La especialista del Chuac advierte acerca de los riesgos de exponerse al sol en una época del año en la que todavía la percepción del peligro es menor que en pleno verano
https://t.co/zmynWuufQm
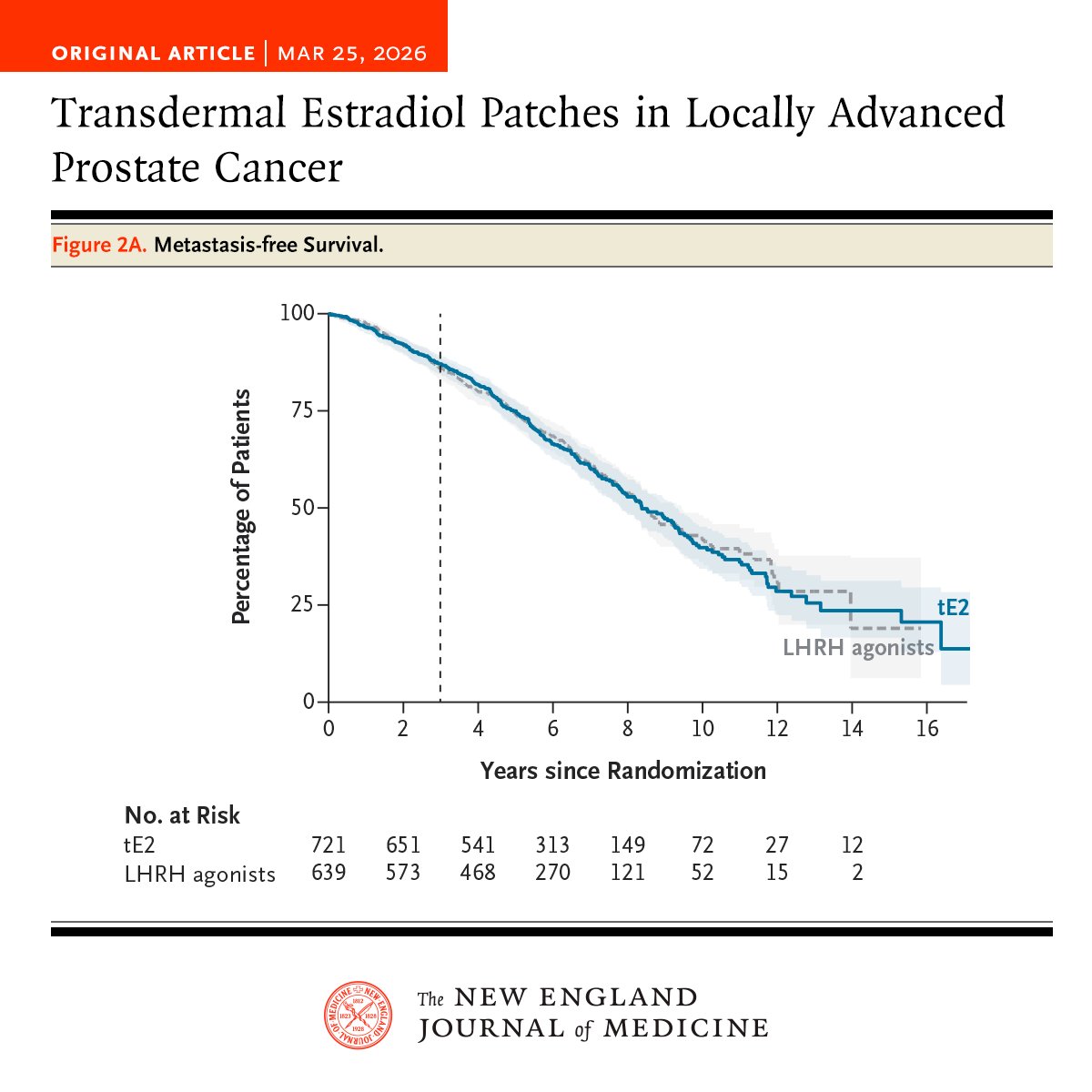
Among men with locally advanced prostate cancer, transdermal estradiol was noninferior to LHRH agonists for 3-year metastasis-free survival and led to a lower incidence of hot flashes but a higher incidence of gynecomastia. Full results of the STAMPEDE-1 and PATCH trials: https://t.co/sKJ6Sr6WiW
⚡️ New SITC clinical practice guideline (v3.0) on immunotherapy in RCC: practical recommendations across adjuvant + metastatic settings, special populations, response monitoring, and QoL.
Key reminders: PD-L1/TMB/MSI don’t guide selection; sarcomatoid features favor IO—nivo/ipi remains a preferred option.
