Phase Ib results from the phase Ib/II study of [Lu]Lu-DOTA-TATE in combination with standard of care as a first-line treatment for pts with ES-SCLC.
☢️ Feasible but challenging combination. Hard to understand the contribution of Lu-DOTA-TATE in terms of efficacy. Ongoing phase II study no longer recruiting patients.
#ASCO25 #SCLC #LCSM
Dr. @LuisPaz_Ares: biomarkers from phase III IMforte trial of maintenance lurbinectedin in SCLC #ASCO26. PFS & OS benefit of maintenance lurbinectedin seen across molecular subtypes and independent of SLFN11 expression. Suggestion that lurbi may overcome TAM-mediated resistance.
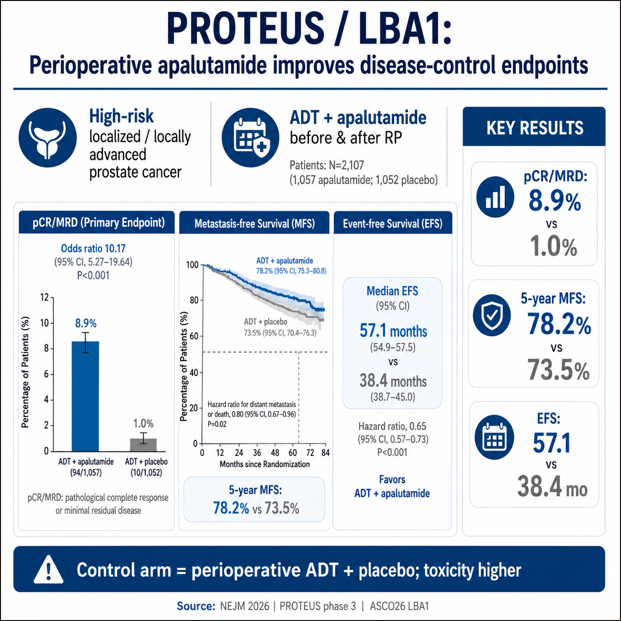
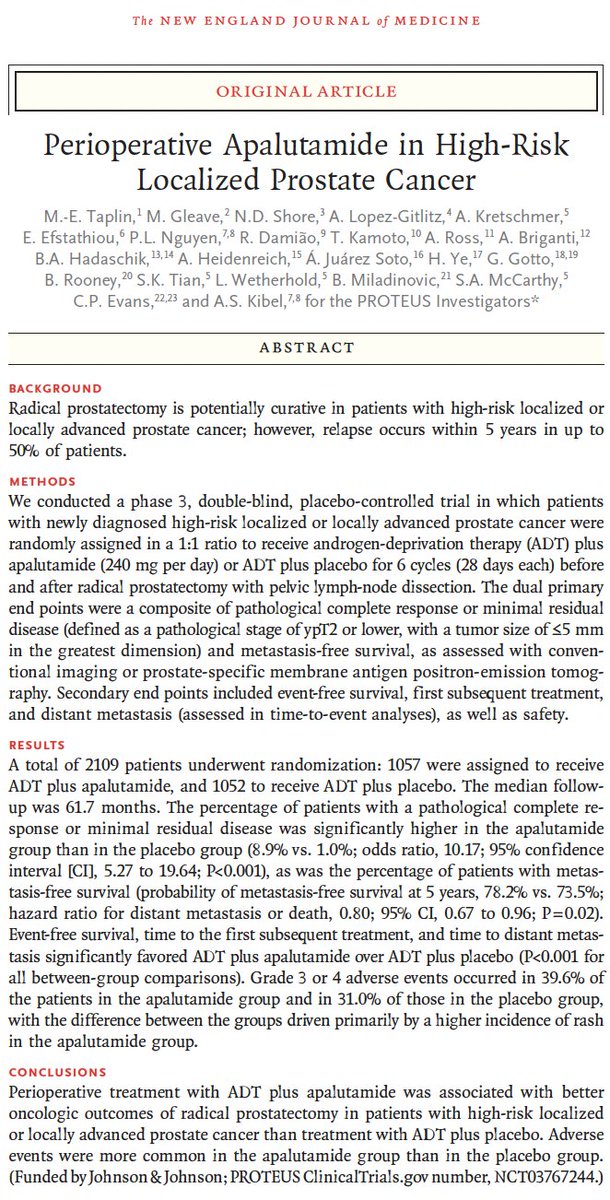
🚨 PROTEUS: perioperative apalutamide moves into high-risk localized #prostatecancer
Just out in @NEJM
🧬 2109 men w/ high-risk localized or locally advanced PCa randomized to ADT + apalutamide vs ADT + placebo around radical prostatectomy.
