🧵 “Quo Vadis” #UroOncology & #ADC sequencing? A critical moment for our field! 🎯 #ASCO26
Exciting biomarker data from JAVELIN Bladder100 is reshaping how we think about ADC selection 🔬
✅ NECTIN4 & HER2 = NOT prognostic for platinum chemo + avelumab maintenance
💡 BUT low NECTIN4 RNA → numerically prolonged OS (~30mo) with avelumab
⚠️ YET low NECTIN4 tumors = LESS favorable outcomes on EV-P & DVP
👉 Same marker. Opposite signals depending on treatment context — THIS is exactly why biomarker-driven ADC selection is no longer optional. It’s essential for properly treating patients with mUC and MIBC in the future as more and more drugs will come up!
🌏 China is already showing us the way — the ONLY country right now with 2 anti-HER2 & 2 anti-Nectin-4 ADCs with same payload in same line. The real-world data coming will be GOLD 📊
🔬 Basal-squamous UC = lower HER2/NECTIN4, higher EGFR → less favorable on EVP/DVP → making the Iza-Bren program potentially crucial for this subgroup!
We MUST build rational, biomarker-driven sequencing strategies not only availability-driven ones! 💊
What’s your opinion on that topic ?
@Dr_Aggen@MichalSternsch@DrRosenbergMSK@jonchou05@PGrivasMDPhD@drenriquegrande@Markuseckstein3@braegelmannlab@ViktorGruenwald@merck_de@OncoAlert@weoncologists@PTarantinoMD@DrChoueiri@Uromigos@PowlesTom@DrYukselUrun@nachoduranm@montypal@shilpaonc@apolo_andrea@urotoday@niklas_kluemper @PHilbertMD @pernasales@EvanYRosen@DrDjWatson@yao_zhu_sh@AndreaNecchi
#BladderCancer #UroOncology #UBC #ADC #Nectin4 #HER2 #Avelumab #JAVELIN #EV #PrecisionMedicine #Biomarkers #Urology #Oncology #BasalSquamous #SequencingStrategy
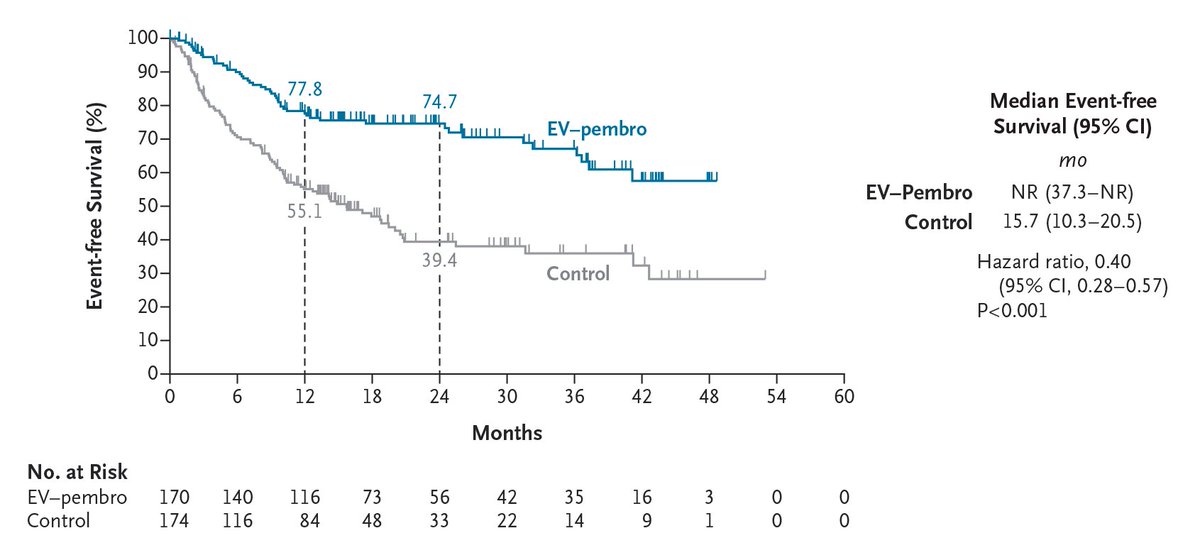
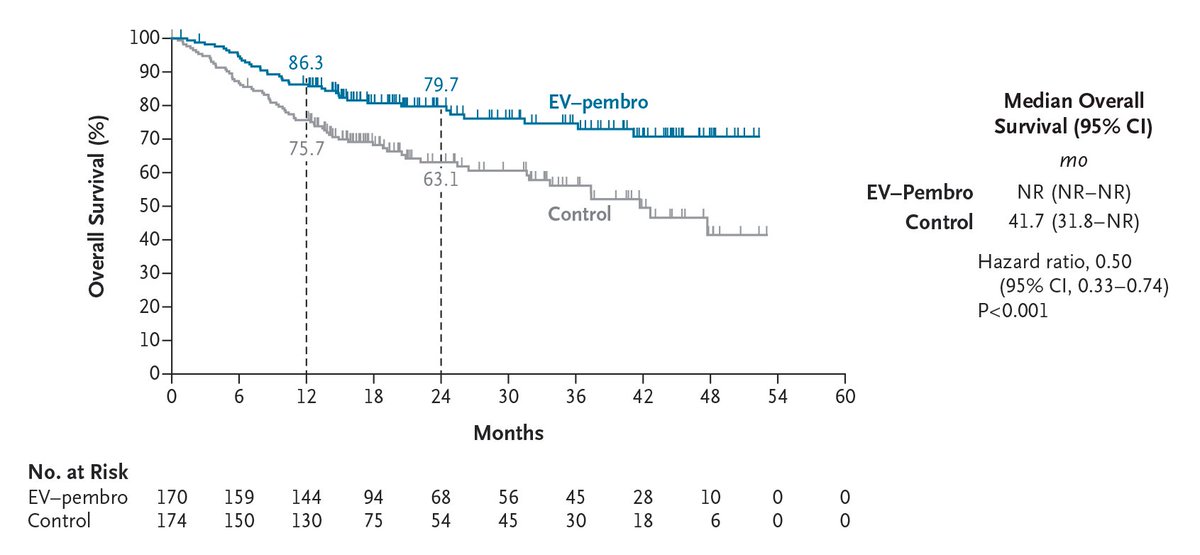
Original Article: Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer (phase 3 KEYNOTE-905/EV-303 trial) https://t.co/VKoHp54Fgs
Editorial: Enfortumab Vedotin plus Pembrolizumab as Perioperative Therapy https://t.co/hpyqWa2eb3
#Oncology
🎆📢First of 2026!
