Great to have Prof. @DrJNaidoo deliver the @IASLC Hot Topics Keynote address at her alma mater @tcddublin on state of the art immunotherapy now and in the future! #lcsm
🫁 Unresectable Stage III NSCLC: Current State of the Art.
The management of unresectable stage III NSCLC continues to evolve. cCRT remains the backbone of treatment, while consolidation durvalumab (PACIFIC) and osimertinib for EGFR-mutated disease (LAURA) have redefined the standard of care.
Precision radiotherapy and biomarker-driven strategies are shaping the next era of treatment.
📖 Am Soc Clin Oncol Educ Book
DOI 👉🏻 https://t.co/NCOmck4ZXI
#CánCare #NSCLC #lcsm #thoraciconcology #immunotherapy #precisiononcology
🫁 Immunotherapy Rechallenge in NSCLC.
The largest meta-analysis to date (10 RCTs, n=3,081) showed that PD-(L)1 rechallenge provided modest OS (HR 0.91) and PFS (HR 0.89) benefits, with no ORR improvement.
No benefit was observed in primary resistance, while patients with acquired resistance appeared more likely to benefit (OS HR 0.86).
Resistance phenotype matters.
📖 Cancer Treatment Reviews.
DOI 👉🏻 https://t.co/dX9gvaj5yP
#CánCare #NSCLC #lcsm #ThoracicOncology #Immunotherapy #ICI
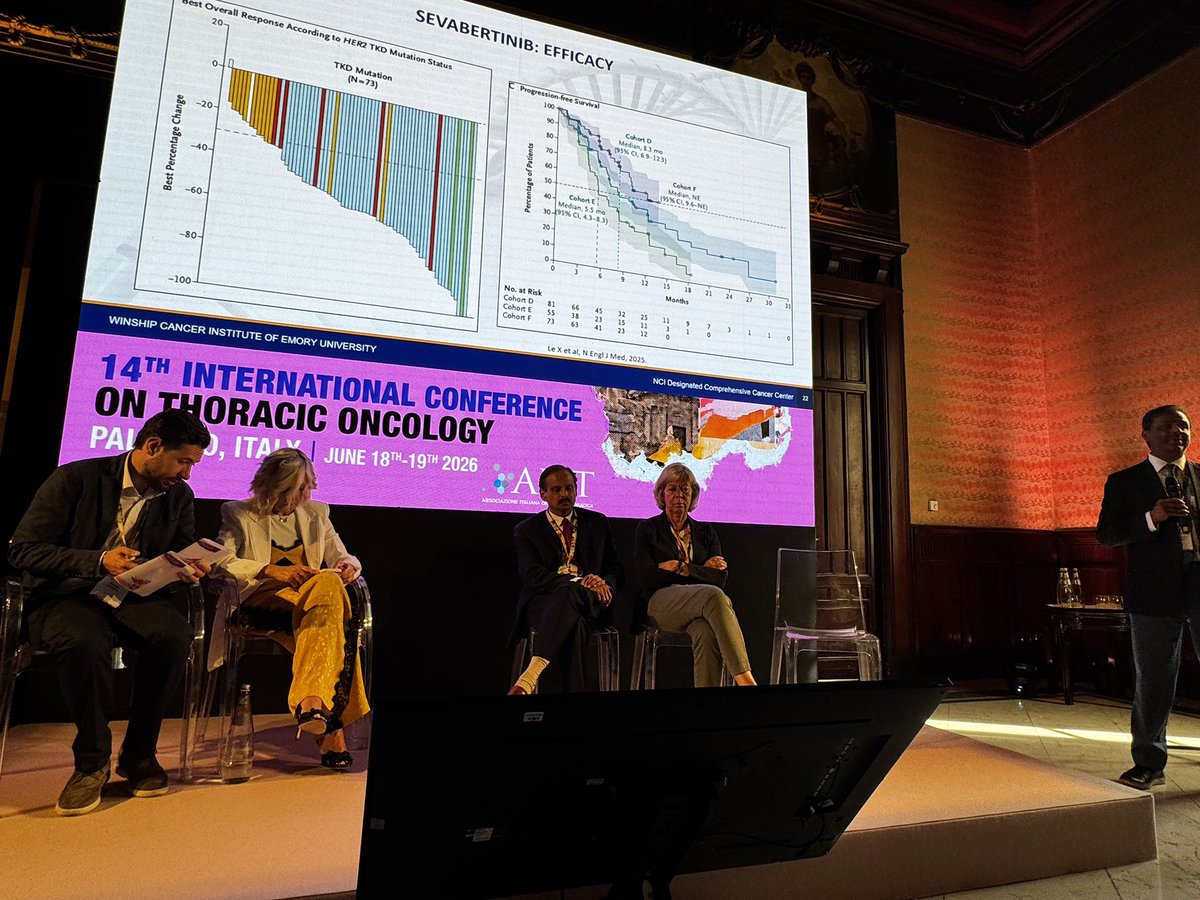
#CIOT26 Dr. @RamalingamMD compares the approved HER2 targeted agents for NSCLC. Trastuzumab deruxtecan first approved agent but oral options like sevabertinib very appealing and zongertinib now with approval as first line therapy. And for NRG1, zenocutuzumab preferred.