🎯 Both stated primary endpoints met.
⚠️ But the trial deserves nuance. Thread 🧵
#ASCO26 @ASCO@PCF_Science
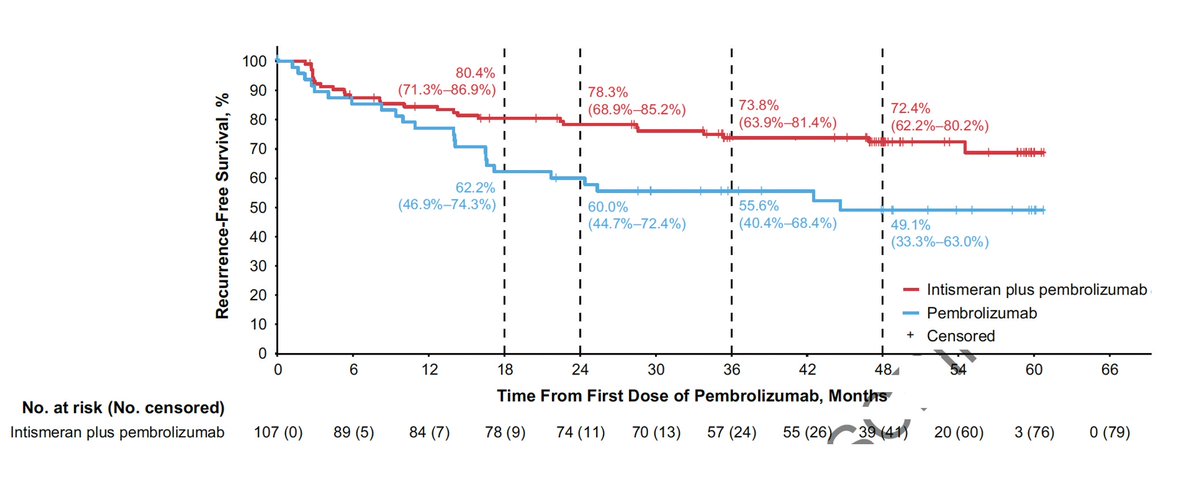
Another major advance vs cancer! @ASCO#ASCO26
Personalized neoantigen mRNA vaccine 5 year follow-up vs metastatic melanoma reduced recurrence and death by 49% (on top of Keytruda)
https://t.co/NadITTYIT2
Subgroup analyses by disease volume and de novo/recurrent #mHSPC in the #PSMAddition study of [177Lu]Lu-PSMA-617. Presentation by Fred Saad, CQ, MD, FRCS, FCAHS @chumontreal. #ASCO26 written coverage by @RKSayyid@UAUrology > https://t.co/WlcyMVLacY @ASCO
#ASCO26 GU Oncology Spotlight 🚨
🔬 Abstract 4521 | CaboNivo in non–clear cell RCC
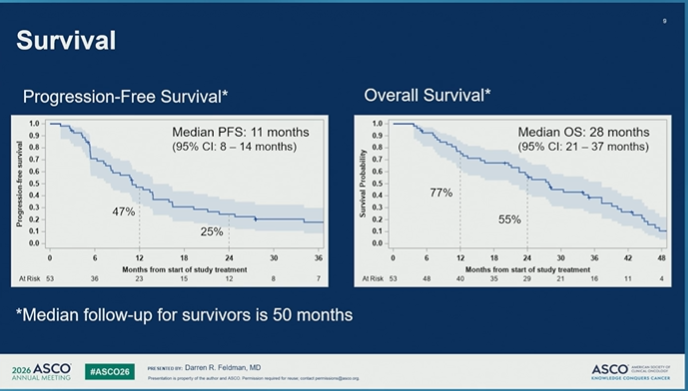
Final results of phase 2 cabozantinib + nivolumab in patients with non–clear cell renal cell carcinoma
Presented by Darren R. Feldman, MD
@ASCO@OncoAlert
Important final dataset in a difficult RCC space.
