Proud to help promote our @MidAmericaHeart / UMKC T32 Postdoctoral Fellowship Training Program in Cardiovascular Outcomes Research.
This NHLBI-funded program has been a major engine for developing the next generation of cardiovascular outcomes researchers. Fellows receive deep mentorship, hands-on analytic and clinical research experience, access to major registries and trial datasets, and opportunities to develop expertise in quality of care, implementation science, health status measurement, health economics, and cardiovascular clinical research.
The program is a 2-year postdoctoral fellowship, with an option for a combined pathway with clinical cardiovascular fellowship training. Fellows may also pursue an MS in Bioinformatics with emphasis in Clinical Research and a Certificate in Biomedical Technology Entrepreneurship.
Our trainees have built an exceptional record of national presentations, peer-reviewed publications, and early-career awards.
Please share with outstanding applicants interested in using research to improve the quality, value, and outcomes of cardiovascular care.
Contact Danielle Olds, PhD, MPH, RN at
[email protected] for more information.
Rare gem in @JAMA_current: a comprehensive review on Cardiac Resynchronization Therapy covering biventricular pacing and the rising role of conduction system pacing. Excellent synthesis of the evidence for HF patients with dyssynchrony.
Huge congratulations to @mihailchelu, @CaiqueTernesMD, @KennethEllenbo1 and coauthors!
https://t.co/VKUU1Apsjc
@NEJM@MKIttlesonMD I appreciate the journal for highlighting the moral challenge. Human formation - the development of virtues such as prudence and charity - is completed by adolescence. Medical education can refine these qualities, but it is not positioned to instill them for the first time.
https://t.co/rhes3jriyH
As we celebrate another anniversary of Favaloro’s remarkable accomplishment, let’s not forget who performed the first CABG in February of 1964.
Kolesov was a medical pioneer and a war hero.
@angioplastyorg@Tesslagra@paulsaundersMD@georgetolisjr My teacher Irina Ganelina might have been the “Mother” of a coronary care unit. In any case, she and Kolesov (LIMA to LAD bypass) worked in Leningrad after WWII. When I was in med school there in 1980s, I was told they were the “first”. Evidently, Cardiology has many parents.
It was a privilege to welcome Dr. Clyde Yancy to Kansas City for a city-wide discussion on contemporary medical therapy for heart failure and the evolving challenge of sudden cardiac death risk.
Few leaders have had as much influence across the modern eras of heart failure care as Clyde. The field has moved from an era largely defined by neurohormonal blockade and device-based prevention to one now shaped by rapid implementation of comprehensive, multi-drug GDMT. Across that arc, trials such as MADIT-II, SCD-HeFT, and DANISH helped define our thinking around sudden cardiac death prevention, while event rates have continued to shift as patient cohorts, background therapies, and competing risks have evolved.
That history made the discussion timely. As therapies improve, the question is no longer simply whether we have effective treatments. It is whether we can reliably deliver them, optimize them, and still recognize where residual risk remains.
Clyde and I have had the opportunity to work together on IMPLEMENT-HF, focused on improving defect-free heart failure therapy at discharge and 30 days after hospitalization. I was fortunate to lead the manuscript published in 2025, with Clyde as senior author, and the work reflects a core principle we both believe in: hospitalization is not just a marker of risk, but an opportunity to change the trajectory of care.
We also took a deeper dive into the SCD PROTECT study. Even in a contemporary cohort with high adherence to four-drug GDMT, event rates while patients were using a wearable cardioverter-defibrillator remained meaningfully elevated. That finding reinforces an important message: modern GDMT has transformed heart failure care, but residual arrhythmic risk persists, particularly during vulnerable transitions and early treatment windows.
On a personal level, this evening felt full circle. Clyde has been a mentor to me since 2010, when he came to Northwestern during my first year of fellowship. I was part of his first full graduating class of fellows under his leadership at Northwestern. I later left Chicago, where he was my Division Chair, to come to Kansas City and help build programs aimed at raising the bar for heart failure and cardiometabolic care across our region.
