❓️Can we avoid ReTURBT in selected patients with T1 NMIBC? ✅️ According to our study YES!
👥️A response-based approach can spare up to 71% of ReTURBT reducing overtreatment
Full paper➡️https://t.co/dmugDLY4Wm
@EurUrolOncol@urotoday@Uroweb@oncodaily@IBCG_BladderCA
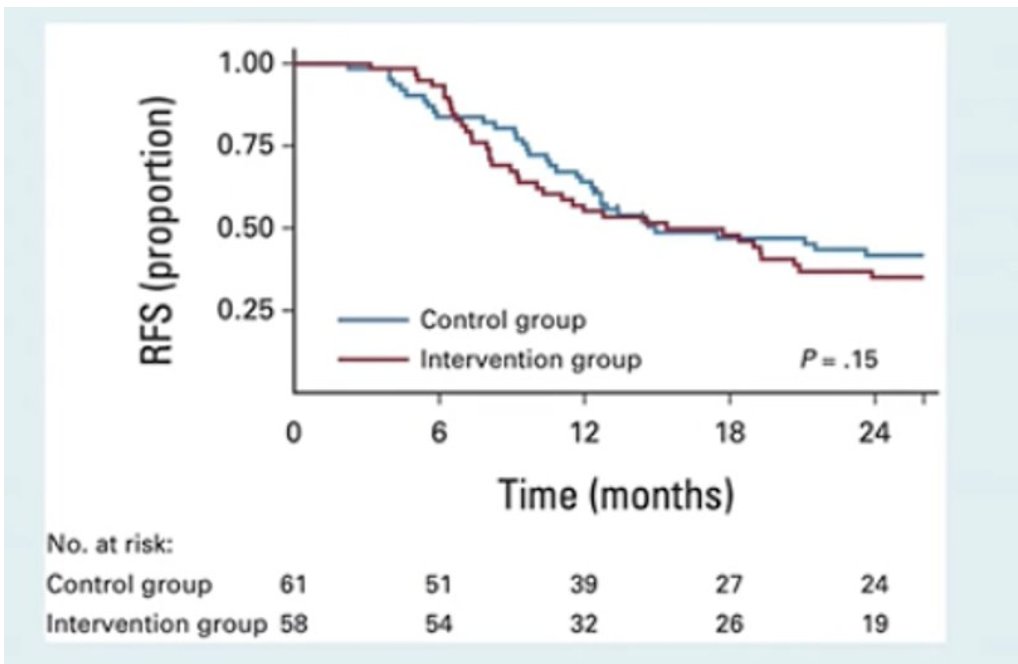
A multi-center study examines maintenance schedules for intermediate-risk #NMIBC. @RobertoContieri@IstTumori joins @UroDocAsh@UTMDAnderson to discuss the results which include two-year recurrence-free survival of 55% with no maintenance versus 78% with any maintenance. Classification and regression tree analysis identified optimal cutoff at more than six monthly instillations. #WatchNow on UroToday > https://t.co/G4Mw1OB0cA
1) Approval based on marginal improvements in efficacy (without improvement to CSS/OS)
2) Toxicity that isn't G5 (death) doesn't seem to impact approval. 10-15% serious autoimmune AEs in NMIBC is deemed ok
3) little weight given to efficacy vs toxicity balance of a drug
Excellent lecture by @SScagliarini_ on the growing importance of patient-reported outcomes in oligometastatic RCC. A crucial reminder that beyond oncologic endpoints, understanding the patient perspective is essential to truly optimize treatment strategies.
@Synergy_Uro@Uroweb
Great pleasure having Prof. Axel Bex at @Synergy_Uro discussing the evolving landscape of locally advanced RCC. Excellent insights and stimulating discussion on current challenges and future directions in kidney cancer care. @eau_yuo@EAUYAU_RenalCa@UrowebESU@EAU_Uroonco
The definitive #SYNERGY26 programme is out
📆 28–29 May | 📍 Naples
Locally-advanced & Oigometastatic GU cancers Edition.
Program: https://t.co/Gx1pBWHGEk
As every year, a packed room for the AUA-IBCG Forum, taking place right now in Salon H.
Great discussions and energy around the future of bladder cancer care and research.
