@PWesslyMD@LucySafi@PriyaPanday27@NadeenFaza@ASE360@JournalASEcho Our group also identified a novel Doppler sign —Bifid-E wave— that could represent an additional echocardiographic marker of advanced MVP and myocardial fibrosis. Keep an eye out for this next time you're reading a Barlow Echo. #ASEchoJC
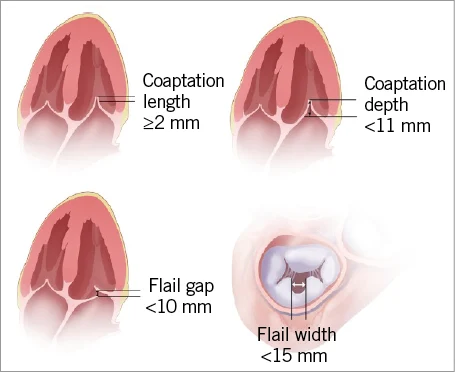
🫀 #CardioNugget: Flail Gap vs Flail Width in MR
📍 Flail Gap
➡️ Distance between the flail leaflet tip and the coaptation line
➡️ Think: “How far is the leaflet flying into the LA?”
🔴 Larger gap = more severe MR
✅ MitraClip-friendly: <10 mm
📍 Flail Width
➡️ Medial–lateral extent of the flail segment
➡️ Think: “How wide is the damaged portion?”
🔴 Wider segment = more complex repair
✅ MitraClip-friendly: <15 mm
🎯 Why it matters?
Both help determine severity + feasibility of transcatheter repair (e.g., MitraClip)
#CardioNuggets #MedEd #TEE #MitraClip
55 yr DM, admitted with chest pain, normal coronary , echo showed saddle shape thrombi, CTPE showed extensive bilateral PE, pan
CT showed prostate CA with extensive abd and pelvic lymphadenopathy,he underwent bil PA catheter-directed thrombosis.@echotalk, @EchoCases, @EchofirstB,
Adam Christian Thebesius 1686-1732