Non–clear cell RCC represents a biologically diverse group of kidney cancers, often with fewer prospective data and historically poorer outcomes than clear cell RCC.
🔵 Study design
Investigator-initiated phase 2 study:
➡️ cabozantinib 40 mg daily
➡️ nivolumab 240 mg q2w or 480 mg q4w
Cohort 1 included:
• papillary RCC
• FH-deficient RCC
• unclassified RCC
• translocation-associated RCC
Chromophobe RCC was evaluated separately and closed early for inefficacy.
🟢 Final efficacy signal
With longer follow-up of ~50 months, CaboNivo reaffirmed antitumor activity in non–clear cell RCC.
In cohort 1:
• N = 53
• PR/CR: 43%
• median PFS: 11 months
• median OS: 28 months
Responses were seen across several non–clear cell histologies, with a particularly notable signal in FH-deficient RCC:
➡️ 7/8 patients had an objective response.
🔵 Why it matters
Non–clear cell RCC is not one disease.
Histology matters.
Biology matters.
And prospective treatment data remain limited.
This final analysis supports cabozantinib + nivolumab as an active regimen for selected patients with non–clear cell RCC histologies, especially papillary, FH-deficient, unclassified, and translocation-associated disease.
🟠 Safety
Toxicity was consistent with known cabozantinib + nivolumab profiles.
Grade 3/4 treatment-emergent AEs occurred in a substantial proportion of patients, and discontinuations due to AEs occurred with cabozantinib, nivolumab, or both.
So this is active therapy — but not low-burden therapy.
🧠 My take
CaboNivo is one of the more clinically useful prospective datasets in non–clear cell RCC.
The key message is not “treat all non–clear cell RCC the same.”
It is:
➡️ use histology
➡️ recognize biologic subgroups
➡️ avoid assuming clear-cell algorithms fully apply
➡️ consider CaboNivo as a treatment option where prospective evidence supports activity
➡️ continue building trials specific to rare RCC subtypes
For non–clear cell RCC, better classification is the beginning of better treatment.
#ASCO26 #GUOnc #KidneyCancer #RCC #NonClearCellRCC #PapillaryRCC #FHdeficientRCC #Cabozantinib #Nivolumab #PrecisionOncology
@OncLive@TargetedOnc@CancerNetwrk@ASCOPost@ecancer@VJOncology@curetoday@JCO_ASCO
#ASCO26 GU Oncology Spotlight 🚨
🔬 Abstract 5017 | PROTRACT
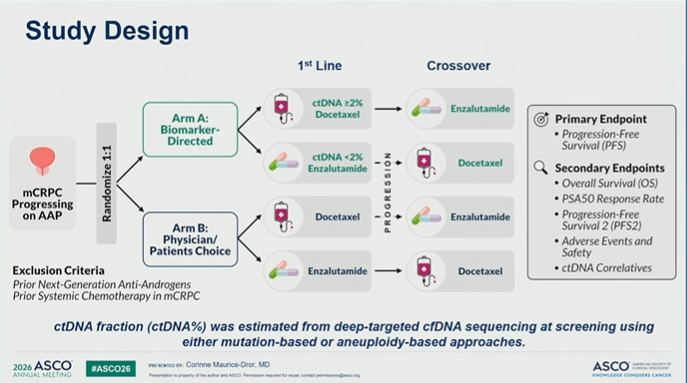
ctDNA-guided biomarker-directed therapy vs physician/patient choice in mCRPC progressing after abiraterone/prednisone
Presented by Corinne Maurice-Dror, MD
@ASCO@OncoAlert
This is a very relevant precision-oncology question in prostate cancer:
➡️ Can ctDNA help guide whether a patient should receive docetaxel or enzalutamide after progression on abiraterone?
PROTRACT tested a simple treatment-selection strategy:
🔵 Biomarker-directed arm
• ctDNA ≥2% → docetaxel
• ctDNA <2% → enzalutamide
vs
🟠 Physician/patient choice
• docetaxel or enzalutamide, based on clinical preference
Primary endpoint: PFS
Secondary endpoints included OS, PSA50 response, PFS2, safety, and ctDNA correlatives.
🔵 Why this matters
This trial directly addresses a common real-world problem:
After abiraterone progression in mCRPC, treatment choice is often based on clinical judgment, patient preference, fitness, access, and toxicity concerns.