#AUA2026#BladderCancer@IBCG_BladderCA@UroDocAsh
To escalate or de-escalate treatment in BCG-naive HR NMIBC?
Our thoughts on the recent JCOG1019 trial by Kitamura et al @EUplatinum
Free access to full text 👇🏽
https://t.co/xH5ios6rmT
@RobertoContieri@LAUrology_NL@UroDocAsh
A multi-center study examines maintenance schedules for intermediate-risk #NMIBC. @RobertoContieri@IstTumori joins @UroDocAsh@UTMDAnderson to discuss the results which include two-year recurrence-free survival of 55% with no maintenance versus 78% with any maintenance. Classification and regression tree analysis identified optimal cutoff at more than six monthly instillations. #WatchNow on UroToday > https://t.co/G4Mw1OB0cA
The International Bladder Cancer Group Travel Award to support outstanding fellows and early-career academic faculty committed to advancing the field of bladder cancer is now offered annually to provide emerging leaders the opportunity to participate in the IBCG Annual Retreat.
Details at link: https://t.co/y8zbYkeLac
#BladderCancer #IBCG26
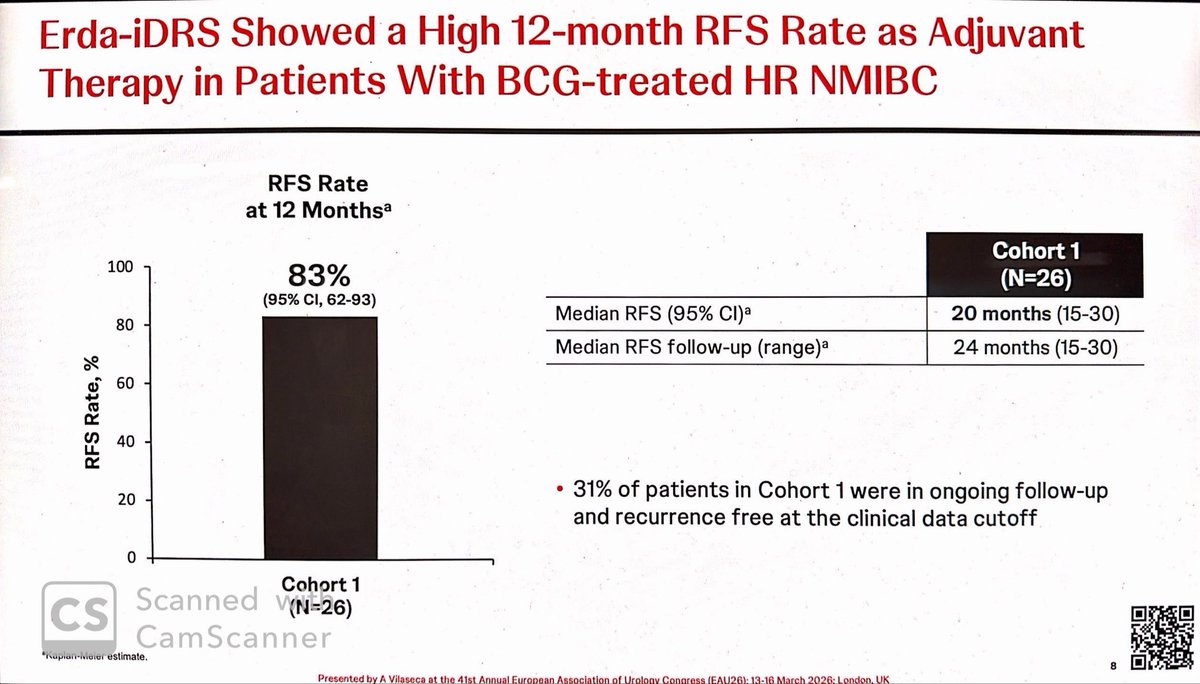
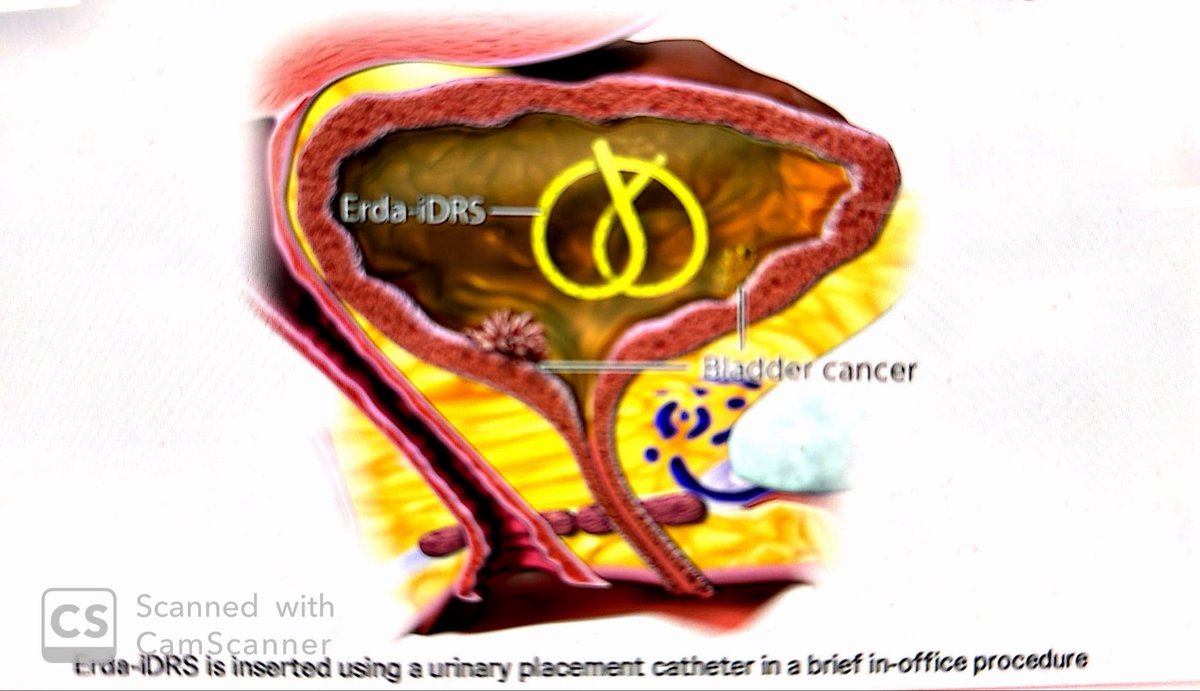
@tonivilaseca presenting promising early data for intravesical erdafitinib (Erda-iDRS) “TAR 210” in NMIBC presented at #EAU26
➡️ 83% 12-mo RFS as adjuvant therapy in HR NMIBC (n=26)
➡️ 89% CR at 6 months in IR NMIBC ablative cohort
Targeted #FGFR therapy moving earlier into NMIBC disease states. @JoshMeeks@DrFelixGuerrero@IBCG_BladderCA@BladderCancerUS
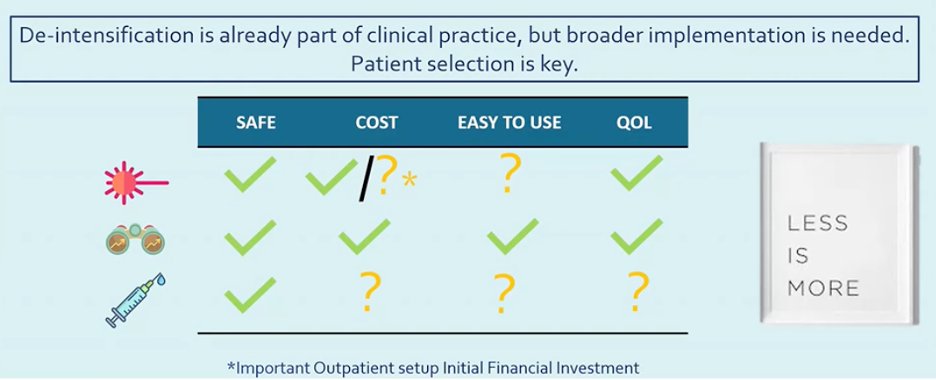
Which #NMIBC patients may safely receive de-intensified treatment?