To get the coronary sinus (CS) in TEE slowly advance the probe from the mid-esophageal 4Ch view till the MV disappears and instead of it the CS appears #echofirst
By zooming in on the image the Thebesian valve can be occasionally seen
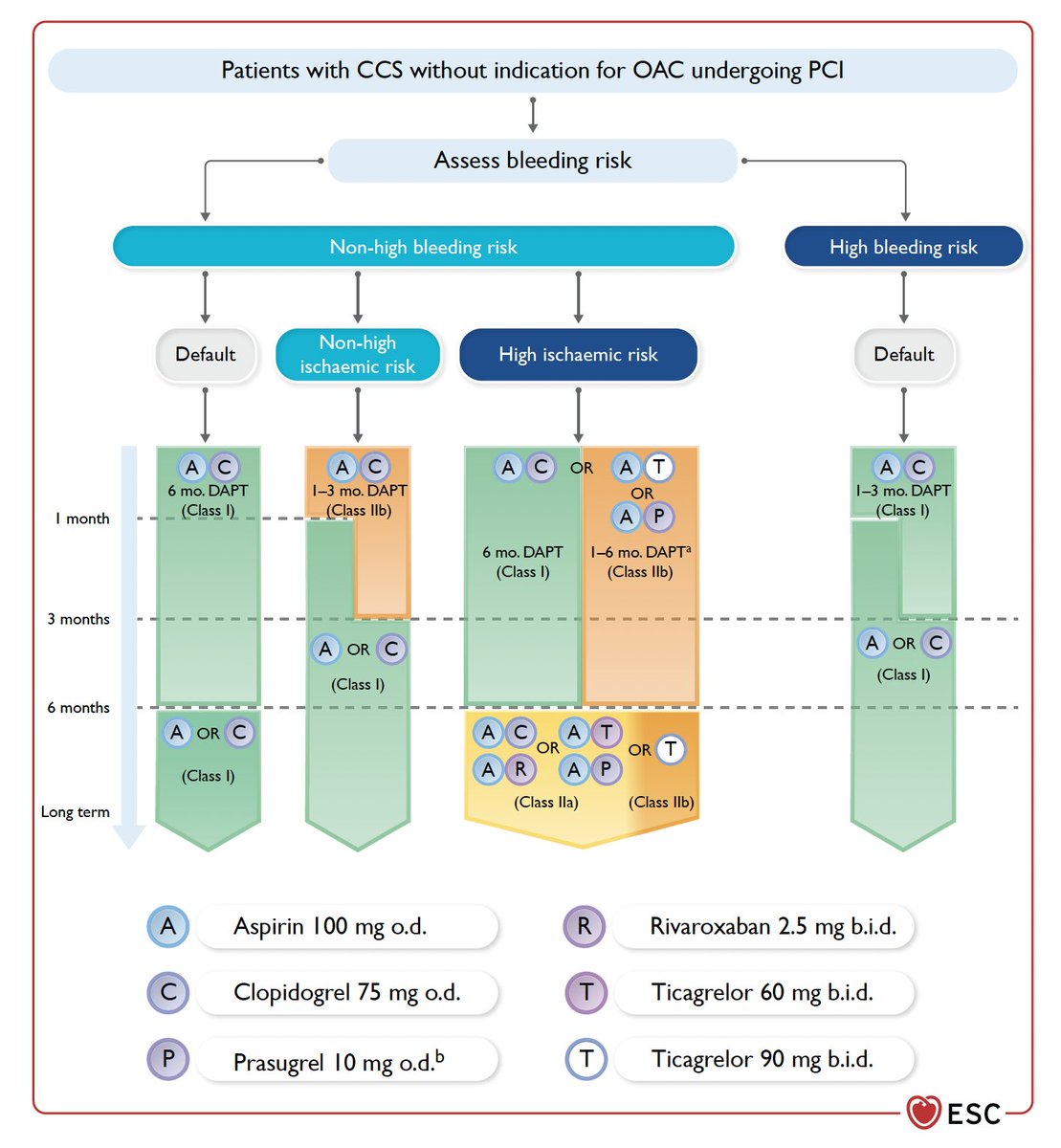
How many times have we seen this flow chart on the duration of DAPT change over the years? Let’s summarize the situation regarding class I recommendations (“must be done”) as reported in the new 2024 guidelines on chronic coronary syndromes:
- High bleeding risk patient: DAPT for 1-3 months.
- High ischemic risk patient with no high bleeding risk: DAPT for 6 months (alternatively 1-6 months in class IIb).
- Patient with neither high ischemic risk nor high bleeding risk: DAPT for 6 months (alternatively 1-3 months in class IIb).
I believe there is a missed opportunity for a recommendation regarding 'bi-risk' patients, but there is little evidence on this matter.
https://t.co/7RI6XRsdrd #ESCCongress
Having an elevated Lp(a) increases your risk of heart disease.
There are no currently approved therapies to Lp(a).
But that doesn't mean you cannot lower your risk.
Here's how
🧵👇
/1
#JADEL#10DaysofCASE
https://t.co/XGbMlfPyYw includes 31 reports (from Earth)!
MOVIE 2 of 31
A. Anomalous PV
B. Secundum ASD
C. Primum ASD
D. Unroofed CS
Details here:
https://t.co/twdHwxvgWl
#31ACHDMovies#ACHD
