People have been DM and asking me: with an HR of 0.68 for durvalumab + BCG in POTOMAC, why isn’t this for every high-risk NMIBC patient?
Here’s how hazard ratios work – and why they can mislead you if you stop there. 🧵 #ASCO26@tompowles1@WesKassouf@shilpaonc@DrFelixGuerrero
Time to revisit something I’ve been saying for years: TaHG bladder cancer is not intermediate risk. The clinical outcomes, molecular biology ... all point in the same direction.
Yet some frameworks allow < 3cm TaHG tumors to be downgraded into “intermediate risk” alongside low-grade disease.
That classification has real consequences for patients:
• undertreatment
• less rigorous surveillance
• in some studies, these patients are even placed on observation as a supposedly appropriate “control arm.”
TaHG is high risk. 🧵 @BladderCancerUS@WorldBladderCan@IBCG_BladderCA
One of the most exciting talks at #AUA26 - @jteoh_hk from @CUHKMedicine delivering the John K. Lattimer Lecture - one of the most prestigious in urology.
Jeremy is not just a friend and a colleague. He is one of the most innovative urologists of his generation and a driving force in the @IBCG_BladderCA.
Today he is challenging the status quo on TURBT. 🧵
Delighted to see that my @TheLancet article was referred to as a landmark 'Provocative' paper at DDW. I guess I like to ruffle a few feathers 🤪 @DDWMeeting#BarrettsEsophagus
Had the pleasure of being a discussant on this very topic at #EAU26. My take? - Stick to the plan!
The survival benefit in EV-304/303 was built on consolidation RC+PLND - not observation, not TMT.
EV+P and radical cystectomy together deliver the advantage. Skipping surgery outside a clinical trial based on cCR alone is premature. Those studies are needed - and are underway - but we have no data yet.
#AUA2026 #AACR2026
Surgery is a "wicked" environment: feedback is delayed, noisy, and often biased. My essay on why experience doesn't always equal mastery, and how to learn when the feedback loops are broken.