At #EAU26@RobertoContieri (@istitutotumori) discusses risk stratification for de-escalation, findings from the ROBUUST database on histological subtypes, and optimizing mitomycin C maintenance in intermediate-risk Ta disease
@Uroweb #GUsm #BladderCancer
#EAU26@RobertoContieri “Less is more” in select NMIBC
🔹 Office-based fulguration
🔹 Active surveillance
🔹 Chemoablation
🎯 The key is patient selection.
@uroweb@UroToday
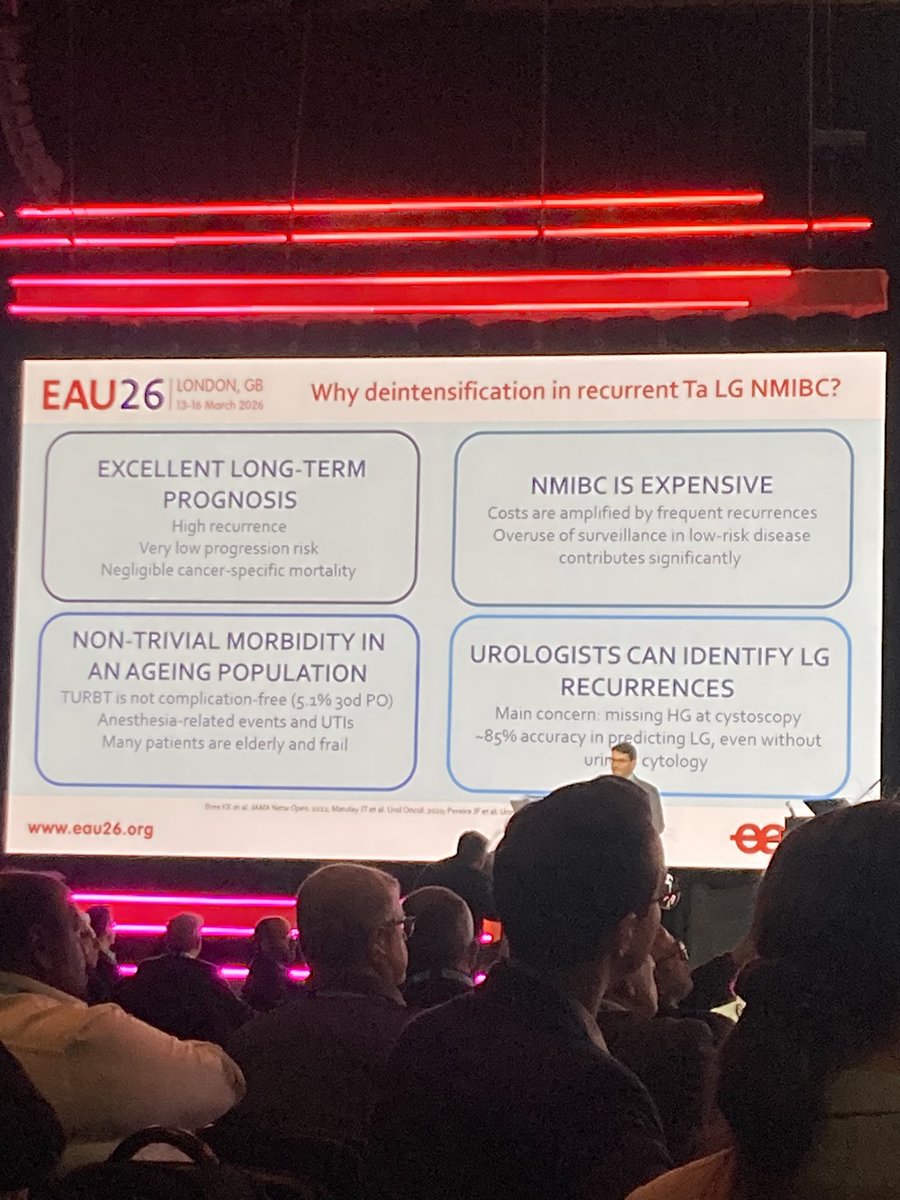
Excellent case for de-escalating management of LGTa #bladdercancer by @RobertoContieri
LG Ta has low progression risk & negligible CSM yet…
We overtreat LGTa
We oversurveil LGTa
Active surveillance in well selected pts is safe, cost-effective & maintains excellent QoL #EAU26