#KidneyCancer #RCC @crisbergerot@OncoAlert
https://t.co/oDPnQzWxK8
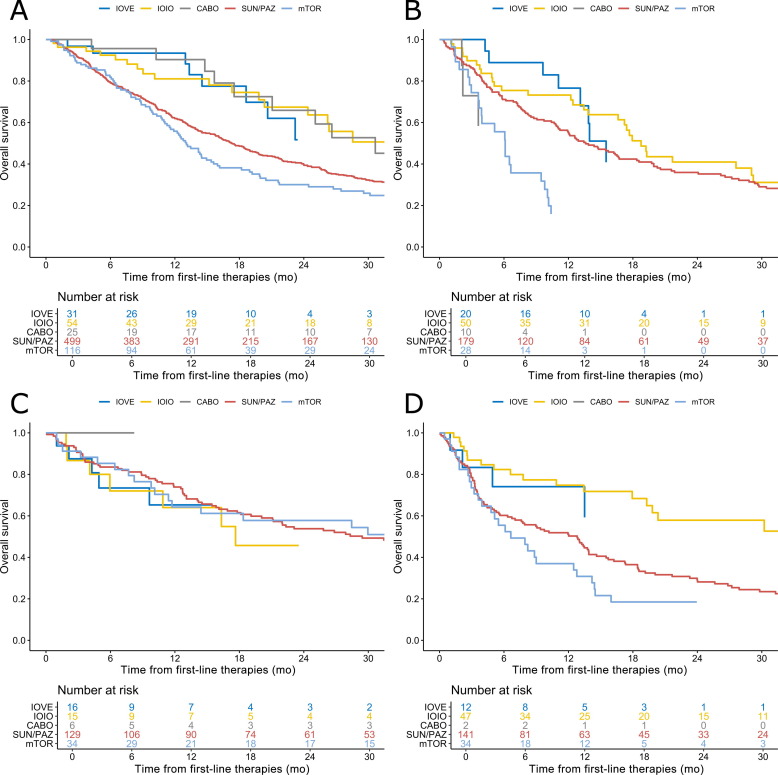
⚡️ IMDC real-world (n=1,551) metastatic non–clear cell RCC: 1L IO+VE, IO-IO or cabozantinib showed higher ORR and longer OS vs sunitinib/pazopanib or mTOR—but the benefit varies by histology.
Papillary: ORR 31–37% & OS ~31–33 mo with contemporary regimens vs 13% & 17.2 mo (SUN/PAZ).
Sarcomatoid: IO-IO had the best outcomes (ORR 39%, OS 31.9 mo).
#KidneyCancer #RCC
https://t.co/pnq1CGC6Wr
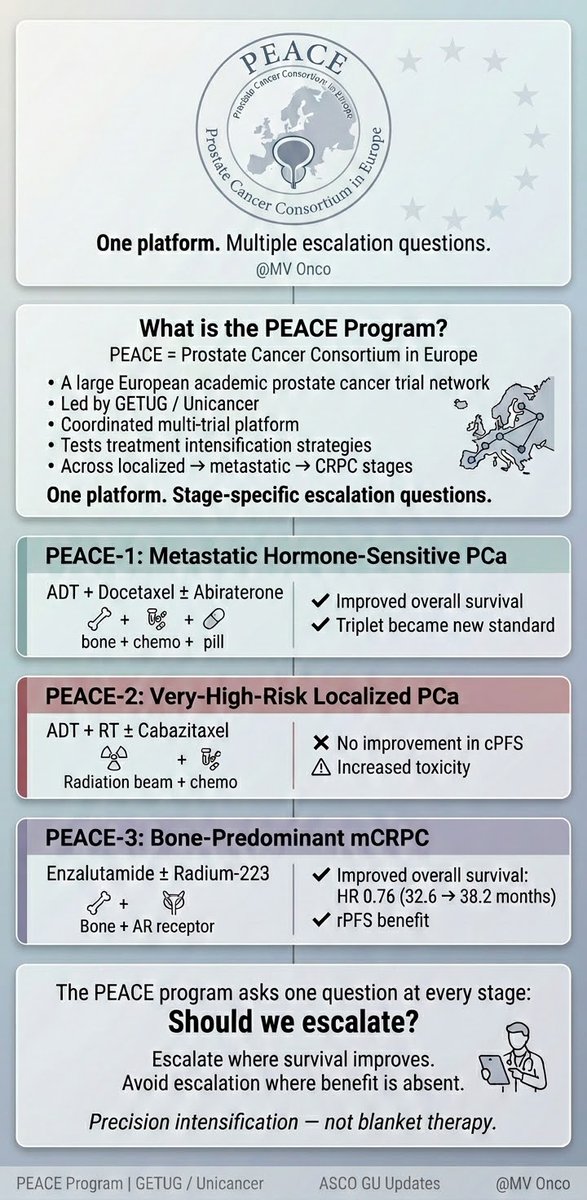
PEACE Program explained 👇
• A European prostate cancer trial platform
• Tests escalation at every disease stage
