Radiologists are the smartest doctors I know, but with all due respect, AI will hit them the most. Attended a lecture by a top gastro from AIG on how AI has been diagnosings CTs and MRCPs better than world renowned Radiologists. Mind blown
@aditya_gan3500 Unfortunately despite multiple checks by different peoples (doctors, nurses), consent forms, WHO checklists, never events still happen in every system. In my practice, where laterality is important, my final check is asking the patient for the last time while skin-marking.
Overall solid advice - Tailor it to your specialty and specific life goals.
If you are confident in your skills and satisfied with training, you need to crack on and build a practice.
If you want to learn more/subspecialise, think about how much time you need as an SR.
For those of you who have recently passed the MD/MS exam and want to get into private practice but are doing senior residency, you need to ask yourself some hard questions.
Why are you doing an SRship?
https://t.co/fxOLH3Frsk want to learn more
Fair enough. But do you really need three years for that? Won’t six months or one year suffice?
https://t.co/QUzemYgMmb want to keep the option of getting into a faculty position open
That is a weak reason. By now, you know both the pros and cons of the system. You are probably just delaying a decision by trying to ride two boats at the same time.
3.Because you got an SRship
That is even worse. This is the default approach to a career. You should be doing what is aligned with your long term goals.
As a young doctor, you should be spending your energy building your name and your practice. The comparative comfort that comes with an SR ship also comes at a cost.
In private practice, the earlier you start, the better you become at handling the initial tough months. Do not assume that just because you trained at a big institute, patients will make a beeline for you. Building a practice takes time.
You have to figure out how to build a team, how to handle finances, how to negotiate rent, and above all, how to get patients.
Start early so that you get time to figure out all these aspects.
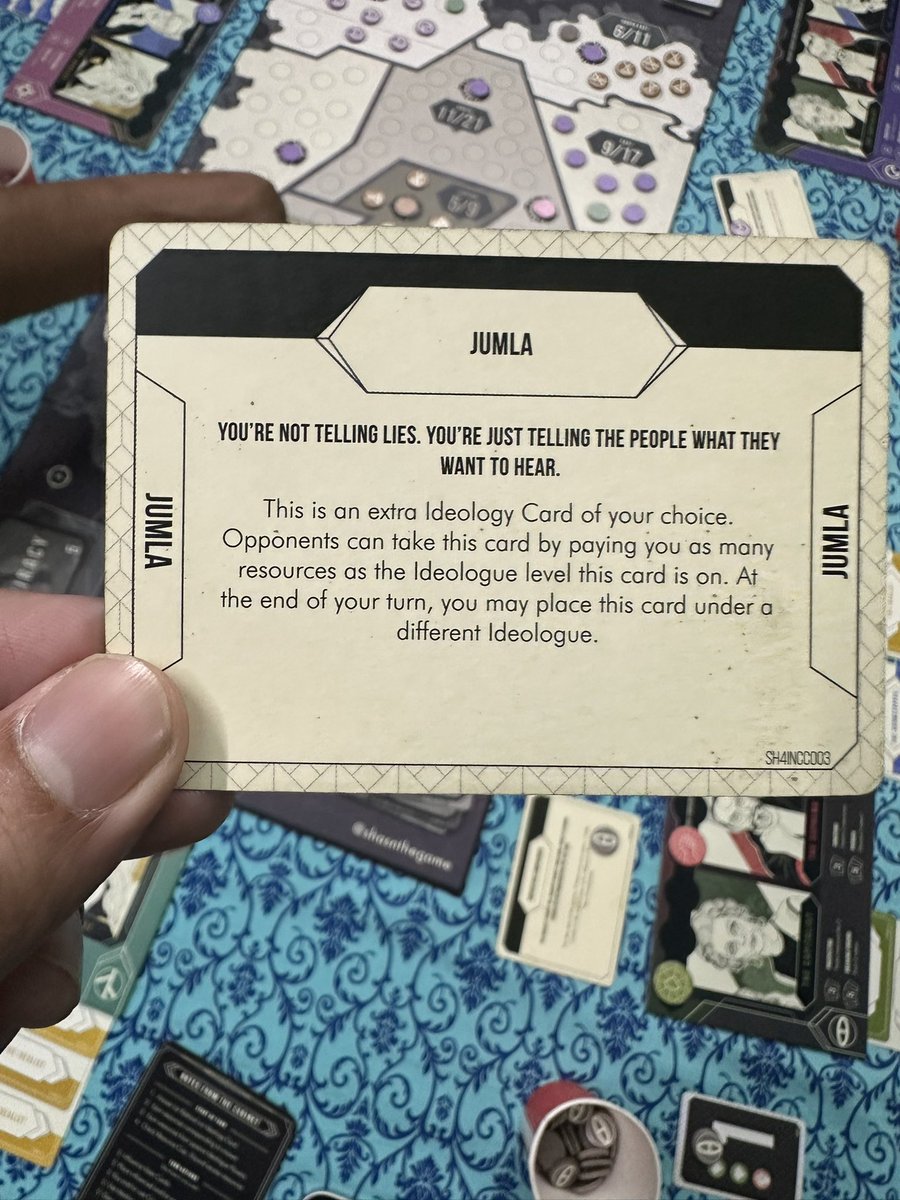
Quick rules question on Jumla @zainmemon_ : if we play this Conspiracy card, can it be used at the start of our turn so we earn resources from the extra Ideology card, or does it only activate during turn actions (meaning no resources that turn)?