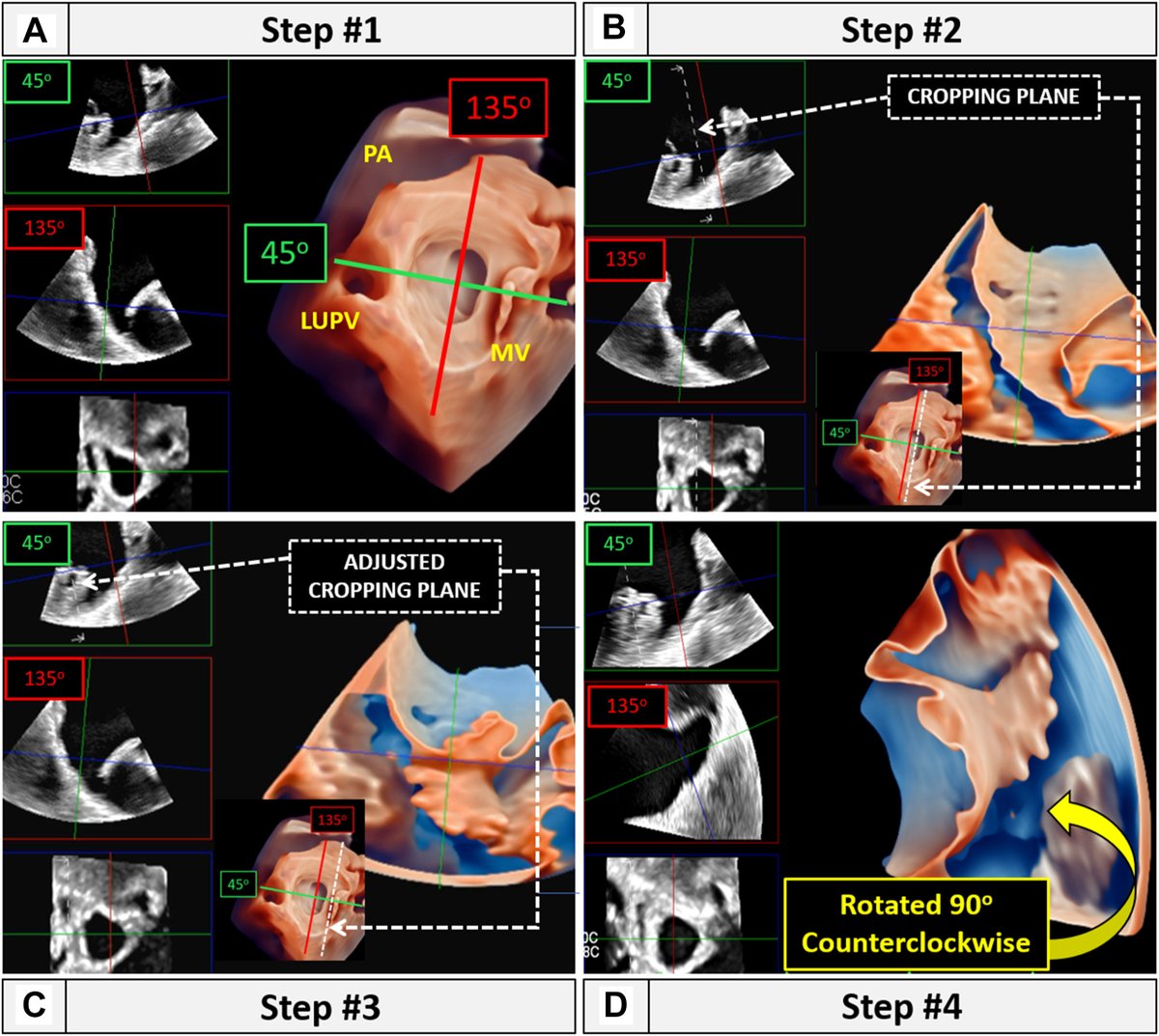
We have developed a simplified version of the below 3D TEE maneuver, which minimizes the number of image rotation and cropping steps.
We have termed this simplified version the 3D left atrial appendage (LAA) multiview (LAAM) technique. https://t.co/JtNVFOnmbo @CASEfromASE
QUIZ: A 68-year-old man with no known past medical history presenting w/ chest pain. The arrow points to which of the following? @CASEfromASE
A) Anomalous coronary artery
B) Unroofed coronary sinus
C) Ultrasound artifact
D) Coronary-cameral fistula
E) Aortic valve calcification
Textbook example of intramyocardial dissecting hematoma : pulsatile cavity with changing echogenicity, mobile endocardial border, clear ventricular myocardium border outside.
Unusual site of IE in iv drug abuser presented with fever, confusion, high inflammatory marker, CT brain showed multiple b/l stroke, blood grew staph. Aureus. Echo IE in tip of papilary muscle and AML. @echotalk@echocardiac@EchoCases@EchofirstB@echo
1/⚡️How to assess tricuspid valve by TOE #echofirst?
➡️What's the role of X-plane?
➡️How to get the best 3D image?
➡️Tips and tricks about transgastric view
➡️What we need to know about pacemaker lead
Take a look this thread 🧵
@NMerke@iamritu@hahn_rt@denisamuraru@lpbadano