et al. JASE 2002 → https://t.co/U3hXFns4jx
⚔️ 2017 — The debate reopens
Baumgartner et al. (EACVI/ASE) maintained the 0.5–1 cm recommendation. However, Hahn and Pibarot responded with a critical letter pointing out that the original articles from the 1980s measured at the aortic annulus, not 0.5–1 cm below it, and that moving away from the annulus introduces errors due to the elliptical and irregular shape of the subannular LVOT.
👉 Baumgartner et al. Eur Heart J Cardiovasc Imaging 2017 → https://t.co/iu07xBTwQS
👉 Hahn & Pibarot. JASE 2017 → https://t.co/uqgcv8kzO7
💡 Bottom line:
The 0.5–1 cm figure was never experimentally validated as the optimal distance. It emerged from empirical observations in the 1980s aimed at avoiding a flow acceleration zone that had been demonstrated with invasive catheters. It was adopted through accumulated clinical practice and later elevated to a formal recommendation by consensus. The debate over whether to measure at the annulus or 0.5–1 cm below it remains open to this day.
One of those recommendations we all follow but few know where it actually came from 🙂
Dr Benigno Valderrábano Salas
@MDBeni@JaeKOh2@ottoecho@WilliamZoghbi@ASE360@EACVIPresident@NephroP@iamritu@PPibarot@hahn_rt@MAecocardio@SISIACOficial@SONECOM_AC@VazyurVasquez@Cardiotweets83@HEARTof_echo@echobasics
@IM_Crit_ for that RV is "always fluids-dependent "misconception, once I've seen a RV infarction complicating inferior STEMI with RA pressure of 21mmHg 🤯🤯receiving levophed 12ug/min (Watch the septal flattening! 😢). She got better with furosemide and dobutamine (obviously revasc👌)
I share this night-shift case! @IM_Crit_@ThinkingCC 57 yo 🧍♂️ with PMH of NSTEMI revasc w/ DES (2), HTN and obesity. He's being treated for ADHF with lasix and NTG. Vitals: HR 105, PA: 150/60. ABG: mild hypoxemia with 2L NC. Exam: apical systolic murmur. Bedside echo show this:
We stopped lasix and tach started to solve. Patient had apneic episodes with O2 desaturation during sleep which worsed BP ( 🤔OSAS probably). Pulsus paradoxus was seen but we decide to start fluids and continue amlo with improvement. Cardiology isn't always diuresis!! Thanks 😀
Se anunciaron las medallas de Perú en la Olimpiada Europea de Matemática para Mujeres en Francia! Dhámaris Alarcón obtuvo una medalla de oro🥇y Faviana Esteban una medalla de bronce🥉
Esta olimpiada es la competición matemática femenina más prestigiosa del mundo. Qué orgullo! 🇵🇪
Sesgos cognitivos
#AventhoAnestesia#Aventho#SMMCE#SAML
Claro, pero el problema no es el paciente… es que la evidencia está mal.
Porque si siempre lo hemos hecho así, ¿por qué cambiar? 🙃
Total, el sesgo de anclaje solo es “experiencia clínica”, la confirmación es “criterio”, y el status quo es “prudencia”.
¿Actualizarse? Para qué, si ya tengo mis verdades absolutas desde la residencia.
