🧠🩺 Onco-Nephrology is no longer optional. It is essential.
Cancer patients are living longer.
Kidney toxicities are rising.
Decisions are getting harder.
This excellent CKJ review lays out 10 practical tips for running an effective onco-nephrology clinic 👇
🔹 Measure GFR correctly
Creatinine alone misleads. Combined Cr + Cys or measured GFR changes dosing, eligibility, and toxicity risk.
🔹 Not every creatinine rise = AKI
Many TKIs and targeted agents cause pseudo-AKI by blocking tubular secretion. Do not stop effective cancer therapy blindly.
🔹 VEGF inhibitors hit the kidney spectrum
HTN → proteinuria → TMA. Early nephrology input prevents irreversible damage.
🔹 ICI-AKI is usually steroid responsive
Early steroids improve recovery. Biopsy matters in complex cases to avoid over or under treatment.
🔹 Steroid-refractory ICI-AIN exists
Infliximab is emerging as a key steroid-sparing option in selected patients.
🔹 Transplant patients are not excluded anymore
With optimized immunosuppression, ICIs can be effective with acceptable rejection risk.
🔹 Plasma cell disorders deserve early transplant referral
MM and AL amyloidosis patients on dialysis can achieve meaningful survival post kidney transplant.
📌 Bottom line
The goal is not just kidney rescue.
It is safe continuation or timely re-initiation of cancer therapy.
#OncoNephrology #MedTwitter #Oncology #Nephrology #CancerCare
@OncoAlert@ASCO@ESMO_Open@myESMO
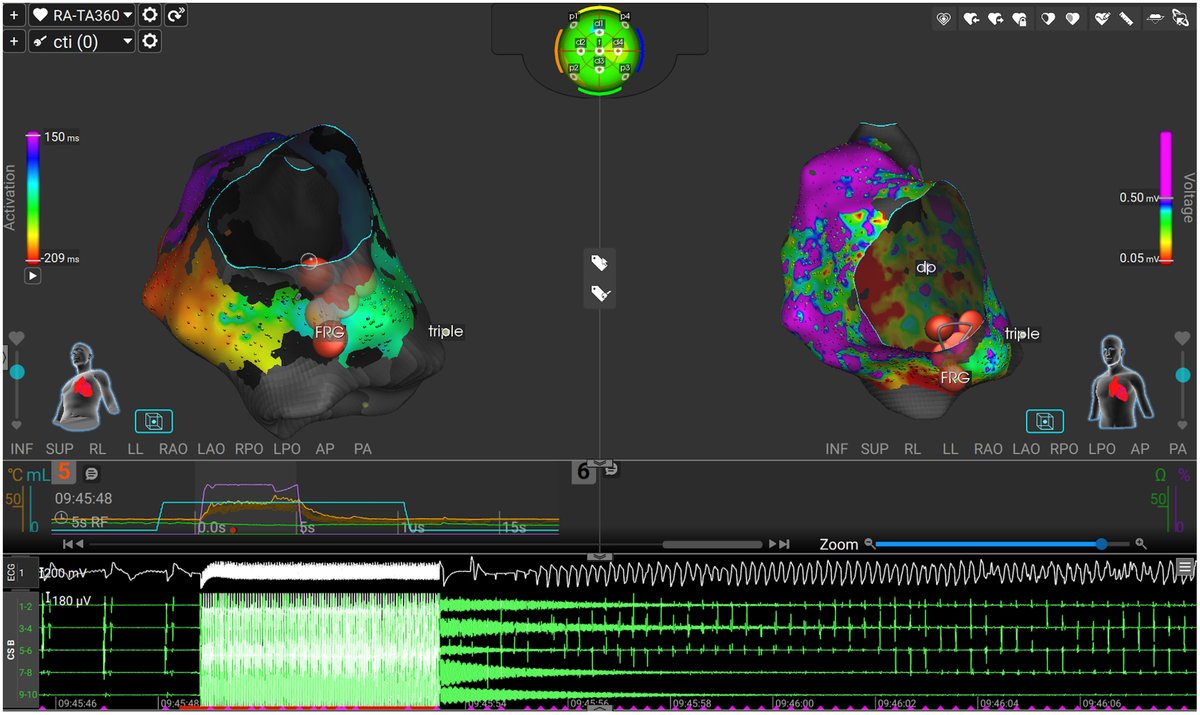
Ventricular Fibrillation Triggered by Cavotricuspid Isthmus Radiofrequency Ablation with a Dual-Energy Lattice-Tip Catheter in a Patient with an Implantable Cardioverter-Defibrillator
@SCYap77
https://t.co/1gJ9RVPIZe
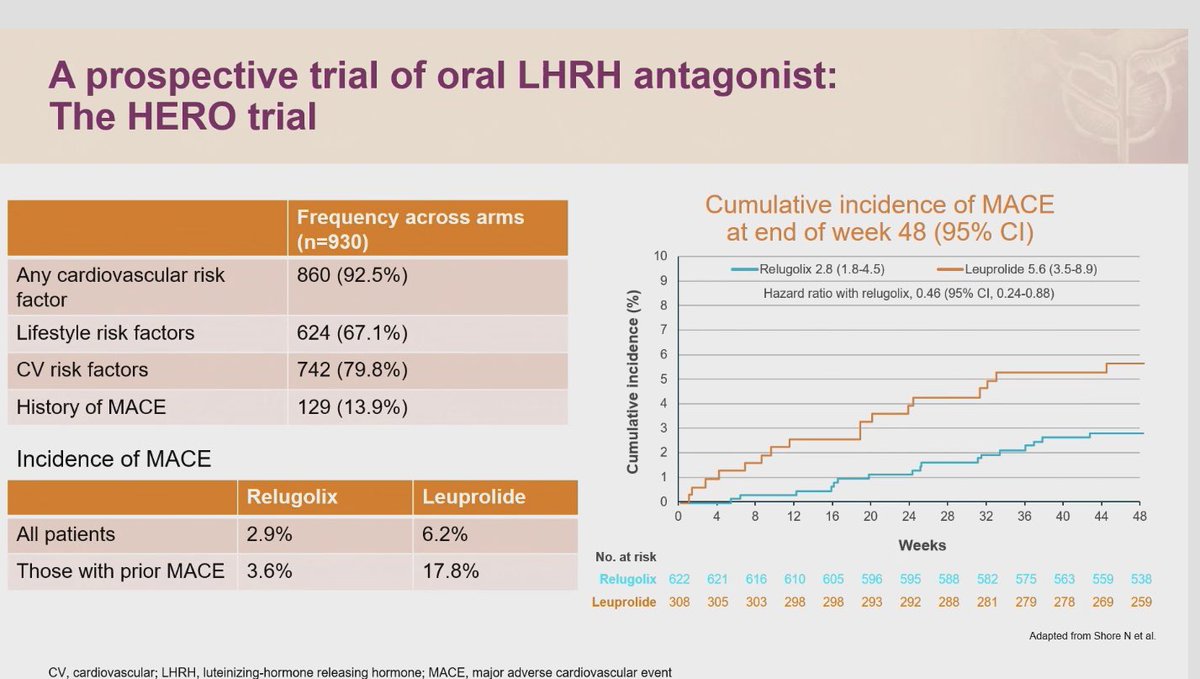
🫀 ADT choices and cardiovascular risk in prostate cancer
#GlobalForum25#PROSCA25
Men on ADT live long enough for CVD to become a major competing risk. Today’s reminder hits hard for daily practice.