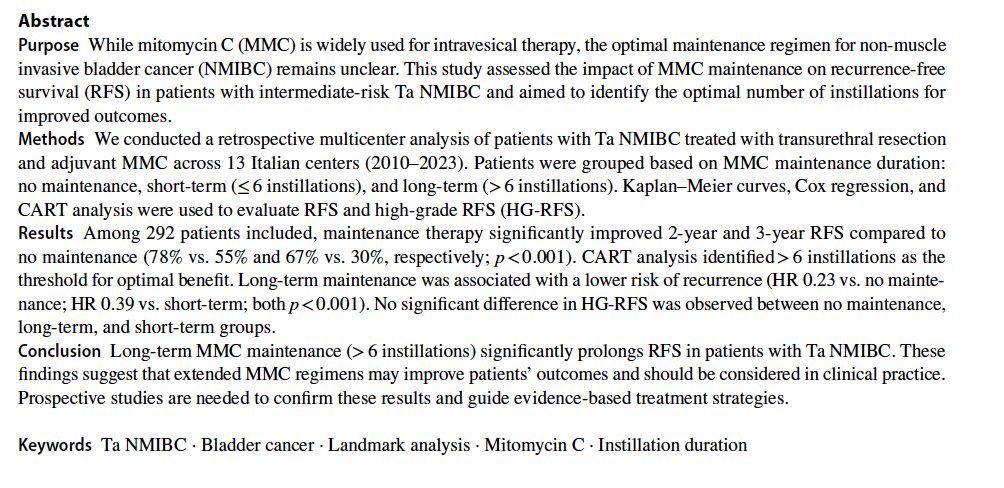
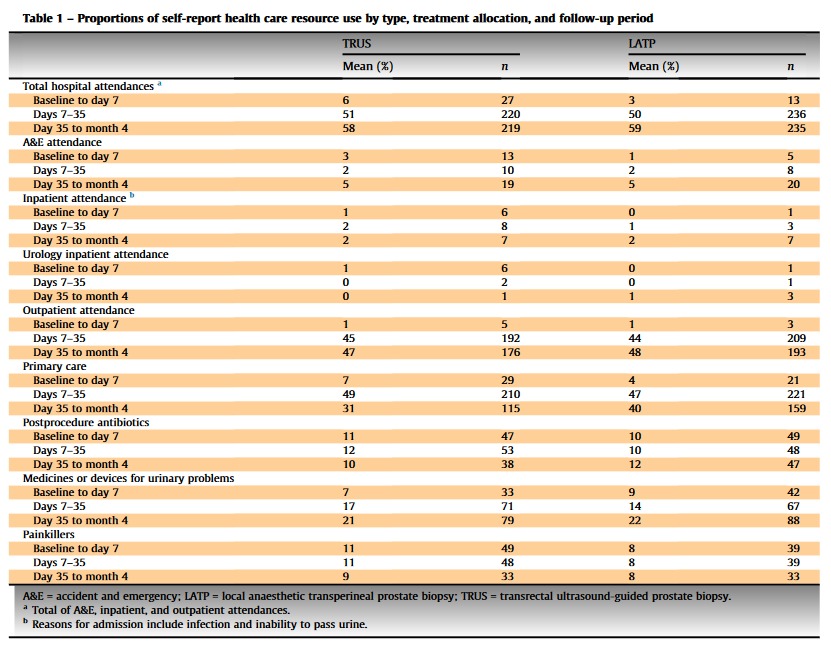
Should we really give MMC maintenance in intermediate-risk #NMIBC, and for how long?
#EAU guidelines recommend adj chemo but the optimal schedule remains unclear
We tried to answer this clinically relevant gap.👇🧵
@Uroweb@urotoday@oncodaily@SpringerNature
📬We are pleased to share our comment on @JAMA_current
Prostatitis continues to represent diagnostic and therapeutic challenges. We discuss key aspects of prostatitis, with particular emphasis on the role of imaging in prostatic abscess' evaluation 👇
https://t.co/BIKT6DXI7n
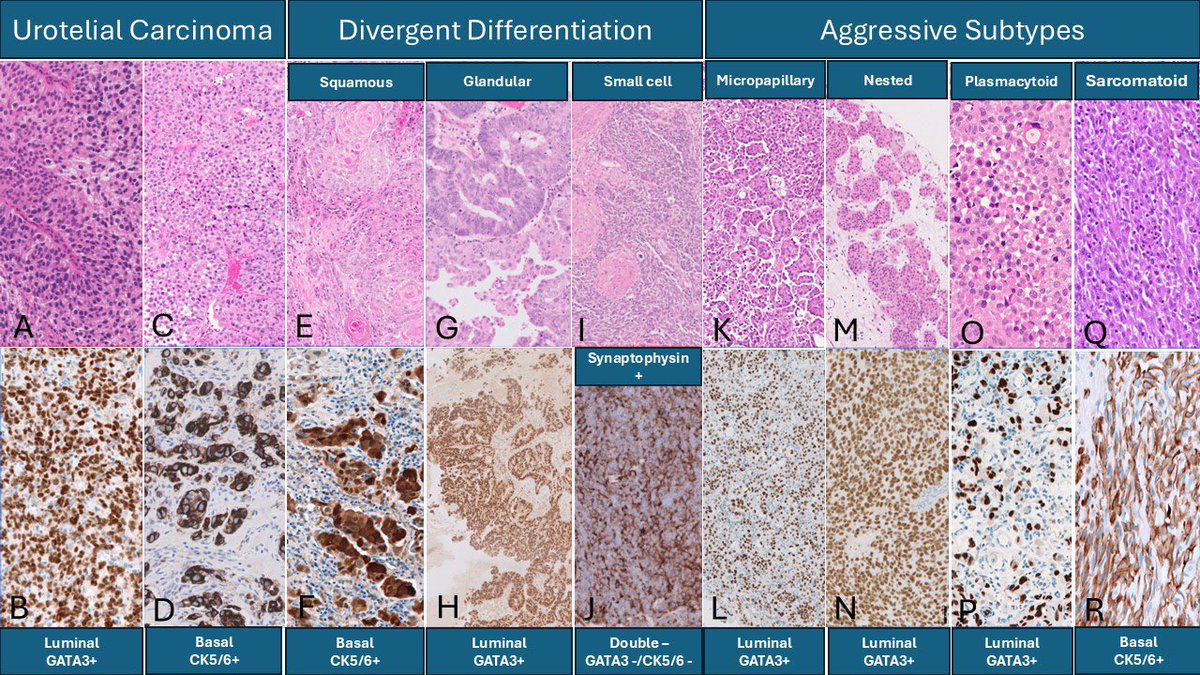
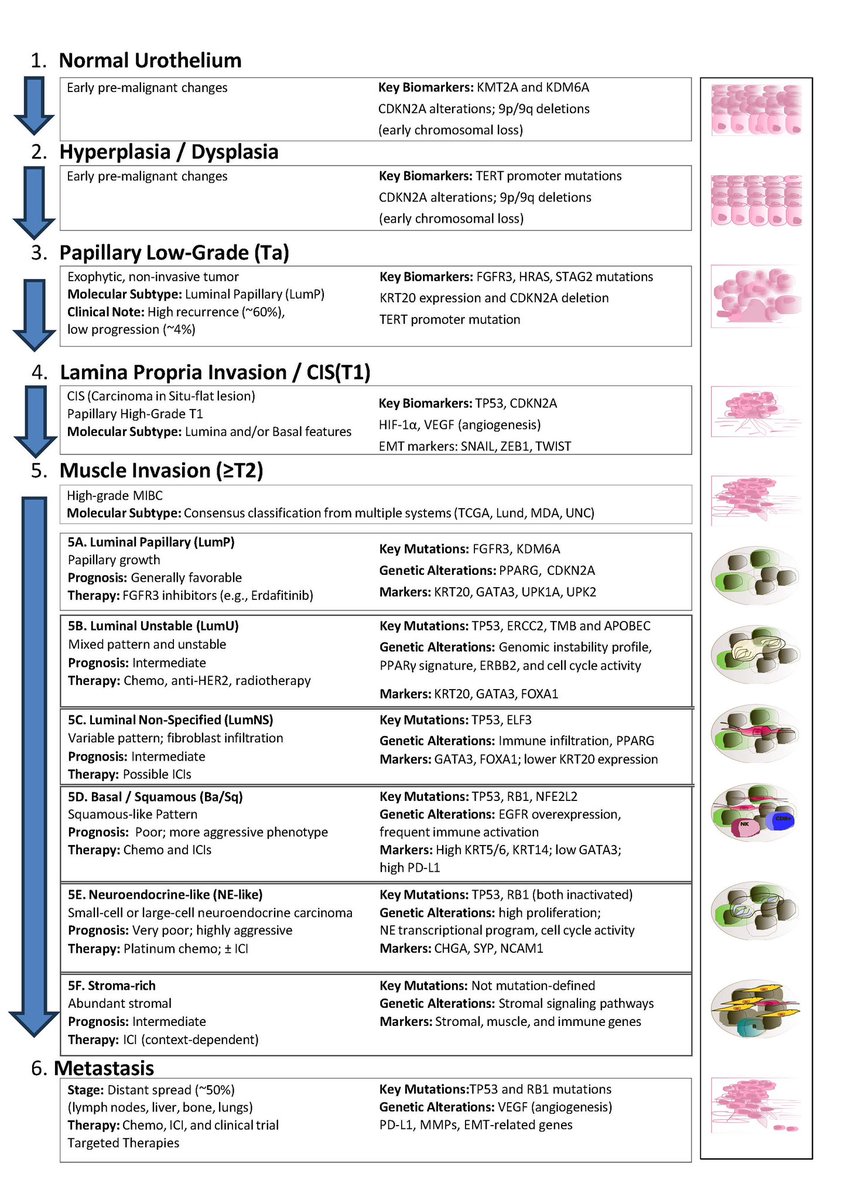
Need an update on the molecular pathology of bladder cancer? I am delighted to share a comprehensive review article by Dr. Antonio Lopez-Beltran and colleagues, published in the 2026 Annual Review Issue of Histopathology @Histo_Journal@daniel_berney 🔗 Article: https://t.co/wPYmanaOxC
Advances in molecular classification, biomarker development, and personalized therapies are transforming the management of bladder cancer. The rapid expansion of therapeutic targets - together with ongoing clinical validation—underscores the essential role of pathologists, as pre-analytical and analytical considerations directly impact the approval, adoption, and optimal use of new cancer drugs. Integrating molecular and morphologic data into routine pathology reporting will be critical to support clinical decision-making and enable precision-based treatment.