🫁 Another phase III trial is making the case for upfront treatment intensification in EGFR-mutated NSCLC.
AENEAS2 evaluated first-line aumolertinib ± platinum-pemetrexed in advanced EGFR-mutated NSCLC.
Study population:
EGFR Ex19del or L858R mutations
Treatment-naïve advanced NSCLC
ECOG 0-1
Stable brain metastases allowed
🔹 Aumolertinib
vs
🔸 Aumolertinib + platinum-pemetrexed → maintenance aumolertinib + pemetrexed
Results:
⏳ Median PFS
28.9 months vs 18.9 months
📉 53% lower risk of progression or death
HR 0.47 (95% CI 0.37-0.60)
🧠 Benefit seen in patients with brain metastases
🧬 Benefit seen in L858R-mutant disease
The trade-off?
⚠️ Grade 3-4 neutropenia
55% vs 1%
⚠️ Grade 3-4 thrombocytopenia
20% vs 1%
Clinical takeaway:
After FLAURA2, MARIPOSA, and now AENEAS2, the question is no longer whether intensification improves PFS.
The question is which patients should receive it upfront.
📖 Full paper in comment ⬇️
@asco@myesmo@oncoalert
#OncoTwitter #MedTwitter #NSCLC #LungCancer
Analysis using Korean insurance claims data: of 10,275 pts receiving immunotherapy for NSCLC, 7.6% complete planned 2y - no significant difference with various agents. Note that after 3y off therapy, 42% of pts received subsequent treatment.
https://t.co/3gJqGspuIv
Early morning learning from Dr. @ZPiotrowskaMD discussing new standards of care for HER2 mutant NSCLC. HER2 ADCs like T-DXd giving way in the first line setting to TKIs like zongertinib - but will the future for advanced HER2+ NSCLC be combinations?
🚨 Our phase 1b/2a study of fostrox + lenvatinib in pretreated advanced HCC is now published in @CCR_AACR@AACR
👉 Fostrox plus lenvatinib demonstrated promising efficacy as a 2L or 3L treatment for advanced HCC after prior ICI.
👉 ORR was 24%, DCR 81%, median TTP 10.9 months, median PFS 6.7 months, and median OS 13.7 months.
👉 Liver-targeted fostrox induced tumor-selective DNA damage without causing treatment-related liver function deterioration.
@ILCAnews@EASLnews@ASCO@myESMO
Full text: https://t.co/kuQF7PcsQ4
#HCC #LiverCancer #Immunotherapy #Fostrox #Lenvatinib #Secondlinetreatment
What did ASCO 2026 change?
Some standards of care have now moved by years.
That almost never happens.
BRAF colorectal, pancreatic KRAS, and DDLPS sarcoma
are three of oncology's hardest diseases
SOC moved by > 1yr:
▫️BRAF mCRC: 15.1 → 30.3 months OS
▪️Pancreatic KRAS: 6.7 → 13.2 months OS 🏆
▪️DDLPS sarcoma: 1.5 → 9.7 months PFS ⭐️
(sarcoma went from "nothing" to a win).
Myeloma, GIST, HR+/HER2- breast, uveal melanoma, bladder, prostate, and RET+ lung cancer moved too.
This is what decades of funded science look like when it compounds.