But biology may matter.
A higher ctDNA fraction may reflect more aggressive disease biology and could potentially support moving toward chemotherapy rather than sequential AR pathway inhibition.
🔵 Feasibility signal
The study randomized 42 patients before early termination due to slow accrual.
Importantly:
➡️ 57% of patients had discordance between physician/patient preference and ctDNA-directed assignment.
That is the key signal.
ctDNA guidance would have changed the treatment direction for more than half of patients.
🟠 Important caveat
This was underpowered and stopped early.
So PROTRACT should not be read as a definitive efficacy trial.
But it is still highly informative because it shows how often biomarker-directed treatment selection may differ from usual clinical choice.
🔵 My take
PROTRACT is important not because it settles the sequencing question, but because it frames the next one:
➡️ Can ctDNA move from prognostic biomarker to treatment-selection tool in mCRPC?
The future algorithm may not simply ask:
“ARPI again or chemotherapy?”
It may ask:
What does the tumor biology suggest this patient needs next?
#ASCO26 #GUOnc #ProstateCancer #mCRPC #ctDNA #PrecisionOncology #Biomarkers #ClinicalTrials #TreatmentSequencing
@OncLive@TargetedOnc@CancerNetwork@ASCOPost@ecancer@VJOncology@curetoday
#ASCO26 GU highlight 🚨
LBA1 PROTEUS
Perioperative apalutamide + ADT in high-risk localized / locally advanced prostate cancer
@ASCO@OncoAlert@NEJM