Molecular classification remains a rapidly evolving research area with major potential to reshape clinical practice. The marked molecular and morphological heterogeneity of urothelial carcinoma presents challenges, but also offers opportunities to refine patient stratification and tailor therapeutic interventions. Emerging liquid-based biomarkers—including circulating tumor DNA (ctDNA) and urinary tumor DNA (utDNA)—show strong promise for detecting minimal residual disease, monitoring treatment response, and assessing disease dynamics in a minimally invasive manner.
For more GU-focused reviews, the full 2026 Histopathology Annual Review Issue (Special GU Edition) is available here: 🔗https://t.co/eBcHxVuroo
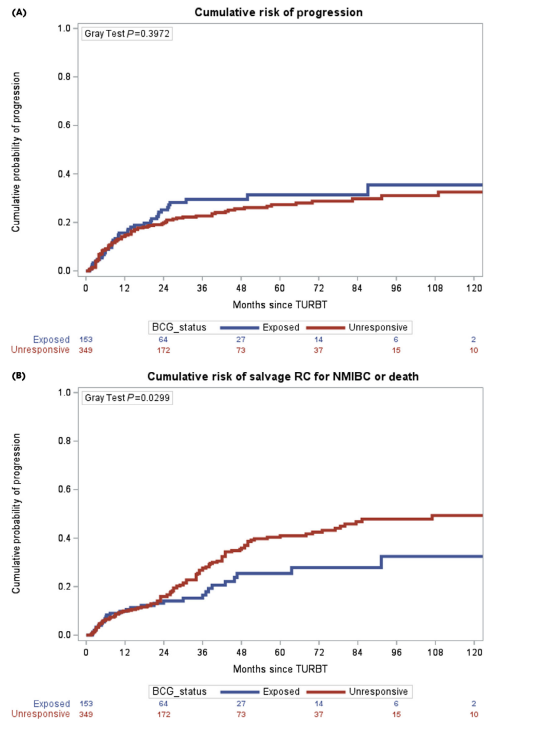
BCG-unresponsive NMIBC trials feel confusing—and inconsistent EFS reporting is a big reason why
We analyze the CIS+ cohorts of 4-FDA registration trials to provide interpretable EFS estimates
🧵👇
@Annals_Oncology@tompowles1@JoshMeeks@wandering_gu
https://t.co/UVlffMc8qY
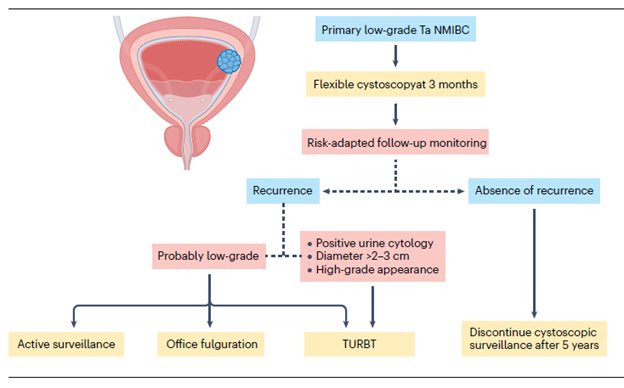
“Low-grade Non–Muscle-Invasive Bladder Cancer: Molecular Landscape, Treatment Strategies, and Emerging Therapies” - just published in Nature Reviews Urology @NatRevUrol. This State-of-the-Art review by Drs. Roger Li @UrogerliMD, Lexi Wen, and colleagues @philippespiess@spsutkaMD@LDyrskjot@DrShariat@UroDocAsh offer an outstanding overview of advances in molecular biology, diagnosis, targeted therapies, and clinical management for #bladdercancer. A great honor to be part of this effort.