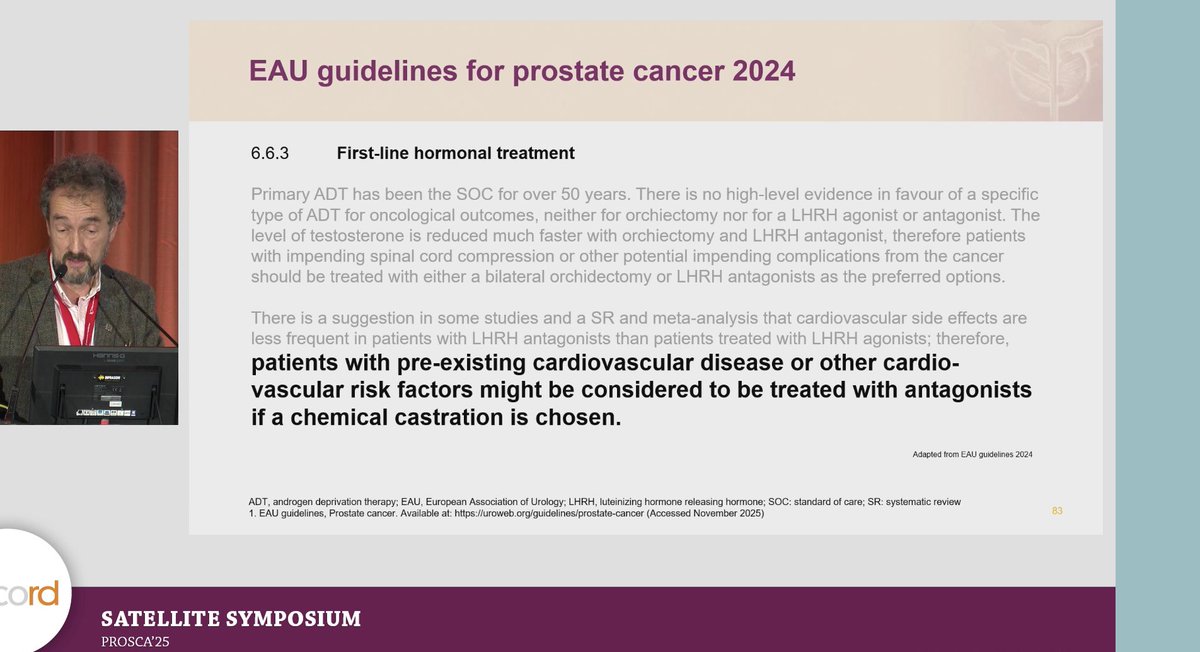
💡 EAU 2024 says
Patients with pre existing CVD or strong CV risk factors may be better treated with GnRH antagonists if chemical castration is planned.
💊 HERO trial insights
Regulatory antagonist (relugolix) showed:
😮💨 2.9 percent MACE vs 6.2 percent with leuprolide
In men with prior MACE, difference was 3.6 percent vs 17.8 percent.
🧬 Why antagonists may be safer
No flare
Faster testosterone suppression
Less endothelial stress and inflammation signals
📌 Clinical takeaway
Cardiovascular health should guide ADT choice.
Take note, monitor, and manage CV risk at every visit.
#OncoTwitter #MedTwitter #ProstateCancer #GU25
@OncoAlert@myesmo@esmo_open@asco@mirrorsmed
This JAMA Oncology Patient Page describes the 3 main types of urinary diversions and care required after surgery to ensure an active and fulfilling life. https://t.co/ccimk5e5fE
🧬 Atezolizumab + bevacizumab in MSI-like mCRC (phase II)
🎯 ORR 38.6% in the MSI-like cohort
🔥 MSI mCRC: ORR 65.2%
⚠️ MSS mCRC: ORR 9.5% (mainly without liver mets)
⏳ Median PFS: 23.2 mo (MSI) vs 4.0 mo (MSS)
💡 MSI-like GES does not enrich for sensitivity beyond standard MSI
🔗 https://t.co/YHWcnkmycE
🔥 New JAMA Oncology study: The hidden burden of metastatic recurrence in AYAs (15–39 yrs)
Even without metastasis at diagnosis… 1 in 10 adolescents & young adults STILL develop metastatic recurrence.
And survival is often worse than de-novo stage IV.
🎯 Key Findings (48,406 patients, 2006–2018)
📌 5-year metastatic recurrence (after early-stage diagnosis):
•Sarcoma: 24.5%
•Colorectal: 21.8%
•Cervical: 16.3%
•Breast: 14.7%
•Stage III (all cancers except thyroid): >30%
📈 Cervical cancer recurrence is rising - from 12.7% → 20.4%
📉 Colorectal & melanoma recurrence falling over time.
💀 Survival after metastatic recurrence vs metastatic at diagnosis
Worse in almost every cancer type:
•Breast: HR 2.87
•Cervical: HR 2.10
•Melanoma: HR 1.61
•Sarcoma: HR 1.57
•Colorectal: HR 1.53
🔥 Only testicular & thyroid cancer were exceptions.
Late recurrence (≥24 months) = better prognosis in breast/cervix
Late recurrence = worse in testicular/thyroid.