That is what made this event so meaningful. It was a true city-wide conversation, with representation from most health systems in Kansas City, including Saint Luke’s / BJC, the University of Kansas, HCA hospitals, including Centerpoint and Research, North Kansas City Hospital, and others across the region. I was especially proud to have Dr. Zubair Shah from the University of Kansas join the panel, a colleague and mentee since I first came to Kansas City in 2015.
Heart failure care advances when science, implementation, and community collaboration come together. Having Clyde with us in Kansas City was a reminder of how far the field has come, how much work remains, and how powerful mentorship can be when it comes full circle.
Most cardiologists obsess over salt restriction.
But the real driver of heart disease in most of my patients? Insulin resistance from carbs and sugar. It’s too cheap and easy to make bad food choices.
Cut those first and blood pressure, inflammation, and plaque risk drop faster than any pill alone.
Angiography-Derived Fractional Flow Reserve During Percutaneous Coronary Intervention. Comparable clinical outcomes compared with pressure-wire assessment through 2-years. LBCT @CRT_meeting#CRT2026 & published simultaneously @wfearonmd@EricSecemskyMD https://t.co/1krGxEgVYP
As the 1st #EAPCI Summit comes to a close, I thought it would be interesting to look back at a time when an infarct was considered a contraindication for PCI. Cue Geoff Hartzler, who explained to me how he changed that. #AngioHistory
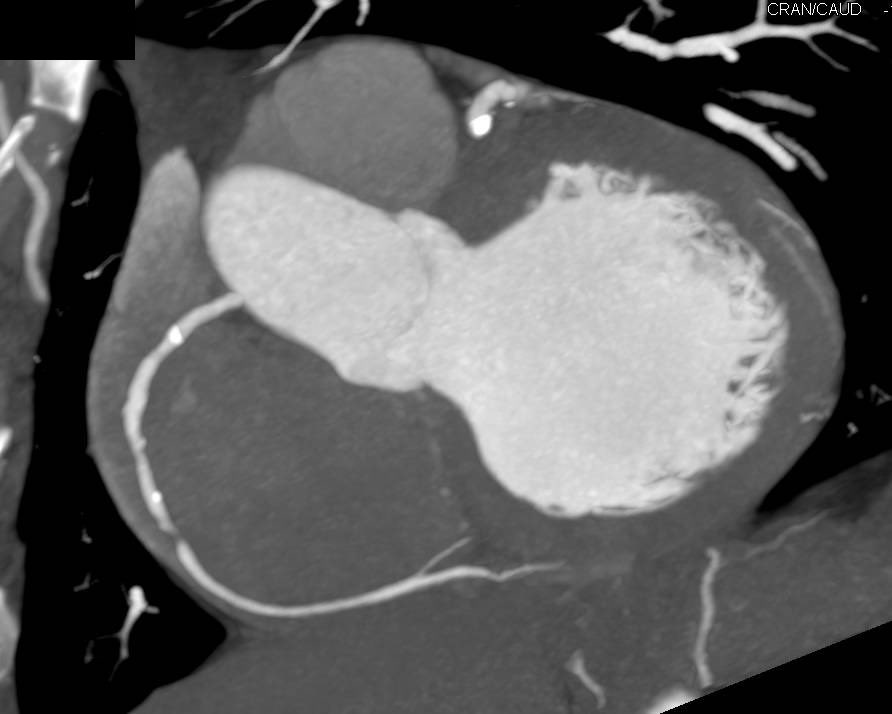
Thanks to JACC Case Reports for publishing our paper on Real-Time IVUS Guided (RTIG) Ostial Stenting: A Step-by-Step Guide.
5 years of work from benchtop models, microCTs to a now standard part of our practice. Hope someone finds it helpful!
https://t.co/1C1krUklzp