Summary:
The management of low-grade non–muscle-invasive bladder cancer (NMIBC) is undergoing rapid evolution, driven by a growing recognition of the need for nuanced, risk-adapted strategies that minimize overtreatment. Yet widespread adoption of de-escalated approaches remains limited by the lack of well-defined, evidence-based guidelines tailored to this favorable-prognosis disease subset. Clear recommendations - particularly regarding surveillance frequency, duration, and criteria for de-intensified care - will likely require international consensus efforts supported by robust prospective data.
A major priority for future research is refining risk stratification. Distinguishing patients at truly increased risk of progression from those with indolent disease will enable more personalized management, including appropriate use of active surveillance and reduced surveillance intensity. Advances in molecular profiling, urine-based biomarkers, and AI-assisted pathology show promise for identifying meaningful biomarkers and histologic patterns to support such stratification, but rigorous prospective validation remains essential before broad clinical adoption.
AI integration into clinical workflows offers additional opportunities to enhance diagnostic accuracy, predict recurrence or progression, and support individualized decision-making. Multimodal models capable of real-time risk assessment may eventually guide therapy selection, but challenges - including the need for diverse training datasets, transparent algorithms, and clear ethical and regulatory frameworks - must be addressed before routine clinical use.
Despite favorable overall outcomes, managing low-grade NMIBC remains challenging owing to high recurrence rates and continued reliance on invasive cystoscopy and imperfect biomarkers. Until emerging diagnostic tools are validated, established clinicopathological systems such as the IBCG risk stratification model will continue to guide treatment decisions. Patients with multiple risk factors generally warrant intravesical therapy, while those without risk factors may be reasonable candidates for active surveillance. The ongoing BCG shortage further underscores the need to balance clinical benefit with treatment burden and to evaluate new intravesical therapies against their potential financial and clinical toxicity.
Meaningful progress in low-grade NMIBC will depend on prospective validation of emerging technologies and therapies, paired with thoughtful integration into evidence-based guidelines. By aligning molecular insights, technological innovation, and risk-adapted clinical practice, the field can improve outcomes while reducing unnecessary interventions and surveillance for this common, yet often overtreated, disease.