- - - - -
Source: Jori (@jori_health)
𝘗𝘭𝘰𝘵 𝘱𝘦𝘦𝘳-𝘳𝘦𝘷𝘪𝘦𝘸𝘦𝘥 𝘣𝘺 𝘦𝘪𝘨𝘩𝘵 𝘰𝘯𝘤𝘰𝘭𝘰𝘨𝘺 𝘦𝘹𝘱𝘦𝘳𝘵𝘴. 𝘛𝘩𝘢𝘯𝘬 𝘺𝘰𝘶 <3
- - - - -
🚨 Stage III unresectable NSCLC has quietly become one of the biggest precision oncology success stories.
A decade ago:
➡️ Median OS ~2 years
Today:
✅ PACIFIC: mOS 47.5 months
✅ LAURA: mPFS 39.1 months in EGFR-mutant disease
✅ 5-year OS approaching 43%
The key lesson?
Every patient needs upfront molecular testing.
🧬 EGFR-mutant → Osimertinib
🛡️ EGFR wild-type → Durvalumab
The era of “all stage III patients get the same treatment” is over.
Full paper in comment below ⬇️
#OncoTwitter #MedTwitter #LungCancer @OncoAlert@myesmo@esmo_open@JCO_ASCO
Negative phase III trial of concurrent thoracic RT in ES-SCLC receiving chemoimmunotherapy.
TRT was initiated early (between cycles 2 and 3), and failed to improve outcomes:
• Median OS 10.0 vs 11.8 months
• No improvement in response rate
• More adverse events and treatment-related deaths While disappointing, these results should not be extrapolated to all consolidative TRT strategies. One key difference from SAKK 15/19 is timing: RT here was delivered concurrently with ongoing chemoimmunotherapy, whereas SAKK 15/19 administers TRT after completion of induction treatment and no major toxicity was detected
Perhaps the lesson is not that thoracic RT has no role, but that timing matters. https://t.co/njhvrV4590
#ASCO26 #SCLC #LungCancer #Radiotherapy
Human scientific ingenuity and hardwork, not AI. Human clinical trialists and patients, not AI
The standing ovation at #ASCO26 for the unprecedented results in metastatic pancreatic cancer with daraxonrasib an oral RAS inhibitor is the result of research excellence and perseverance, and a witness to this.