• PEACE-1 → Escalation improved survival
• PEACE-2 → No benefit, more toxicity
• PEACE-3 → OS benefit in bone-predominant mCRPC
#ProstateCancer#ASCOGU#MVOnco
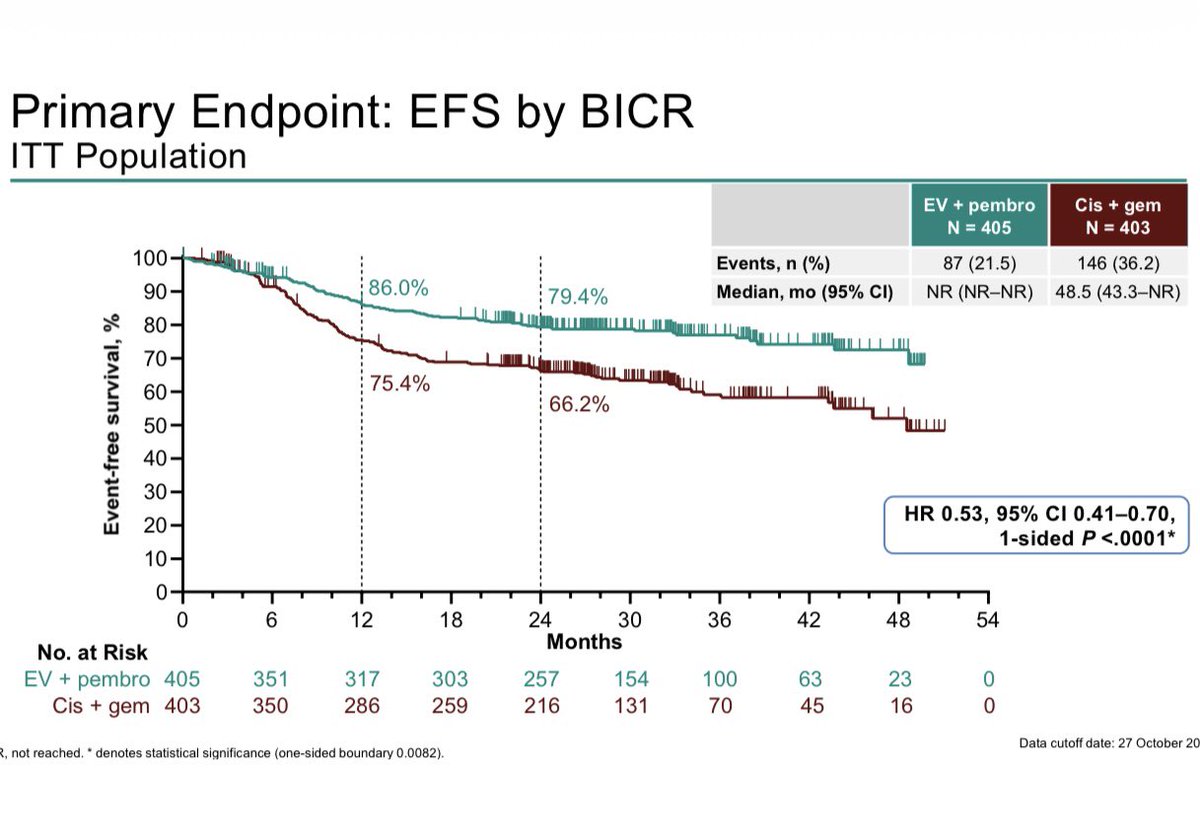
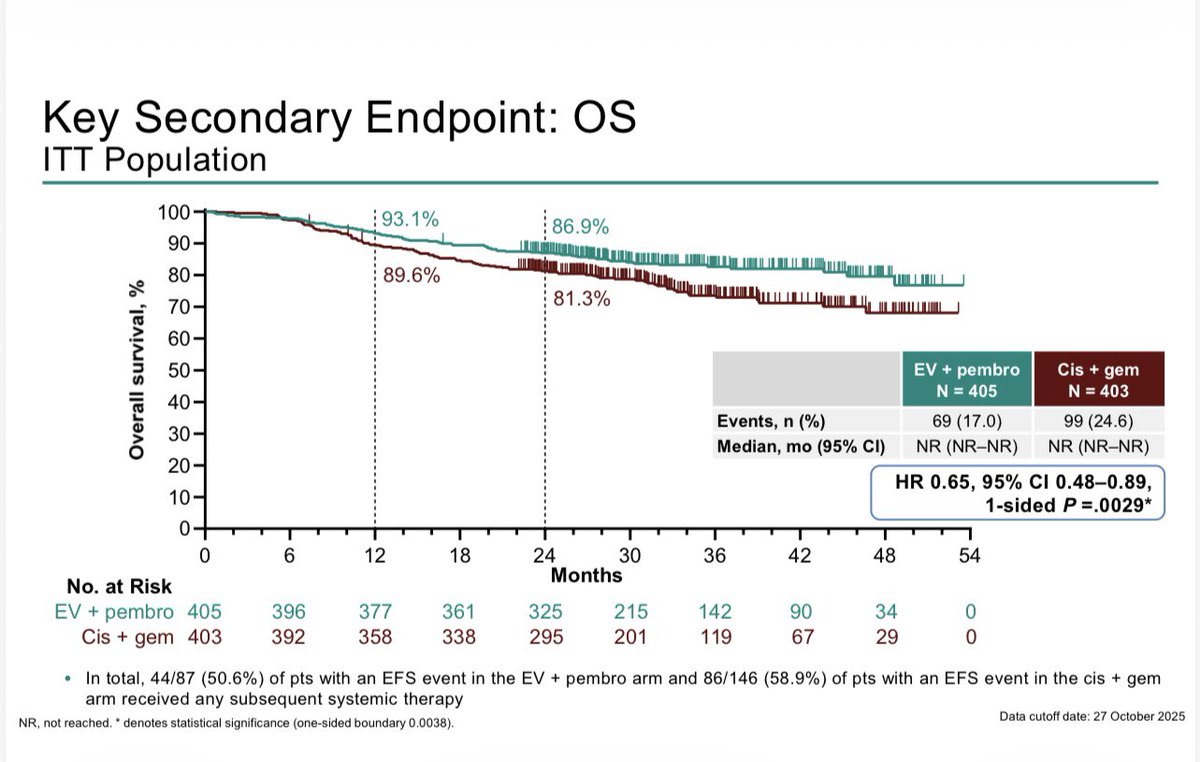
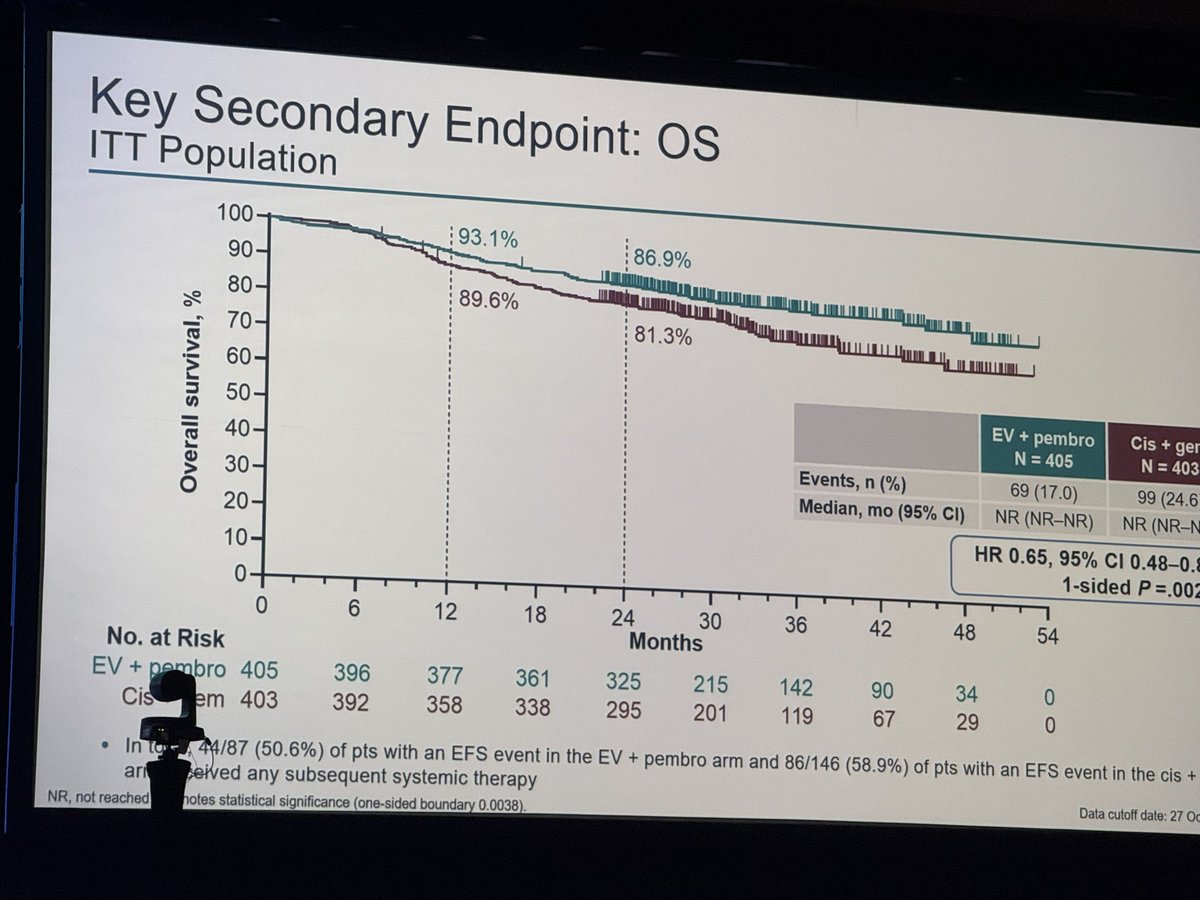
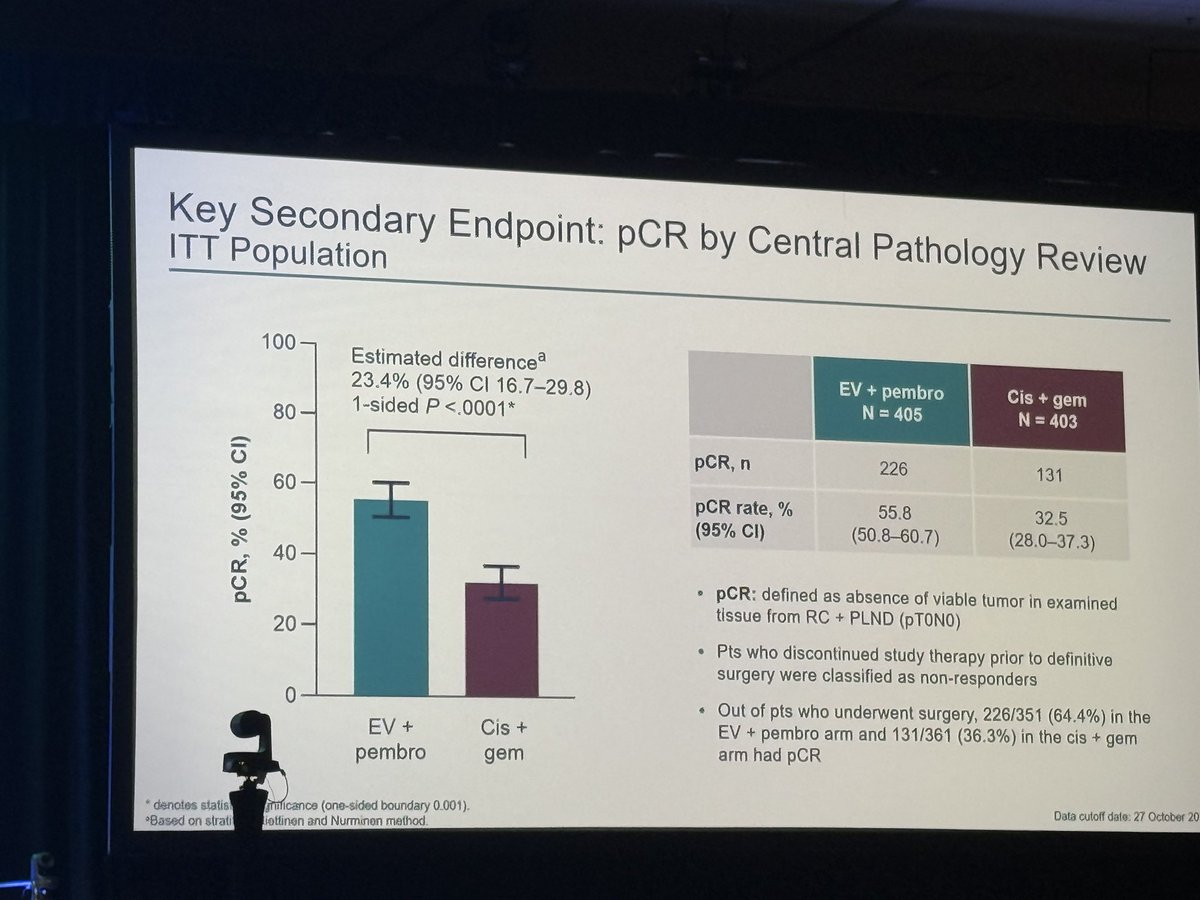
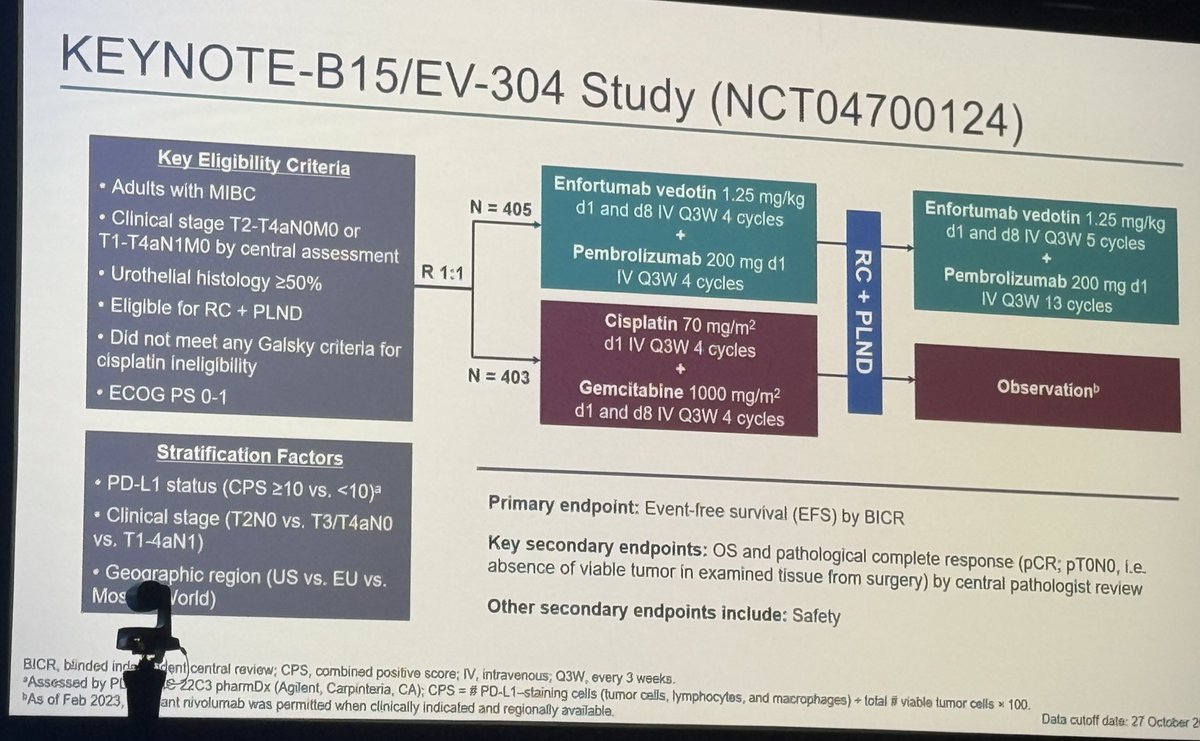
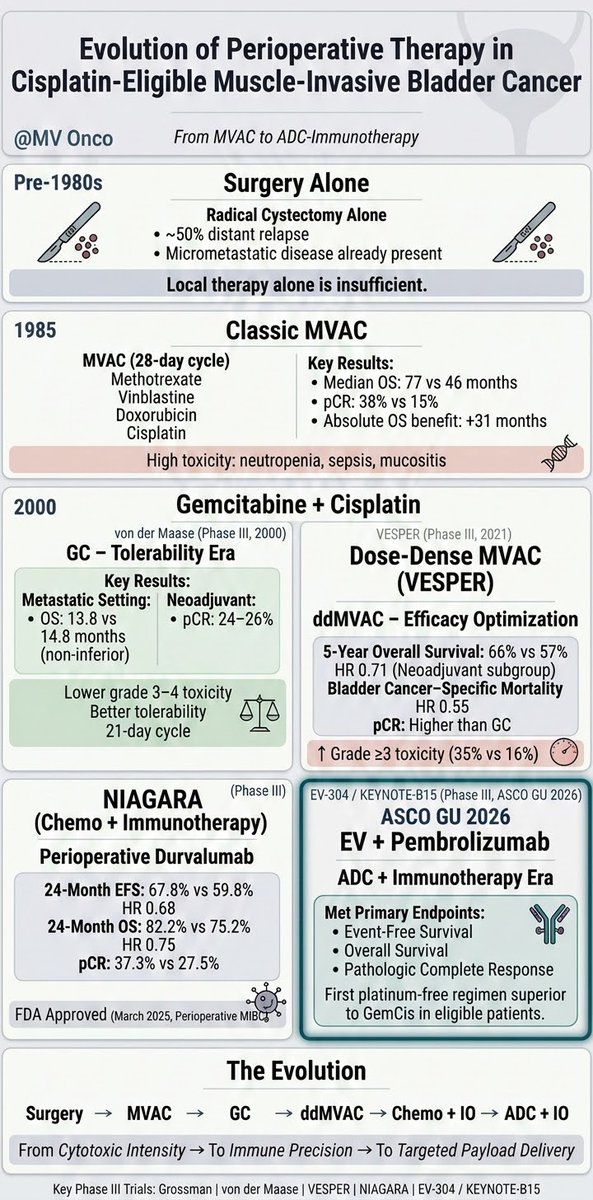
KN-B15/EV303: R3 Perioperative EVP vs Gem/cis in MIBC shows EFS HR 0.53 (0.41–0.70), OS HR 0.65 (0.48-0.89), pCR 56% vs 33%, G3+ tox 76% vs 67% #GU26. About half the patients completed 9 cycles of EVP. These are great results. Gem/cid is harder to beat when not all patients are