🧠 Why this matters?
AYA survivors often “graduate” from oncology follow-up early.
But this data shows:
Metastatic recurrence is common, deadly, and varies hugely by cancer type + stage.
This is a survivorship problem, not just a treatment problem.
A must-know dataset for oncologists, registries, policy makers, and AYA survivorship programs.
📖 Full study in comment ⬇️
#OncoTwitter #AYAOncology #CancerSurvivorship #CancerEpi #OncologyResearch
@OncoAlert@ESMO_Open@myESMO@ASCO
🎯🎯.- How to apply the current evidence in the treatment of mCSPC!! Excellent review.🙌
https://t.co/OFccsZ439w
👉.- The new molecular precision "triplet intensification" is here.
👉.- A HRR (BRCA2+) alt and pTEN loss population have a poor prognosis.
👉.- We need to better biomarkers profile in this setting
@OncoAlert@APCCC_Lugano@ANZUPtrials@myESMO@GuardConsortium@fedelosco
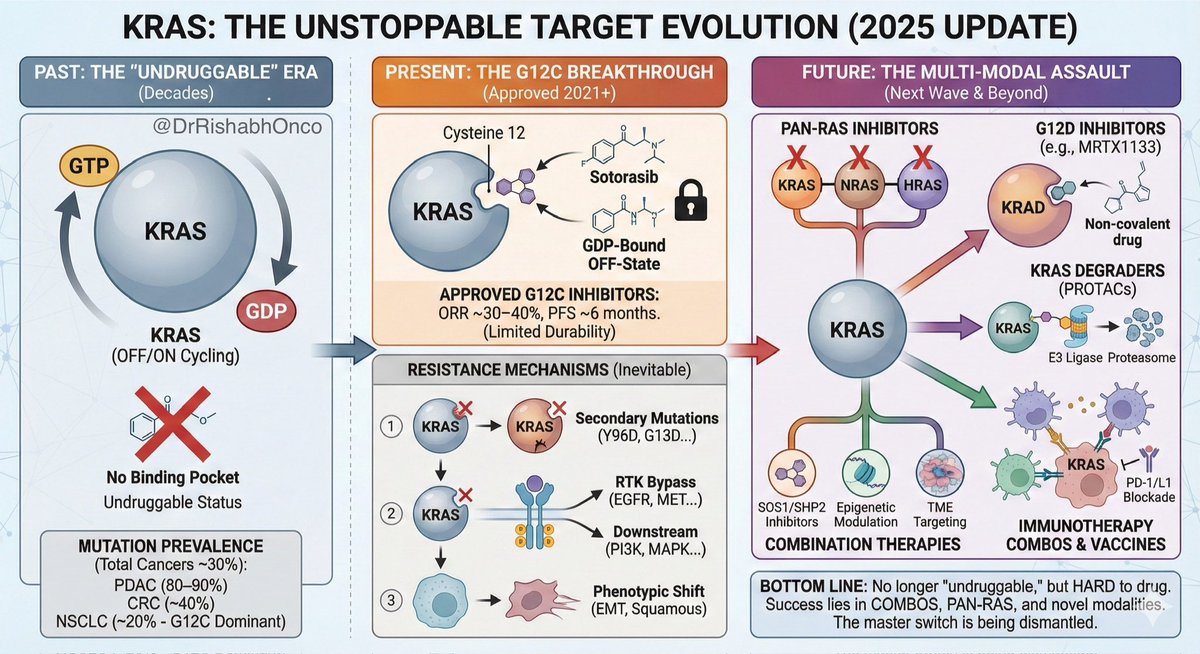
🚀 KRAS: From “Undruggable” to the Hottest Target in Oncology 🔥🧬
KRAS is the most mutated oncogene in cancer - yet for decades it was “undruggable.”
2025 marks a turning point.
A brand-new Signal Transduction & Targeted Therapy review lays out the ENTIRE evolution:
• Why KRAS drives PDAC, CRC, NSCLC
• Why G12C inhibitors work but only partly
• Why resistance is inevitable
• What the next wave of KRAS therapies looks like
🔑 Key takeaways:
🧩 KRAS mutations = ~30% of all cancers
– PDAC: 80–90%
– CRC: ~40%
– NSCLC: ~20% (G12C dominant)
🧬 Approved “OFF-state” inhibitors:
•Sotorasib
•Adagrasib
➡️ ORR ~30–40%, PFS ~6 months.