@Drpoojadutta@drpraveenpsy I fail to see why him reminiscing about what he personally considers a period of struggle in his life prompts you to defend something that he does not criticise in the first place. Let’s stop here before it gets silly. Well done on realising your American dream. Have a good day.
@Drpoojadutta@drpraveenpsy The post is a personal reflection on @drpraveenpsy experiences and challenges. It offers no recommendations or warnings. Interpreting this as a critique of the US healthcare system is not only disingenuous but also serves to invalidate his lived experiences.
@DrAditya2935 That attitude is insufferable. But thankfully, that’s a loud subset, not the whole category. Most NRIs don’t need to construct a superiority narrative to feel at peace with their life choices. Plenty manage to appreciate their adopted country without critiquing their home.
@aditya_gan3500@Dr_S_Arora@medalityhq It is as Shubham says. These days CTs acquire volumetric data. So after the machine spins, it gets a continuous spiral 🌀 of data which it then reconstructs. And all scans use multiple detectors = MDCT. HRCT is historical - now we use lung kernel reconstructions.
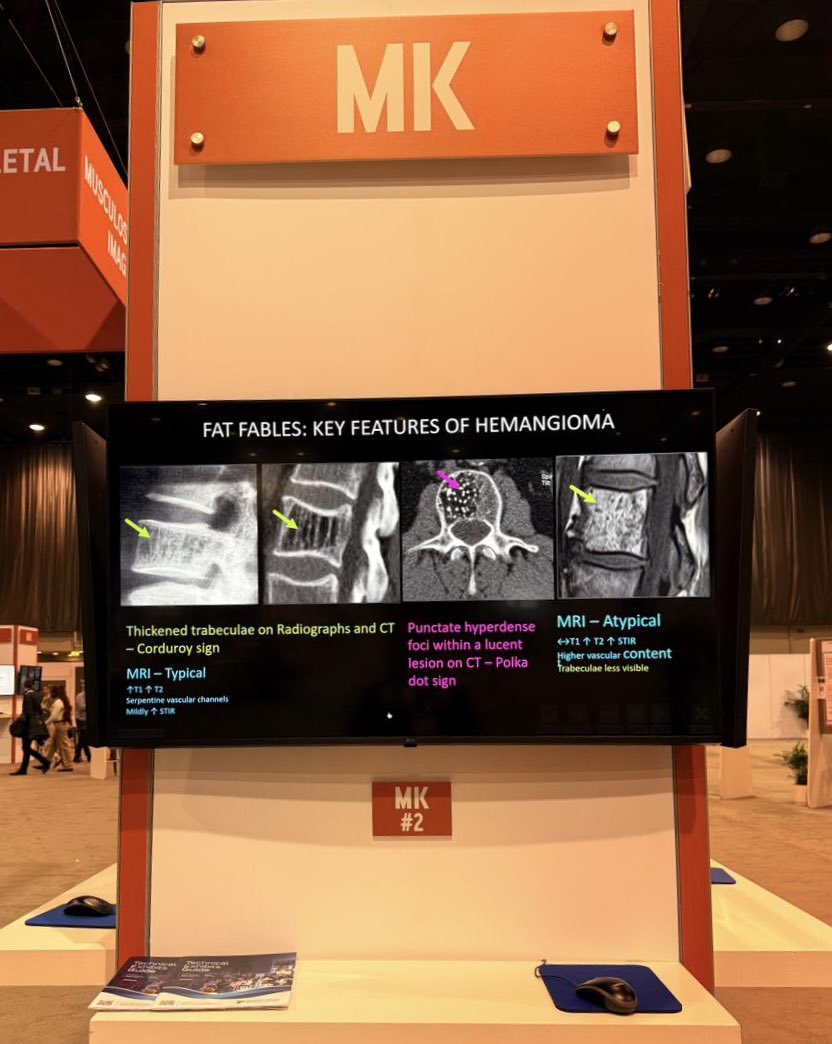
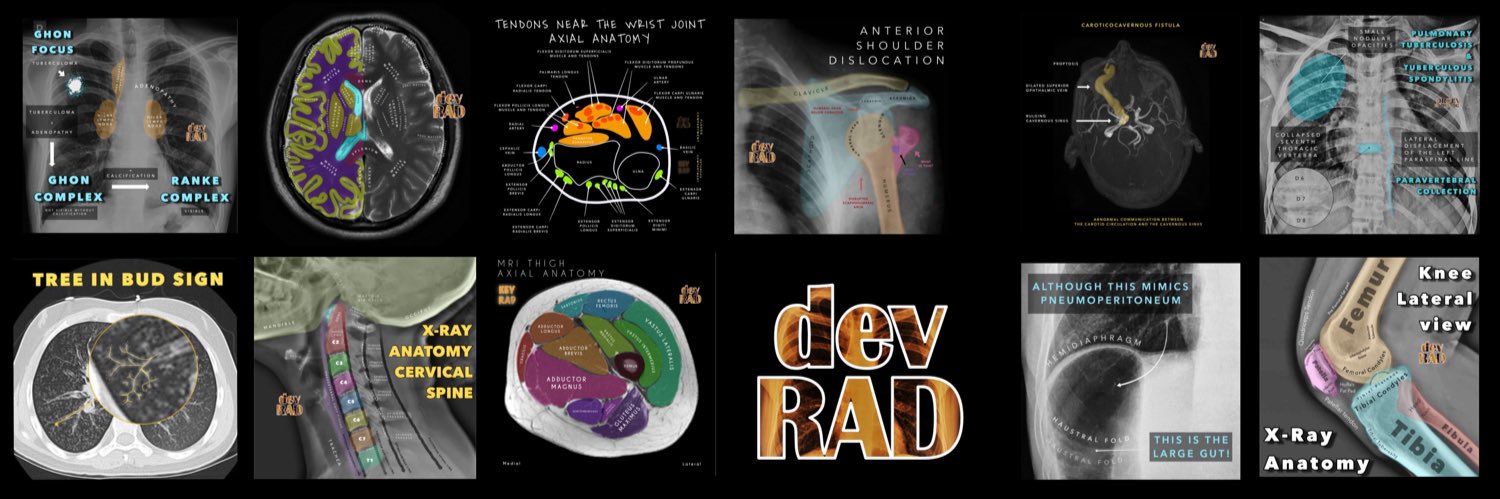
Feel free to check out our @RSNA exhibits are up in Chicago!
While I couldn’t be there, my amazing colleagues are holding the fort and sending me photos. So happy to see this…with a tiny bit of FOMO!
@samrad77@AliShahMSKRad@mskradiology4u1
@KitPeacock@trentconsultant@owenjonesjourno I don’t remember if I read it somewhere or a colleague said it during a discussion (on autopsy data, perhaps?) but close to 80% of men in their 80s have some degree of prostate cancer. Only a small percentage of that becomes clinically relevant.