at risk of relapse. Bladder sparing approaches for cCR (~60%) will be where this ends. ‘EVP 1st, ask questions later’. These studies are needed soon.
Here it is the long awaited KEYNOTE -B15/EV-304. A new reference for the perioperative management of MIBC. The combination of enfortumab vedotin + Pembrolizumab improves survival in this settings. Huge congrats to the team brilliantly led by #MattGalsky. Huge congrats also to the senior author @Uro_Oncologist . Clinically significant impact on pCRs, EFS and OS. Now it’s time to digest the data and compare the outcomes with NIAGARA and discuss the expectations created by EV-303
Los medios están perdiendo interés en Irán. Los políticos están perdiendo interés en Irán. Las celebridades y los influencers nunca han mostrado interés por Irán . No lo permitamos.
90 millones de iraníes sufren la mayor matanza del siglo y están aislados del mundo. ¡Sé su voz!
🚨| URGENTE: El Times revela la terrible verdad: 16.500 manifestantes muertos y 330.000 heridos en Irán 🇮🇷. Dos semanas de protestas en Irán han causado más muertes civiles que dos años de guerra en Gaza. Sin embargo, el mundo parece la otra guerra,
Comparison of prostate-specific antigen kinetics between androgen receptor signaling inhibitor doublet therapy and androgen receptor signaling inhibitor with docetaxel triplet therapy in patients with metastatic castration-sensitive #ProstateCancer