➡️ Resistance? Guaranteed.
🔥 Major resistance mechanisms:
– Secondary KRAS mutations (Y96D/S, G13D, A59…)
– RTK pathway upregulation
– EMT & squamous transformation
– KRAS amplification
– KEAP1/STK11/TP53 co-mutation biology
💡 The future = multi-modal KRAS targeting:
– Pan-RAS inhibitors
– G12D inhibitors (MRTX1133-like)
– SOS1/SHP2 inhibitors combos
– KRAS degraders (PROTACs)
– KRAS vaccines & cell therapies
– RNA & antisense therapeutics
🧠 The review beautifully shows KRAS as a signaling “master switch” with MAPK, PI3K, Ral, RAC1, Hippo/YAP-TAZ crosstalk explaining why single-agent inhibition fails.
🎯 Bottom line:
KRAS is no longer undruggable - it’s just very hard to drug.
The next breakthroughs will come from combos + pan-KRAS + epigenetic modulation + TME targeting.
🔖 Save this - it’s THE 2025 roadmap for KRAS-targeted therapy.
📖 Full paper cited below.
#OncoTwitter #MedTwitter #LCSM #GIOnc #TargetedTherapy @myESMO@OncoAlert@ESMO_Open
Guía básica para leer una revisión sistemática + metaanálisis y aplicar los resultados a los pacientes.
Una guía obligada para los profesionales de la salud.
https://t.co/uGgEd3p9BF
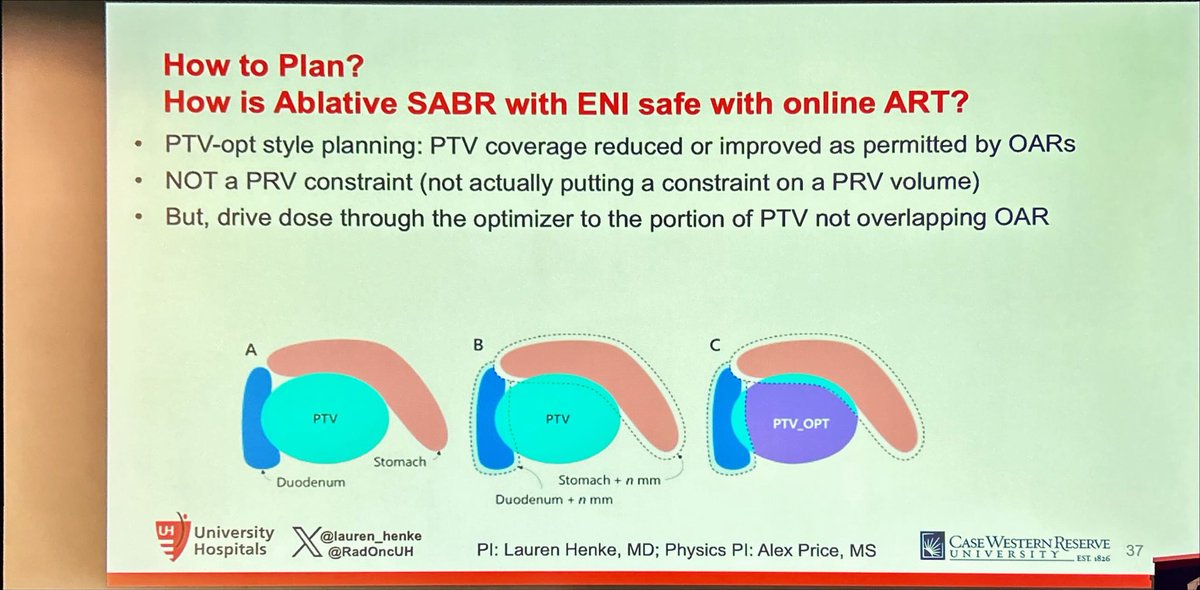
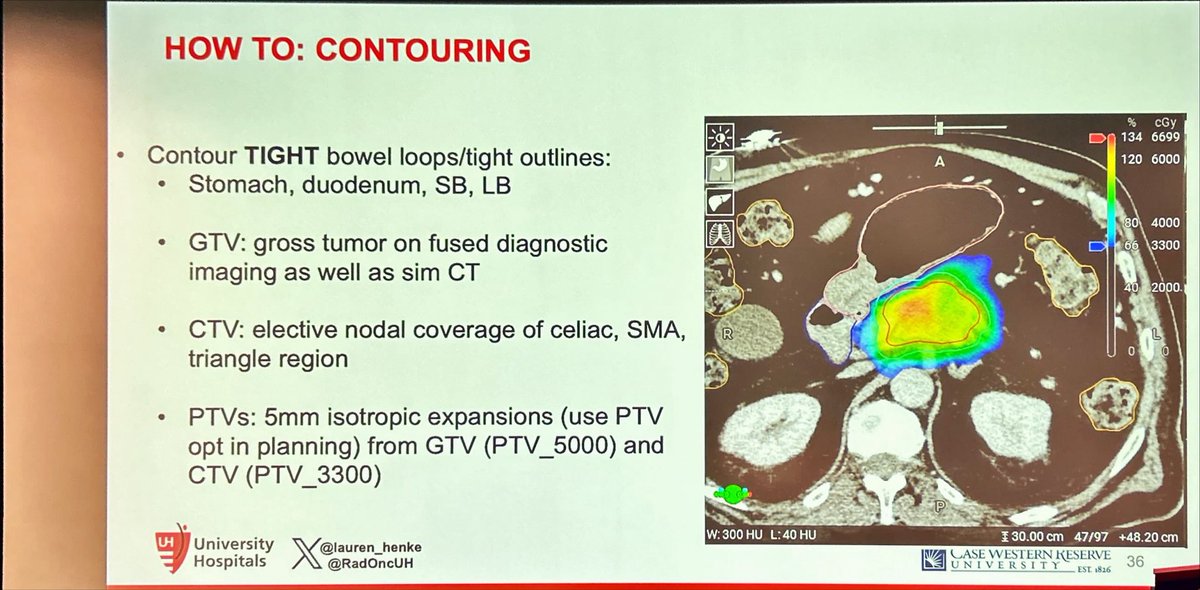
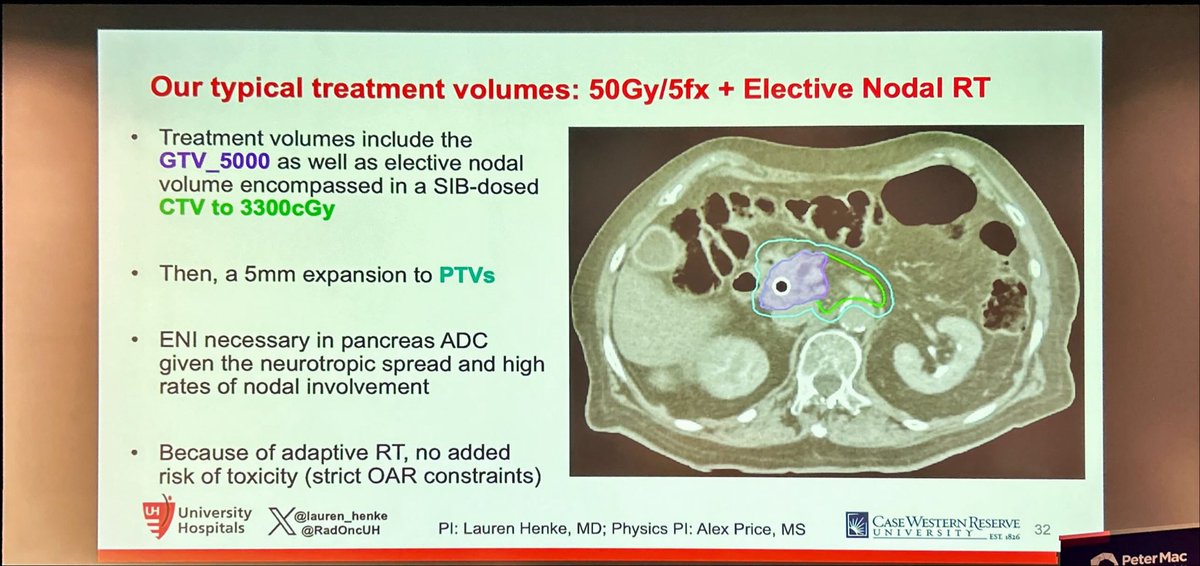
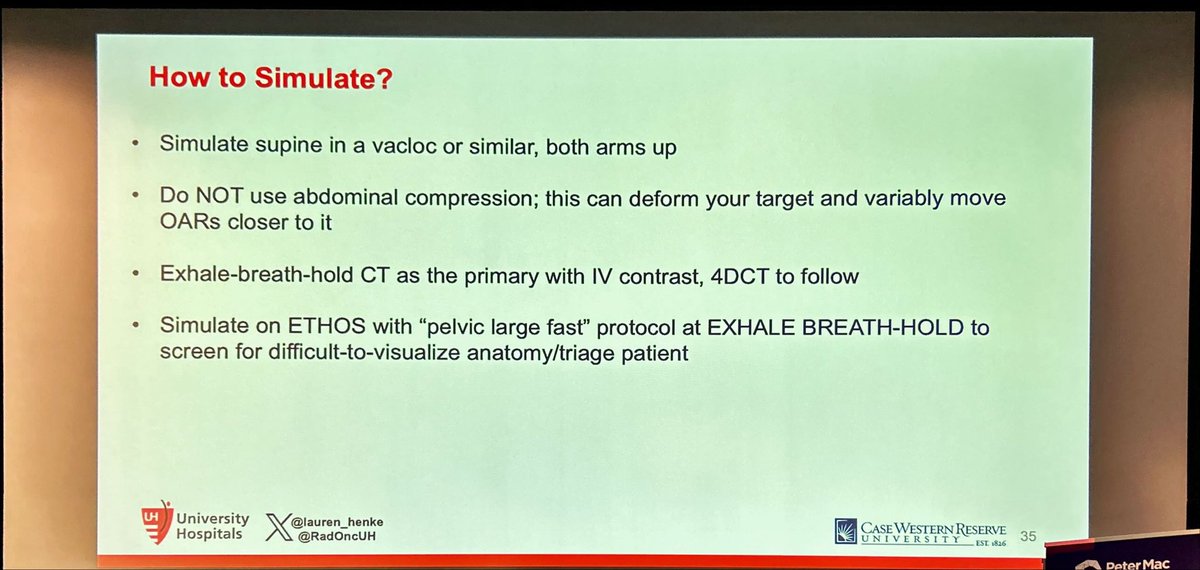
Practical step by step guidance on how to perform pancreatic #SBRT by @lauren_henke at #SABR2025#SBRT is the best way to deliver BED>100Gy to this tumors, which likely drives superior survival in #PancreaticCancer