The article is available at the following link:
https://t.co/Hkzge1HLDo
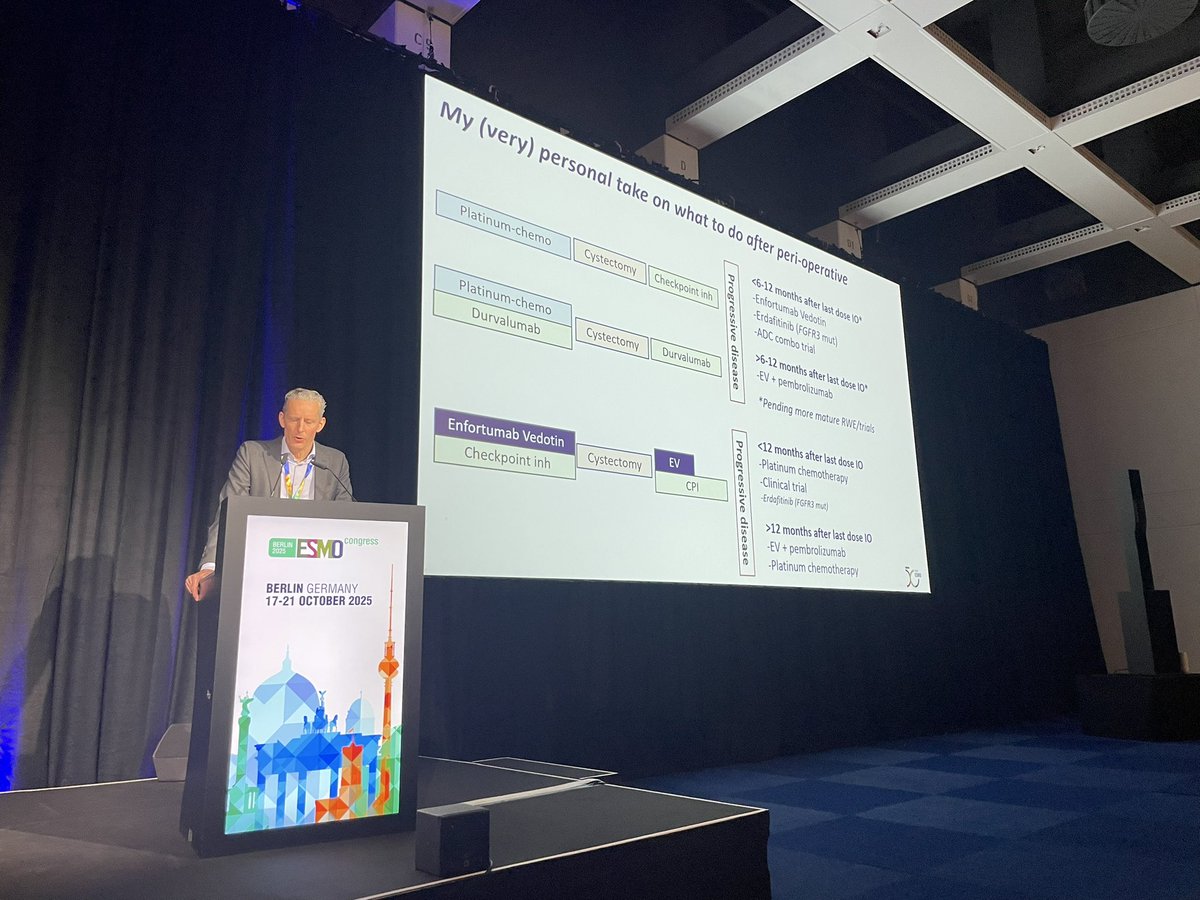
One slide says it all! Terrific distillation by @MichvdHeijden of what to do in emerging pt populations in #bladdercancer, namely pts who received perioperative IO. Mirrors discussions we have been having in #kidneycancer. #ESMO25