Presented by @MaryEllenTaplin
Published in @NEJM
https://t.co/0JWZmhn0df
This is a major perioperative prostate cancer dataset.
#PROTEUS tested 6 cycles of neoadjuvant + 6 cycles of adjuvant apalutamide added to ADT around radical prostatectomy.
Key results:
• pCR / minimal residual disease: 8.9% vs 1.0%
• 5-year metastasis-free survival: 78.2% vs 73.5%
• HR for distant metastasis or death: 0.80
• Event-free survival: 57.1 vs 38.4 months
• Time to first subsequent therapy: 74.2 vs 41.5 months
Why it matters:
For years, systemic perioperative intensification around prostatectomy has been difficult to establish in high-risk localized prostate cancer.
PROTEUS gives phase 3 evidence that deeper androgen-receptor pathway inhibition can improve pathologic response and delay clinically relevant recurrence events.
Important caveats:
This was not surgery alone vs systemic therapy.
The control arm received perioperative ADT + placebo.
MFS by conventional imaging alone was not significantly different.
Grade 3/4 AEs were higher with apalutamide, largely driven by rash.
My take:
This is practice-informing and potentially paradigm-shaping, but implementation will require careful patient selection, toxicity counseling, imaging context, and multidisciplinary discussion.
@EAntonarakis@DanaFarber_GU@DrChoueiri@montypal@tompowles1@brian_rini@PGrivasMDPhD@DrRanaMcKay@AliciaMorgans@amerseburger @NealShoreMD @DrYukselUrun@BraunMDPhD@DrSpratticus@EAntonarakis@KOSJ12@LoebStacy@apolo_andrea@AndreaNecchi@DrDanielHeng@neerajaiims@OncLive@TargetedOnc@CancerNetwrk@ASCOPost@VJOncology@ecancer