https://t.co/mkHMtpskBV
#MedTwitter#Surgery#MedEd
So exciting that this is now in the NCCN guidelines!
No doubt that this will better stratify IR NMIBC patients for clinical trials.
Grateful to @UroDocAsh and the @IBCG_BladderCA team for the opportunity to lead this work
https://t.co/X1QvHxC9HV
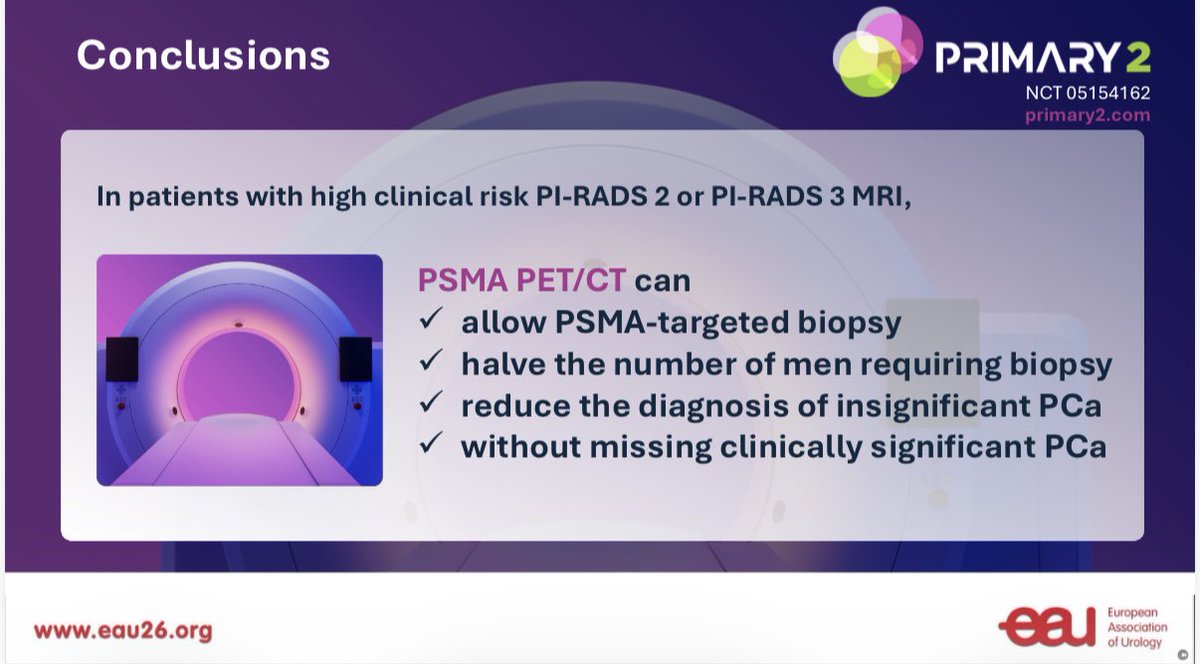
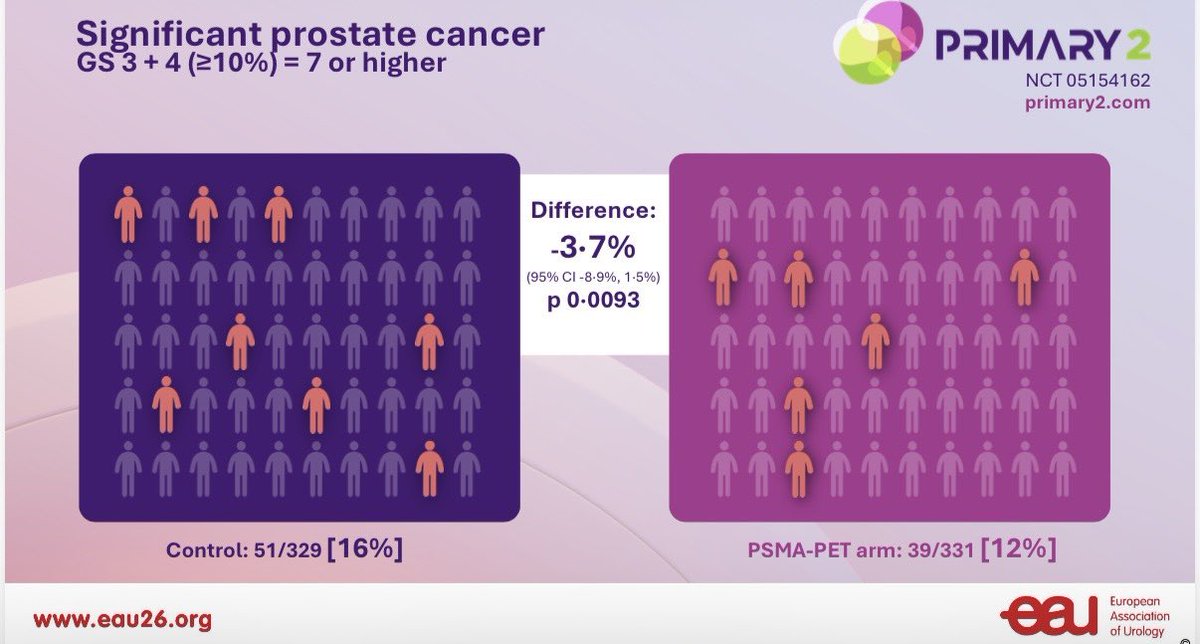
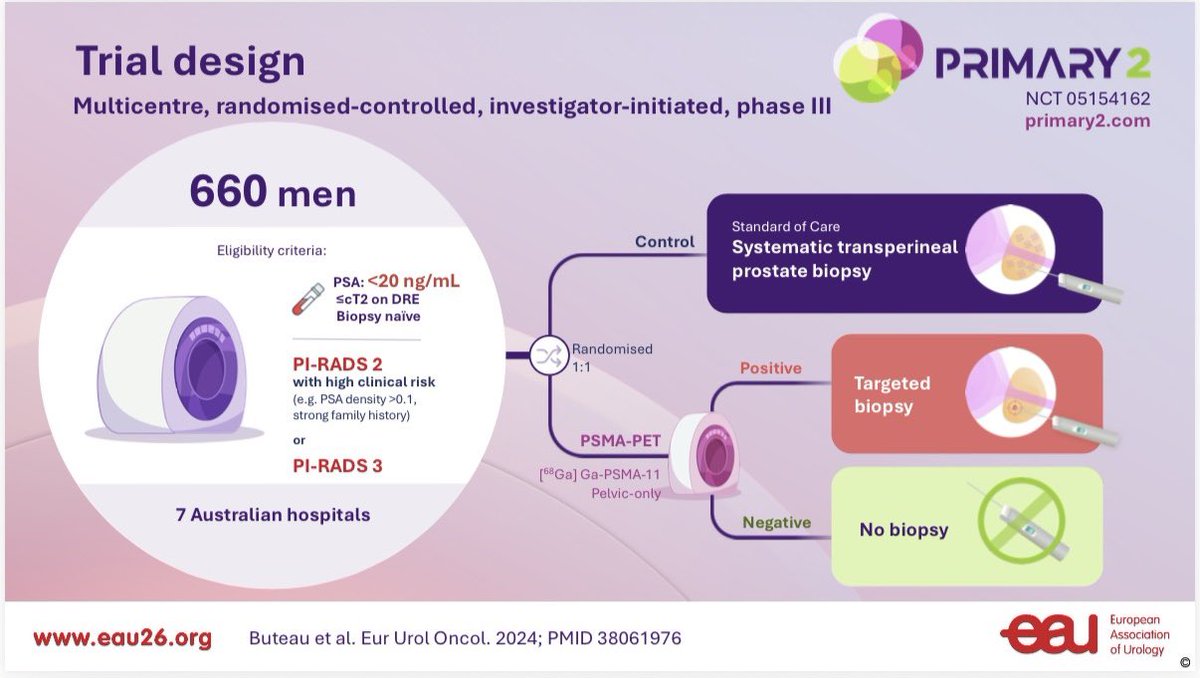
🚨 Gamechanger #PRIMARY2 RCT #EAU26, presented and in press @TheLancetOncol. PSMA-PET CT in men with equivocal or -ve MRI but red flags results reduces biopsy by 49% and has non-inferior csPCa detection to template biopsy in all. Proud to be part of this🚨
Agree. BCG remains effective with minimal tox. Adding IO increases efficacy marginally with significantly increasing tox.
Unless we see a significant reduction in MIBC progression, justifying IO for BCG-naive (or unresponsive) patients is difficult
We are proud to share that our @drtanws has been awarded England's Royal College of Surgeons' 2026 Hunterian Professorship for his work on non-muscle invasive #bladdercancer
The award is given to those who have made an outstanding contribution to surgical research and practice.
I’m truly honoured to receive the 2026 Hunterian Professorship from the Royal College of Surgeons of England for my work on non-muscle invasive bladder cancer.
I owe a debt of gratitude to my mentors John Kelly & @UroDocAsh whose wisdom and encouragement have shaped my journey.
Huge congratulations to @drtanws on being awarded the prestigious Hunterian Professorship by Royal College of Surgeons of England.
A well-deserved recognition of his outstanding work in defining NMIBC risk stratification in bladder cancer.
Proud to see you continue to excel and lead on the global stage!
@Yale_Urology@UCLDivofSurgery@MDAndersonNews #OncSurgery @RCSnews@SUO_YUO@UroToday