— “Seguro es EPOC, fuma”
— “Es ansiedad, como siempre”
— “Ya encontré algo, no necesito buscar más”
Pero no, eso no son sesgos… es ojo clínico
Mientras tanto
🔴 Diagnósticos incompletos
🔴 Errores que se refuerzan solos
🔴 Innovación frenada
🔴 Pacientes pagando el precio
Y el clásico
“Todos lo hacen así” → falso consenso nivel experto
“Yo no cometo errores” → punto ciego certificado
“Ve las cosas que ese está haciendo, no sabe” → status quo
La medicina no se estanca por falta de evidencia…
se estanca por exceso de ego
Actualizarse no es opcional
Cuestionarse tampoco
Porque el cateter de arteria pulmonar no es una terapia sino es el comienzo para decidir qué terapia recibirá. Esto se correlaciona a lo evaluado por el CCCTN en USA. Felicidades! @Jorgeheartshock
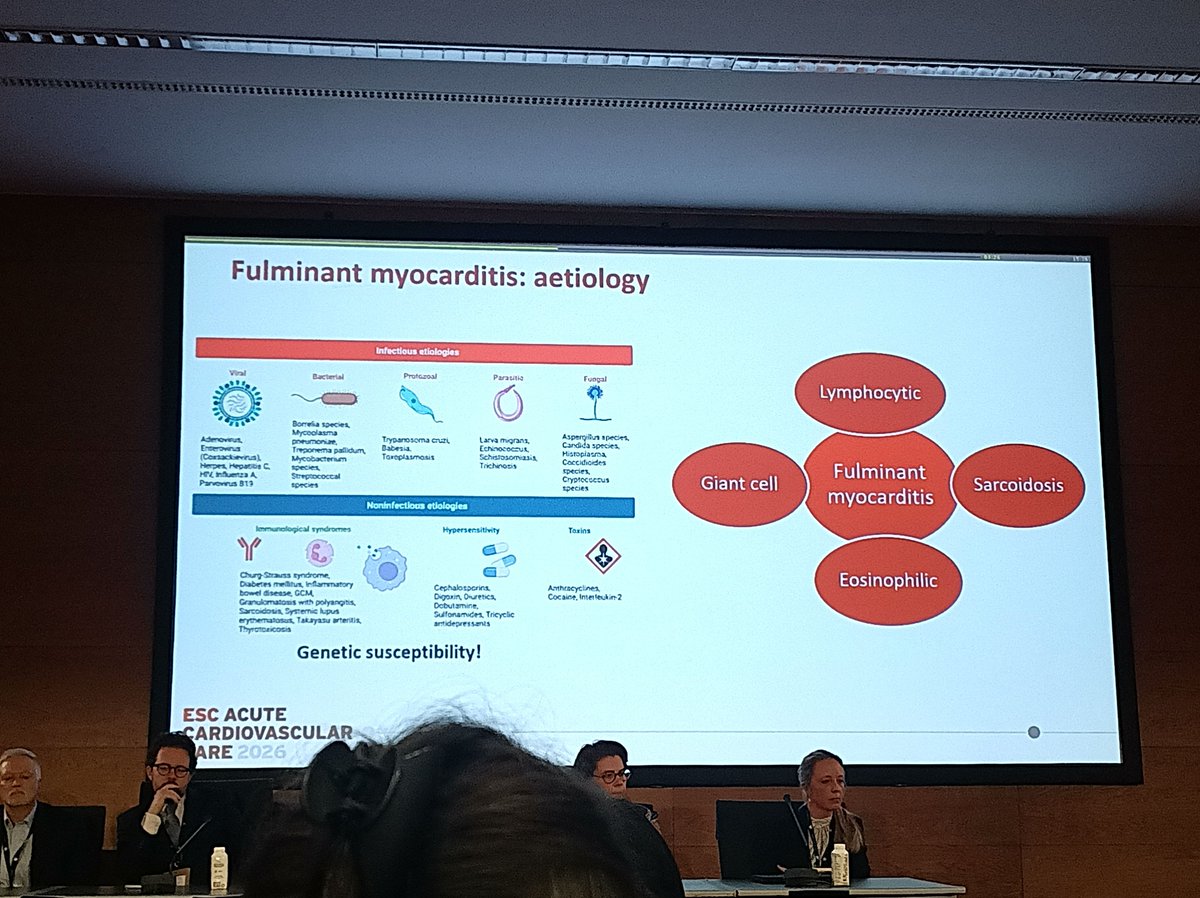
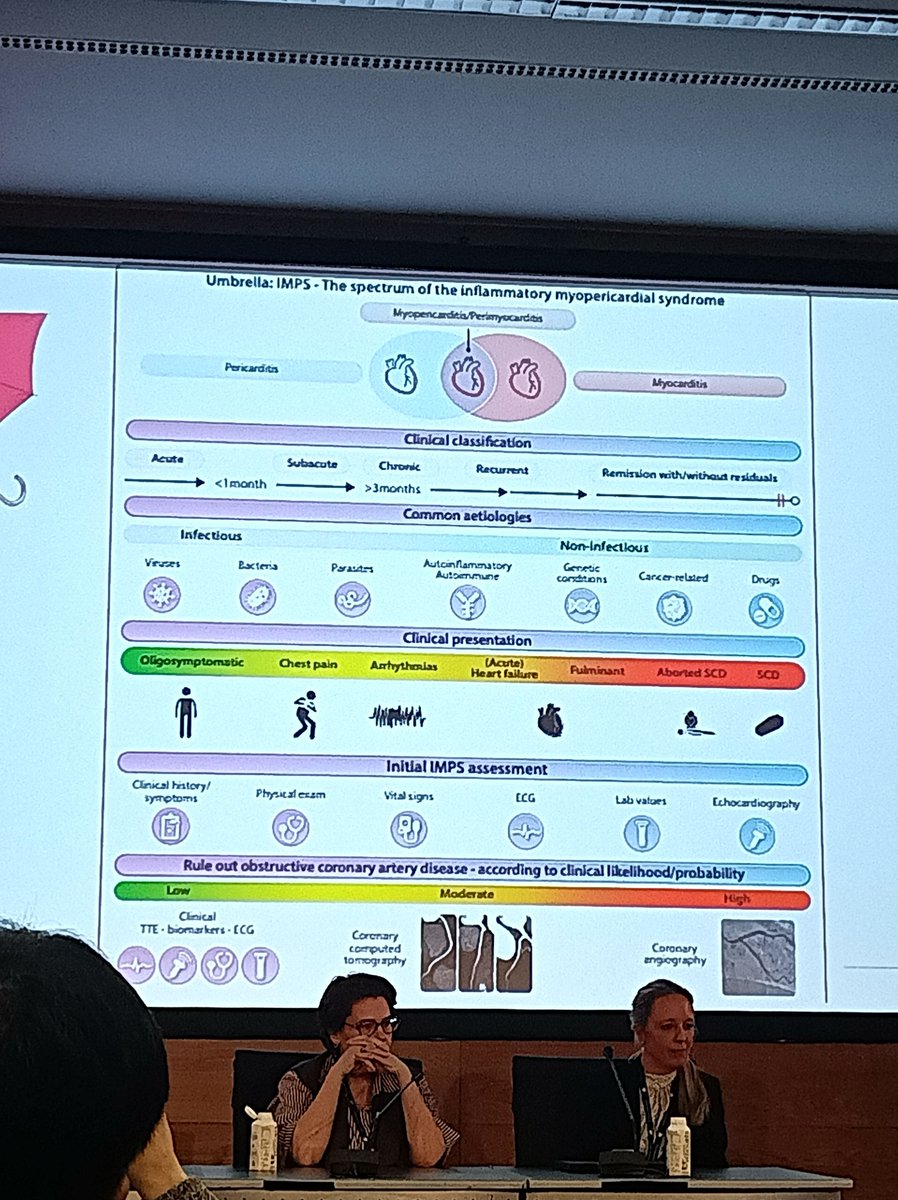
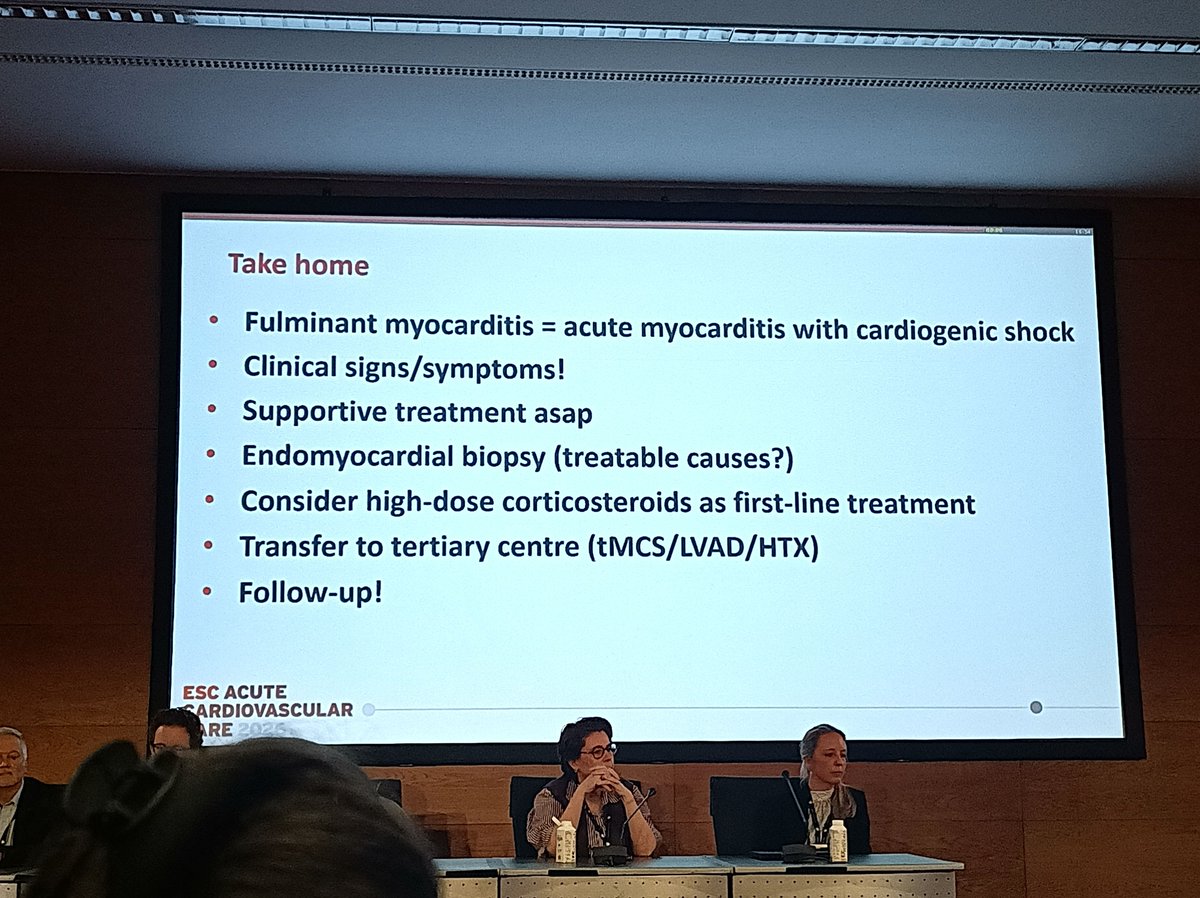
📍 ACVC 2026 Highlights | Acute Myocarditis.
Acute myocarditis remains one of the most unpredictable conditions in acute cardiovascular care.
From oligosymptomatic cases to fulminant cardiogenic shock, early recognition and risk stratification are critical.
🔑 Key takeaways:
• Acute myocarditis = symptoms ≤ 4 weeks
• Fulminant myocarditis = hemodynamic instability requiring inotropes or mechanical support
• High risk features: Cardiogenic shock
Malignant arrhythmias
Advanced AV block
LVEF < 40%
• Most cases are benign
But: ≈ 25% complicated
≈ 8% fulminant
High short-term mortality in severe forms
• Endomyocardial biopsy: Useful for identifying treatable causes
Still limited by sampling error and procedural risk
• Management priorities: Early recognition
Shock team activation
Rapid escalation to mechanical circulatory support
• Selected cases: High dose corticosteroids as first line therapy.
👉 Bottom line: Think myocarditis early in unexplained shock
Act fast
Involve the right team
#ACVC26 #Cardiology #CriticalCare #CardioICU #Myocarditis #CardiogenicShock #AcuteHeartFailure #MechanicalCirculatorySupport #HeartFailure #Hemodynamics #MedicalEducation