#ProstateCancer #GUonc #Oncology
Phase III MAIN-CAV: Maintenance #avelumab + #cabozantinib did not improve OS (23 v 24.8)/PFS vs avelumab alone in #mUC after 1L platinum chemo, though very small numbers/early closure amid changing 1L landscape. Great efforts f/ investigators& research team! #ASCO26
Duravelo-2 reports encouraging activity of the Bicycle Drug Conjugate zelenectide pevedotin (BT8009)+pembrolizumab in 1L mUC: ORR 55–58%,CR ~27%, low discontinuation rate (3%),no severe skin reactions and no hyperglycemia. A Future alternative?? @OncoAlert
POTOMAC 5-year OS update presented by Dr Maria De Santis: Durvalumab + BCG (I+M) continues to show no detriment to OS vs BCG alone in BCG-naive high-risk NMIBC (5-yr OS 87.6% vs 86.3%), with no major impact on quality of life. #ASCO26#BladderCancer@OncoAlert@ASCO@OncBrothers
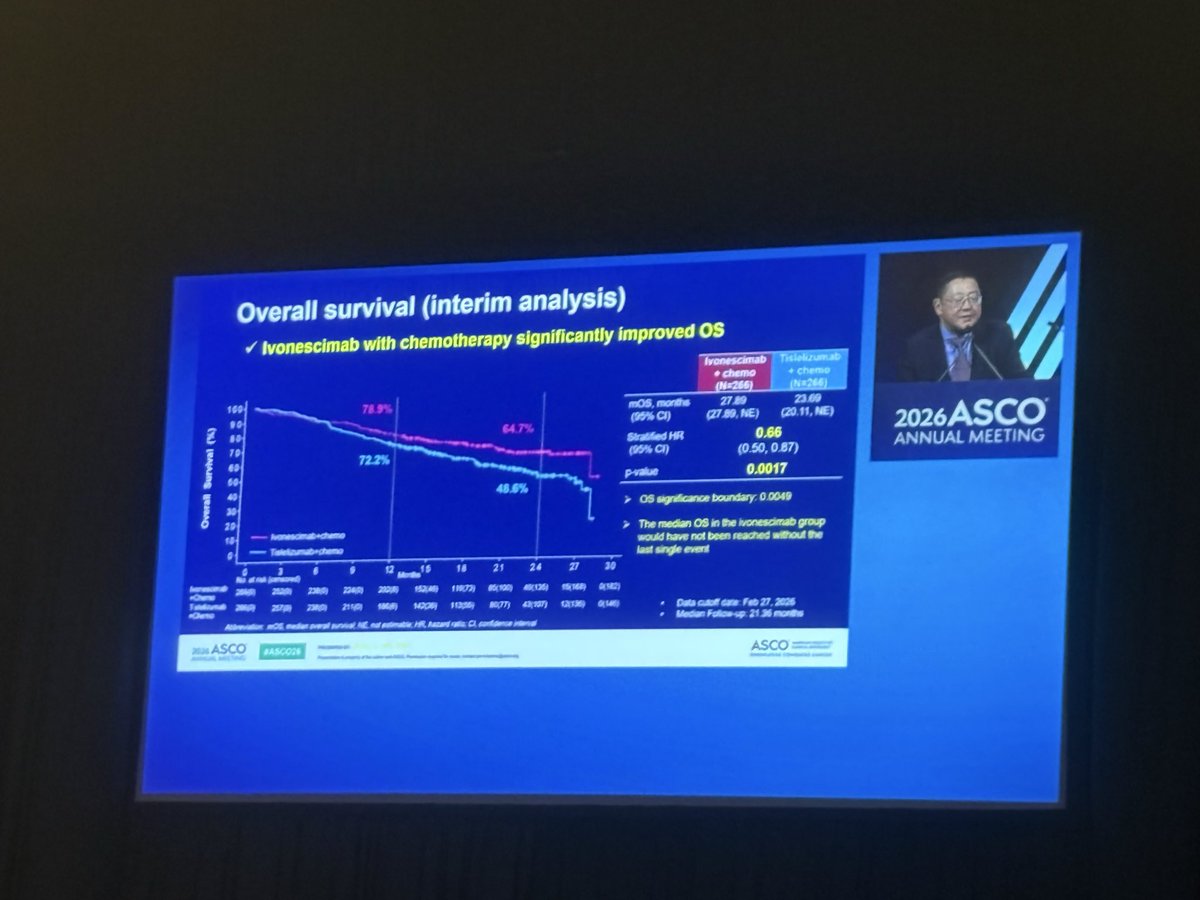
One of the most awaited presentations( at least by me) #ASCO26:
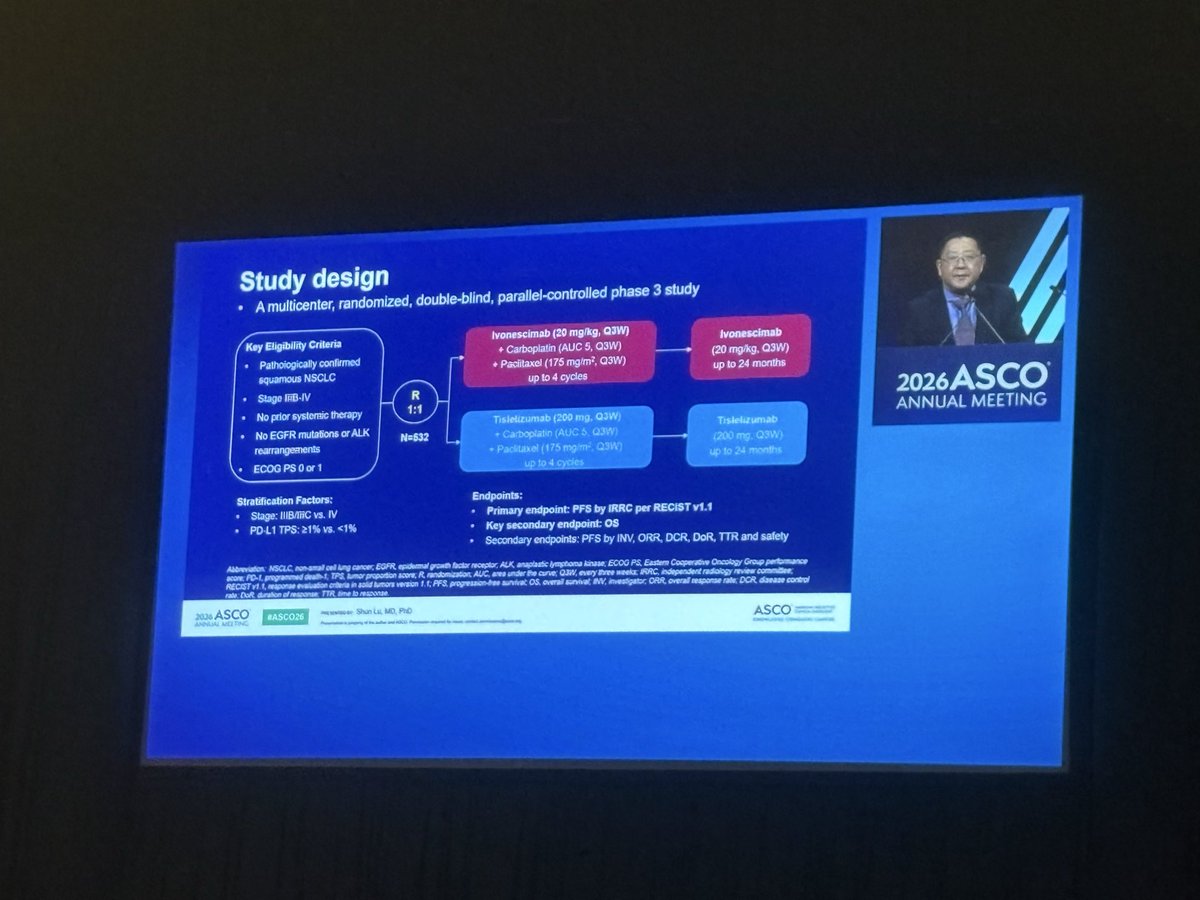
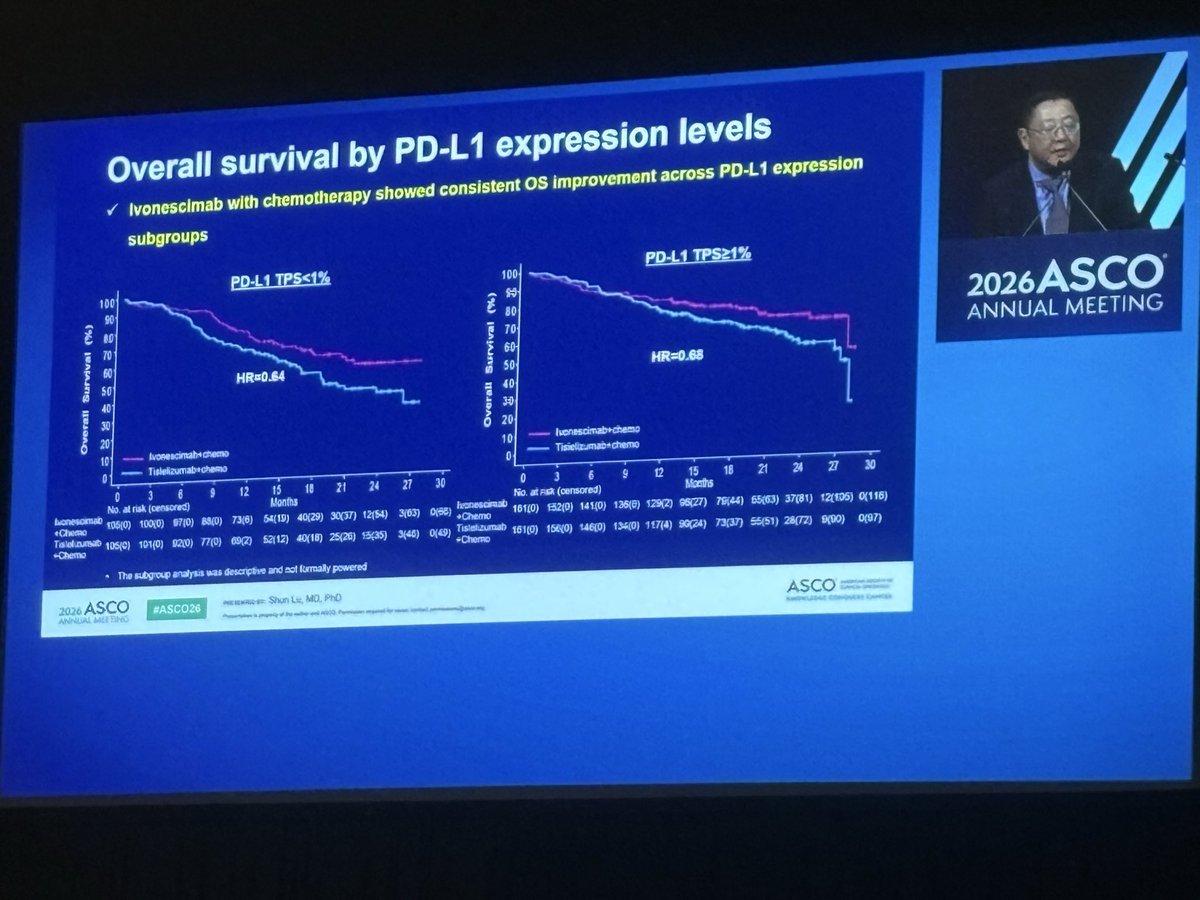
HARMONi-6 shows that ivonescimab + chemo significantly improves OS
Vs tislelizumab + chemo in first-line advanced Sq #NSCLC (HR 0.66).
A positive phase III study with a clinically meaningful OS benefit and simultaneous publication in @TheLancet:
https://t.co/2JR3fy4cL1
Caveat: this was a study conducted entirely in China. How these data will translate globally remains an important question? Let’s see what HARMONI 3 will show