https://t.co/SvDe7SuqV3
Retrospective real-world study compared doublet versus triplet therapy in patients with metastatic castration-sensitive prostate cancer. After matching, triplet therapy led to a higher rate of deep PSA suppression (≤ 0.02 ng/ml) at 12 months, especially in those with high-volume disease, while early PSA response rates were similar between groups. However, triplet therapy was associated with more frequent severe treatment-related adverse events.
Overall, triplet therapy may offer greater PSA benefit for selected patients but with increased toxicity.
@OncoAlert 🚨
@silkegillessen@AOmlin@weoncologists
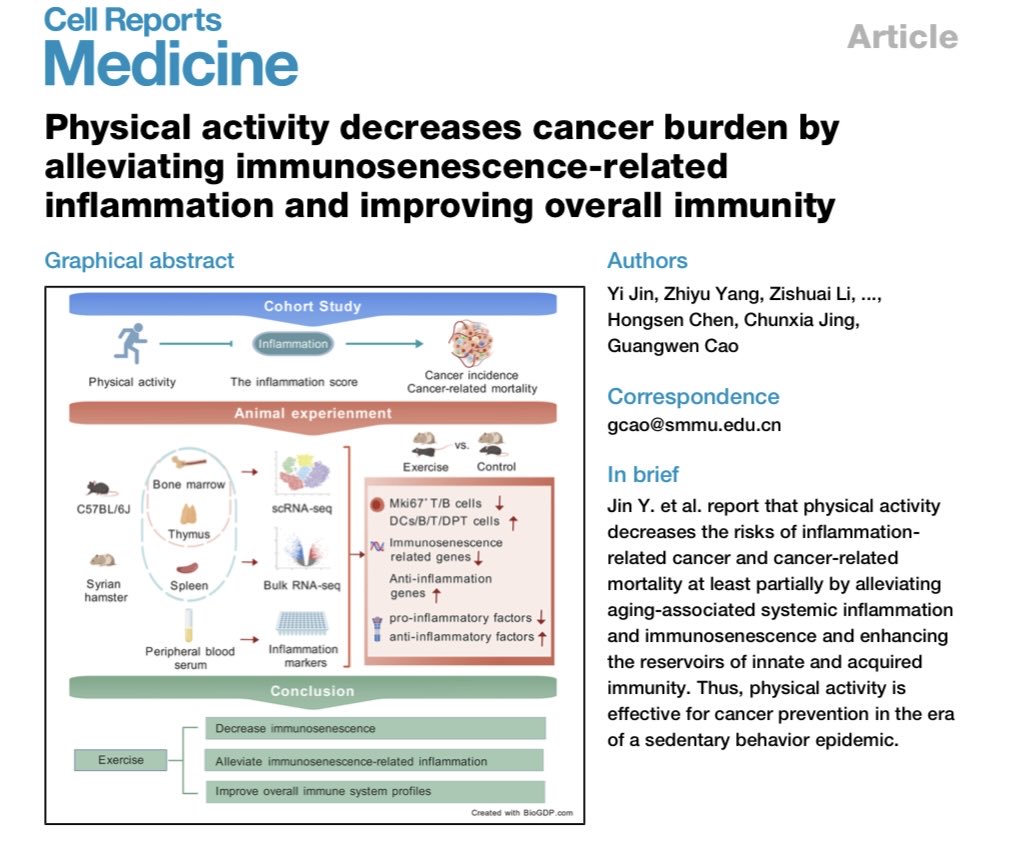
Physical activity decreases cancer burden by alleviating immunosenescence-related inflammation and improving overall immunity https://t.co/3tLuB6ZmOB @OncoAlert
Juan No, médico rehabilitador: «Mi mayor ilusión es que un paciente de cáncer me diga que sigue haciendo ejercicio» @somosLVSalud https://t.co/k42rLyd8Td
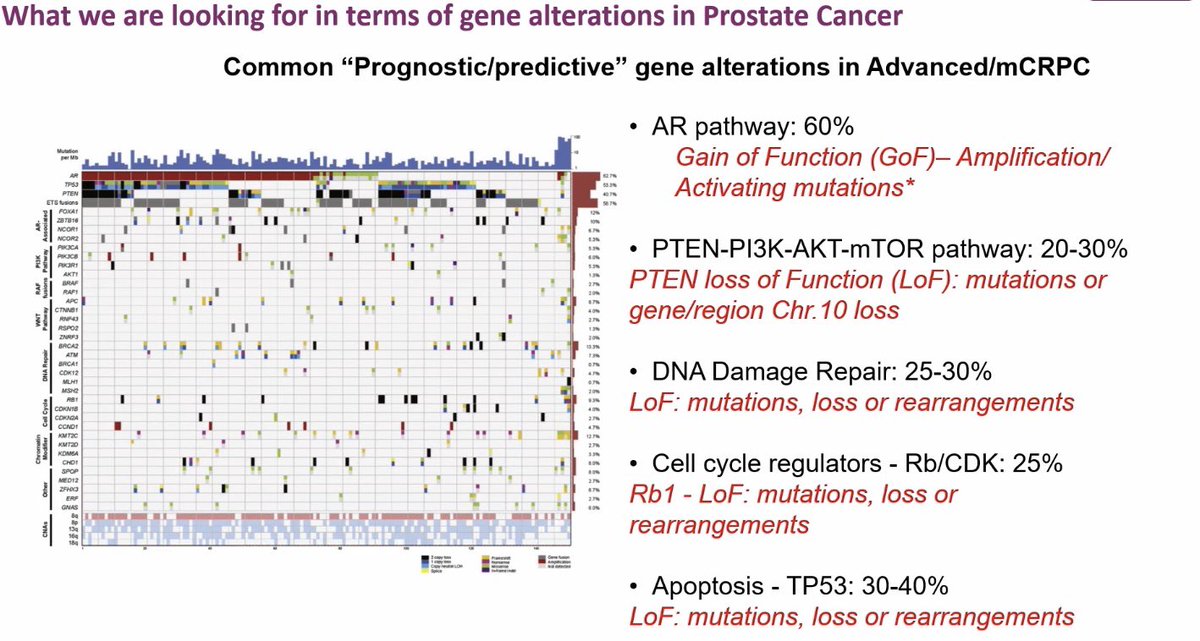
Prostate Cancer Genetics 🧬🔥
What drives advanced mCRPC?
#GlobalForum25#PROSCA25
AR pathway dominates, PTEN loss and PI3K-AKT next, then DDR defects, Rb loss, and TP53 mutations. These are the major therapeutic and prognostic signals.