Among patients with advanced urothelial cancer, upfront enfortumab vedotin dose reduction was linked to a 50% reduction in treatment interruption risk but did not compromise overall survival. https://t.co/0vqWHuJ9tm
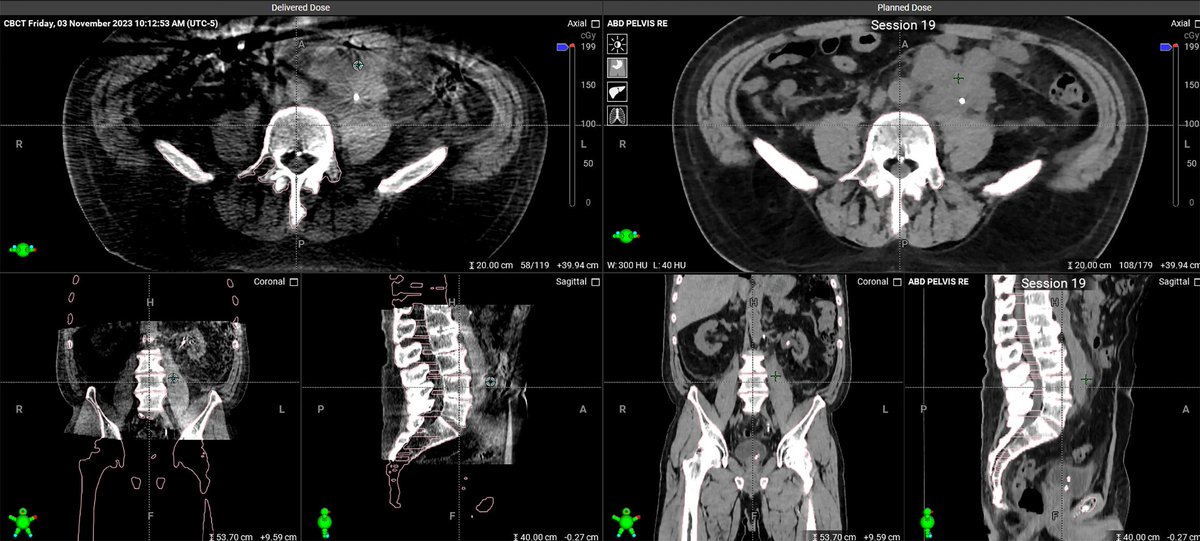
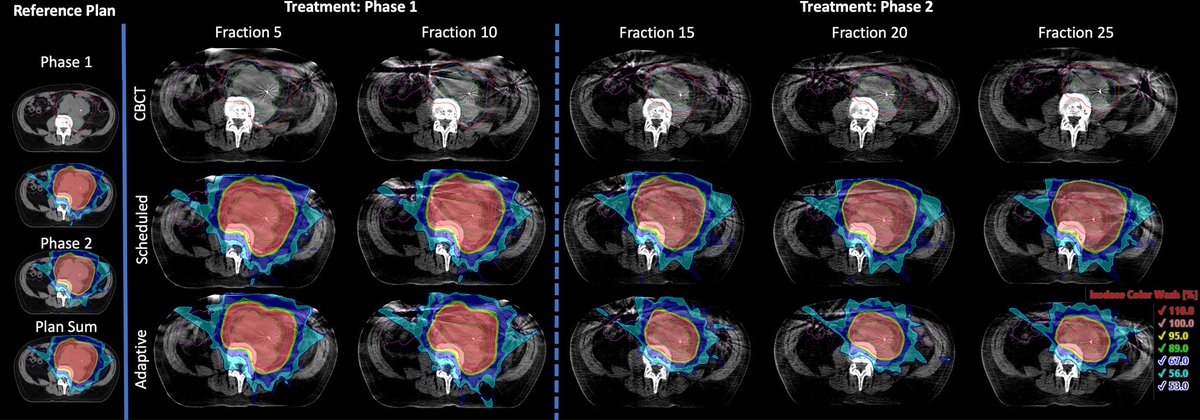
The Use of Adaptive Radiation in a Retroperitoneal Seminoma Patient with Poor Candidacy for Chemotherapy: A Teaching Case
🔗 https://t.co/wdm9wI1s2p
#radonc#radonced#menshealth#movember



































![DrRishabhOnco's tweet photo. 🎯 HARMONi-6 delivers new hope in 1L advanced squamous #NSCLC 🫁
📍 Phase III | n=532 | 1L Stage IIIB–IV sqNSCLC
💊 Arms:
🔹 Ivonescimab + chemo (20 mg/kg Q3W)
🔹 Tislelizumab + chemo (200 mg Q3W)
→ Followed by monotherapy maintenance
📈 Results:
• PFS: 11.1 mo vs 6.9 mo (HR 0.60 [0.46–0.78], p<0.0001)
• PD-L1 < 1%: 9.9 vs 5.7 mo (HR 0.55)
• PD-L1 ≥ 1%: 12.6 vs 8.6 mo (HR 0.66)
✅ Consistent benefit across subgroups
⚕️ Safety:
• SAE 32.3 % vs 30.2 %
• Grade ≥3 hemorrhagic events 1.9 % vs 0.8 %
🧩 Takeaway:
Ivonescimab-chemo shows superior PFS vs tislelizumab-chemo - emerging as a potential new 1L standard for advanced sqNSCLC.
#OncoTwitter #MedTwitter #LungCancer #Immunotherapy #ESMO25 @OncoAlert @myesmo @esmo_open](https://pbs.twimg.com/media/G3lQhZEW0AALc5A.jpg)




