Dr. Jun Gao presented a phase 1b/2 of Bulumtatug fuvedotin (BFv) + toripalimab in la/mUC: ORR 83%, DCR 89.4%, mPFS 12.9 mo, and 18-mo OS rate 68.1%. All CRs remained on treatment. Impressive efficacy signal for this novel Nectin-4 ADC + anti-PD-1 combo. #ASCO26#BladderCancer@OncoAlert@ASCO@OncBrothers
Our #ASCO26 podcasts are now available in Spanish! Thanks to the magic of AI translation, @tompowles1 and @brian_rini speak fluent (sort of) Spanish. Listen to our podcast on PROTEUS here and all ASCO podcasts on all major podcast platforms. @_SEOM@OncoAlert
https://t.co/7IUeZAU7Bb
Adjuvant nivolumab in high-risk muscle-invasive #UrothelialCarcinoma: Real-world evidence from the SOGUG-NIADY study of the Spanish Oncology Genitourinary Group (SOGUG). Presentation by Aurea Molina Diaz, MD. #ASCO26 written coverage by @RKSayyid > https://t.co/T0V3pBN1kJ @sogug1@ASCO
CaboNivo final results in non-clear cell RCC presented by Dr Darren Feldman: ORR 43% in Cohort 1 (papillary, unclassified, tRCC), with a striking 88% ORR in FH-deficient RCC. mPFS 11 mo, mOS 28 mo. No responses in chromophobe RCC. CaboNivo confirmed as a standard 1L option for these rare subtypes. #ASCO26 #RCC @OncoAlert@ASCO@OncBrothers
Unsung hero poster award for RCC. @OncHahn discusses muscle and fat changes in patient receiving either Len/Ev or Cabo with some interesting findings that complement standard toxicity data.