AI won’t do the work or run the trials to make these advances. It can make the process easier in the future. But you still need human ingenuity and hard works to take a chemical and make it an effective approved medicine.
Institutions and companies must nurture the human talent. Academic medicine is bleeding talent. Leaders are appointed for pliability over excellence. With NIH funding of new investigators at an all time low, coupled with institutions and organizations extolling the efficiencies and prioritizing the virtues of AI, we are at risk slowing down our ability in drug development.
https://t.co/2YRwESyIuu
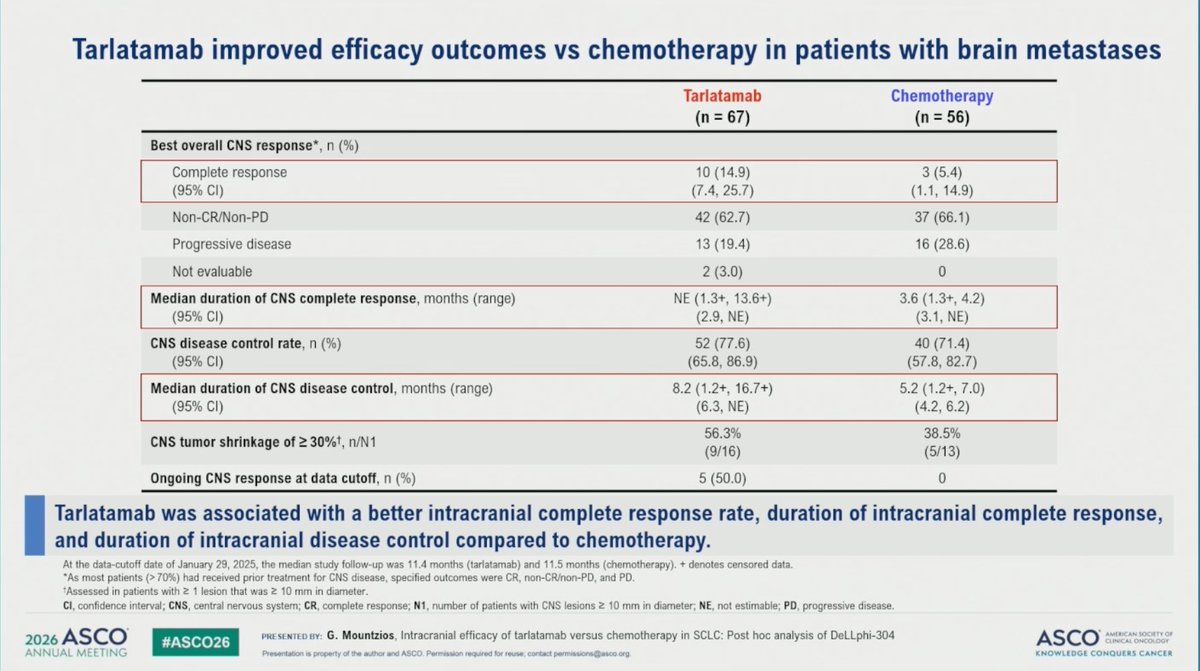
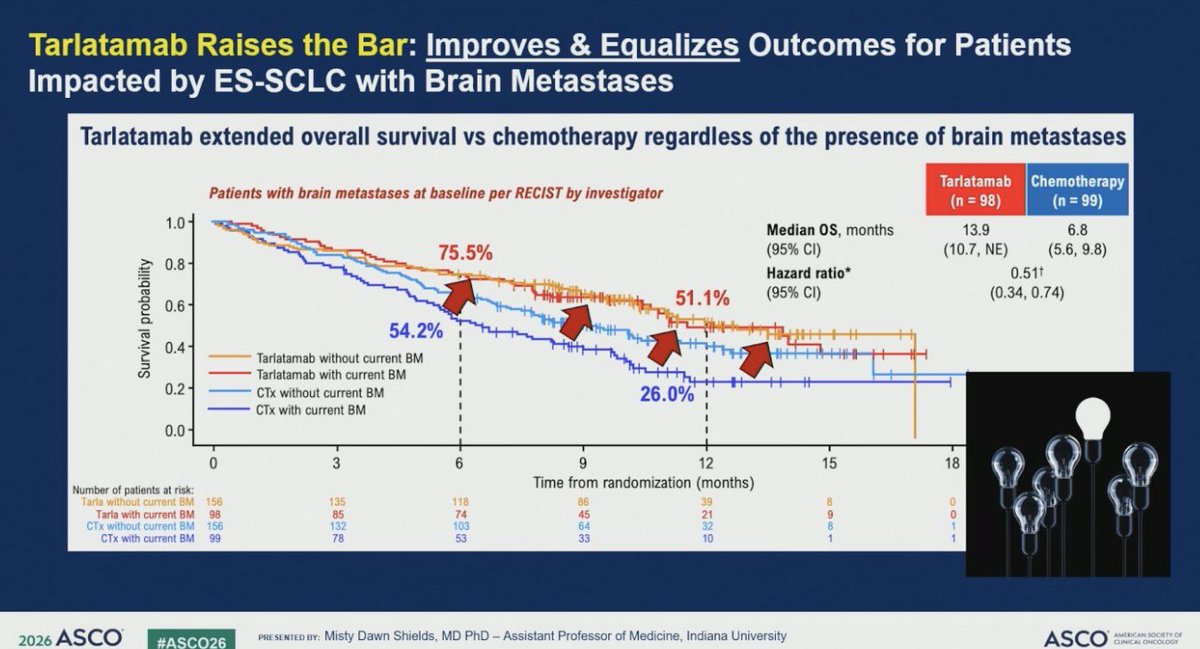
Dr. @drshieldsmd gives a great discussion on SCLC at #ASCO26. Tarlatamab update shows the drug raises the bar but points out importance of ICANS awareness. Is it higher in its with brain metastases?
As many other oncologists will also attest, we were taught this was a dead end
It was, dogmatically, never going to work — kras was too much of a “greasy ball” to be targeted
And yet here we are, with truly meaningful survival curves👇
Inspiration on multiple levels #ASCO26
#ASCO2026 | LORIN Phase II
Neoadjuvant lorlatinib in stage III ALK+ NSCLC delivered impressive results:
pCR 47%,MPR 81%,ORR 84%, 75% surgical conversion in initially unresectable disease
Small, single-arm study? Absolutely. Randomized confirmation needed? Of course.Practice changing? Debatable.
But if I see a stage III ALK+ patient tomorrow, these data would be very hard for me to ignore. I probably wouldn’t hesitate to discuss a neoadjuvant ALK-directed approach at the MDT.
#LungCancer #NSCLC #ALK #Lorlatinib #PrecisionOncology #ASCO26