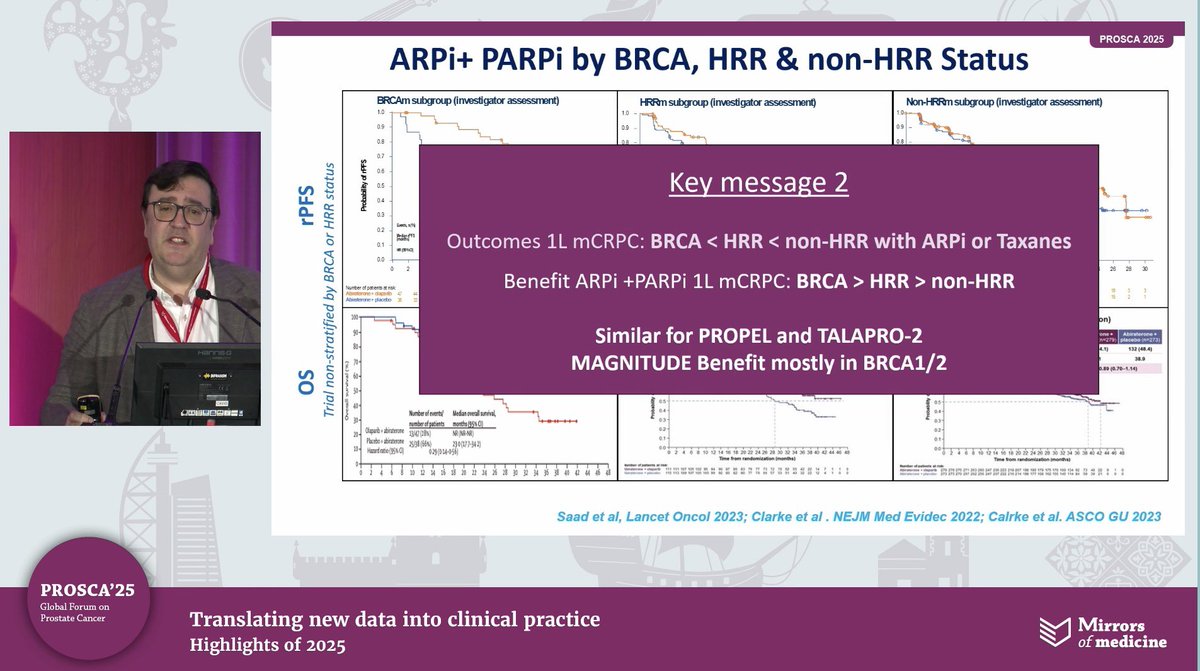
And the ARPi + PARPi story is crystal clear
BRCA patients do the best, HRR moderate, non-HRR lowest benefit.
Same pattern across PROPEL, TALAPRO-2, MAGNITUDE.
The biggest wins always in BRCA1/2.
#OncoTwitter #MedTwitter #ProstateCancer
@oncoalert@asco@myesmo@esmo_open@mirrorsmed
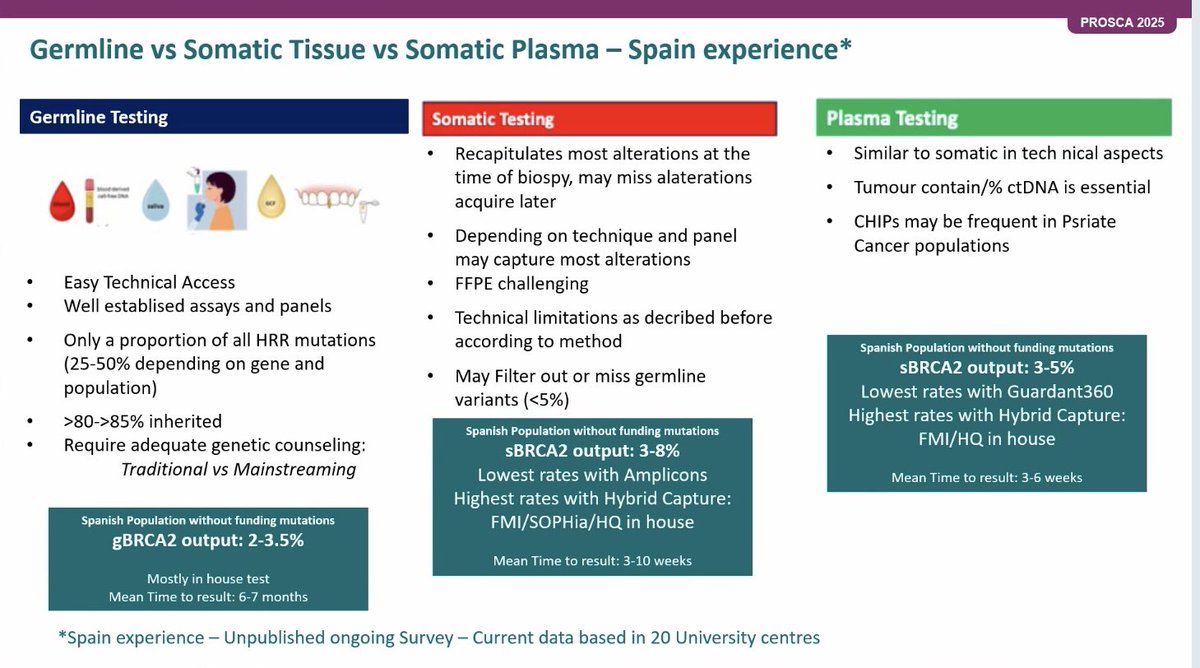
Before ordering HRR testing, ask this: which method will actually find the mutation?
#GlobalForum25#PROSCA25
🩸 Germline
Easy access, stable panels, picks up only 20-50 percent of HRR mutations.
Most variants inherited >80 percent.
gBRCA2 yield about 2-3.5 percent.
🧫 Somatic tissue
Best reflects alterations at biopsy time but technique dependent.
FFPE issues and filtering can miss variants.
sBRCA2 detection 3-8 percent, turnaround 3-10 weeks.
🧪 Plasma (ctDNA)
Similar workflow to somatic but needs adequate tumour fraction.
CHIP can confuse interpretation.
sBRCA2 yield 3-5 percent, turnaround 3-6 weeks.
Takeaway: each method gives different outputs, so test selection matters in mCRPC decision-making 💡
#OncoTwitter #MedTwitter #ProstateCancer @OncoAlert@ASCO@myESMO@ESMO_Open@mirrorsmed