![Tony_Calles's tweet photo. Phase Ib results from the phase Ib/II study of [Lu]Lu-DOTA-TATE in combination with standard of care as a first-line treatment for pts with ES-SCLC.
☢️ Feasible but challenging combination. Hard to understand the contribution of Lu-DOTA-TATE in terms of efficacy. Ongoing phase II study no longer recruiting patients.
#ASCO25 #SCLC #LCSM](https://pbs.twimg.com/media/HJ0UkHpXgAAIjLD.jpg)
![Tony_Calles's tweet photo. Phase Ib results from the phase Ib/II study of [Lu]Lu-DOTA-TATE in combination with standard of care as a first-line treatment for pts with ES-SCLC.
☢️ Feasible but challenging combination. Hard to understand the contribution of Lu-DOTA-TATE in terms of efficacy. Ongoing phase II study no longer recruiting patients.
#ASCO25 #SCLC #LCSM](https://pbs.twimg.com/media/HJ0UkHoW0AA_s5o.jpg)
![Tony_Calles's tweet photo. Phase Ib results from the phase Ib/II study of [Lu]Lu-DOTA-TATE in combination with standard of care as a first-line treatment for pts with ES-SCLC.
☢️ Feasible but challenging combination. Hard to understand the contribution of Lu-DOTA-TATE in terms of efficacy. Ongoing phase II study no longer recruiting patients.
#ASCO25 #SCLC #LCSM](https://pbs.twimg.com/media/HJ0UkHmXAAAVs2m.jpg)










![urotoday's tweet photo. Subgroup analyses by disease volume and de novo/recurrent #mHSPC in the #PSMAddition study of [177Lu]Lu-PSMA-617. Presentation by Fred Saad, CQ, MD, FRCS, FCAHS @chumontreal. #ASCO26 written coverage by @RKSayyid @UAUrology > https://t.co/WlcyMVLacY @ASCO https://t.co/yoXm8Dygkr](https://pbs.twimg.com/media/HJvfKbiW4AAn-8g.png)
![urotoday's tweet photo. Subgroup analyses by disease volume and de novo/recurrent #mHSPC in the #PSMAddition study of [177Lu]Lu-PSMA-617. Presentation by Fred Saad, CQ, MD, FRCS, FCAHS @chumontreal. #ASCO26 written coverage by @RKSayyid @UAUrology > https://t.co/WlcyMVLacY @ASCO https://t.co/yoXm8Dygkr](https://pbs.twimg.com/media/HJvfJOGXAAA_2-d.png)
![urotoday's tweet photo. Subgroup analyses by disease volume and de novo/recurrent #mHSPC in the #PSMAddition study of [177Lu]Lu-PSMA-617. Presentation by Fred Saad, CQ, MD, FRCS, FCAHS @chumontreal. #ASCO26 written coverage by @RKSayyid @UAUrology > https://t.co/WlcyMVLacY @ASCO https://t.co/yoXm8Dygkr](https://pbs.twimg.com/media/HJvfH_oWcAAChG_.png)


























![Tony_Calles's tweet photo. Phase Ib results from the phase Ib/II study of [Lu]Lu-DOTA-TATE in combination with standard of care as a first-line treatment for pts with ES-SCLC.
☢️ Feasible but challenging combination. Hard to understand the contribution of Lu-DOTA-TATE in terms of efficacy. Ongoing phase II study no longer recruiting patients.
#ASCO25 #SCLC #LCSM](https://pbs.twimg.com/media/HJ0UkHqXMAAxH5V.jpg)





![urotoday's tweet photo. Subgroup analyses by disease volume and de novo/recurrent #mHSPC in the #PSMAddition study of [177Lu]Lu-PSMA-617. Presentation by Fred Saad, CQ, MD, FRCS, FCAHS @chumontreal. #ASCO26 written coverage by @RKSayyid @UAUrology > https://t.co/WlcyMVLacY @ASCO https://t.co/yoXm8Dygkr](https://pbs.twimg.com/media/HJvfLp7XQAAPgJ5.png)