@Geeky_Foodie The em-dash is a dead giveaway. I make it a point to remove that and introduce incorrect punctuation when I am using LLMs just so it looks more real 🥹
@Geeky_Foodie@Sona_unplugged Not with teleradiology as the degree of access you have to clinical information/ordering clinician is unreliable - depends on company, hospital, time etc. In the hospital, I can always access the EPR or call someone - takes time but atleast I know of a way out. With tele 🤷🏻♂️
Take some time to figure out the how instead of just how much.
When comparing incomes in specialties, remember that 💰 isn’t made in a vacuum. It comes with its own bill - your time, sleep, family, hobbies, and pieces of your health are all variables.
That nobody can define what these are is precisely the reason this fuels (and will continue to fuel) discussions and arguments every day. We all need a solid basis to judge others, and these topics are ripe for the picking.
This is a list of entities that Indian #MedTwitter talks about daily
But nobody can define them or even describe them well
1. Good doctor
2. Terminal subject
3. Best branch
4. Work life balance
5. Good bedside manner
6. Good clinical skills
Please add more
#MedTwitter
#NeuroTwitter
@Geeky_Foodie@Sona_unplugged I feel you. Totally chose radiology with the dream that I will be a slob and report from home in shorts but I underestimated my aversion to insufficient clinical information and affinity for procedures both of which prevent me from becoming 100% teleradiologist.