Let's talk RA-BRIDGE/RA-BRANCH (the 'new ORAL Surveillance'):
baricitinib vs TNFi RCTs in RA + 1 VTE RF
Big news was secondary endpoints:
MACE (HR 1.06), malignancy (HR 1.27), not sig
The key: how similar is study population to ORAL Surveillance? 1/4
LB0009 #EULAR2026@RheumNow
#JCLSpotlight: Baseline apoB may drive long-term MACE recurrence in very young ACS survivors, highlighting its potential utility for risk stratification beyond traditional lipid markers.
🔗 https://t.co/mIMLJ4OX2C
@NutritionMadeS3@EliasBjornson Comparative imaging data are limited. Many unknowns. Here's a PCSK9i study. If you assume olezarsen effect is 50% greater at 18 months vs 12, median % lowering from baseline ~80% of that with PCSK9i on non-calcified plaque, 62% of PCSK9i on LAPV. https://t.co/VSxuxaoHuo
More interesting context for ESSENCE imaging study. Also in this study, LAPV change with evolocumab -45% at 18 months. ESSENCE: placebo +2.78%, olezarsen -16.62% at 12 months /1 https://t.co/U0YciAjmRD
• using apple-apples supplement comparison (with similar #'s on statin), incremental cost/qaly 70% lower than new AHA threshold, i.e. highly cost effective
• uses uber conservative assumptions that understate benefit. /3-fin https://t.co/8blGWOkZrd
New lipid guidelines are a good step forward from the last ones. In my view, apoB adds value beyond traditional measures, including non-HDL-C and newer LDL equations. Even with newer equations, (by some definitions) over half of Americans have apoB-LDL-C discordance. /1 🧵
When measures disagree, cardiovascular risk tracks with apoB. Systemic review from last year. 👇
To my eyes, recent JAMA cost effectiveness study impressive.
/2 https://t.co/MrBAg9UA8i
LDL lowering in primary prevention. Bigger impact than we thought?
Drs. Kevin Maki, @DineshKalra, and Alan Brown show ~30% MACE reduction per ~39 mg/dL LDL drop even in lower-risk patients.
Is it time to treat earlier?
🎥 Watch on #Vumedi - https://t.co/gE1suyAHHD
#LDL#ASCVD #Prevention #Lipidology #VumediCardio @nationallipid
@TriglycerideF@UCPH_Research Interesting study. After PROMINENT, one probably needs more than this observational study, despite propensity score matching, to support fenofibrate use with statins in those with non-HDL-C>140mg/dL.
The recording from today's Baim Grand Rounds with @ProfKausikRay titled, "Changing the Paradigm of ASCVD Prevention" is now available on the Baim website. You can find it here: https://t.co/npsuK6R7L7
@sanekachakrava1 Thanks for comment. On concern 2: The HOPE-3 trial likely included many with PCE 10y risk 5-7.5% and many of those would also have PREVENT 10y risk 3-5%. https://t.co/nOtQzDTiCV On point 1, there's uncertainty with non-randomized data. At lower doses, risk seems modest.
@Hragy@ACCinTouch@escardio@Drlipid 1. As @DrMarthaGulati notes, Rx recommended based on LDL>=190, also 30y risk>10%. 2. There is an issue that traditional risk calculators don't reflect causal drivers of disease (lipids/ blood pressure) to the extent seen in short term RCTs or long term genetic studies.
@drpablocorral Agree with the sentiment. But science takes time. There are hints of benefit from inflammation targeting. I'm hopeful one of the inflammation based strategies will pan out and become a useful treatment adjunct. https://t.co/MNz5bEakXQ
Somewhat lukewarm view of colchicine in this editorial. "the CLEAR SYNERGY results have brought considerable clinical equipoise for the prescription of colchicine to reduce ASCVD risk"
https://t.co/aUBwtKBCF6
https://t.co/s4PAwArQ5c
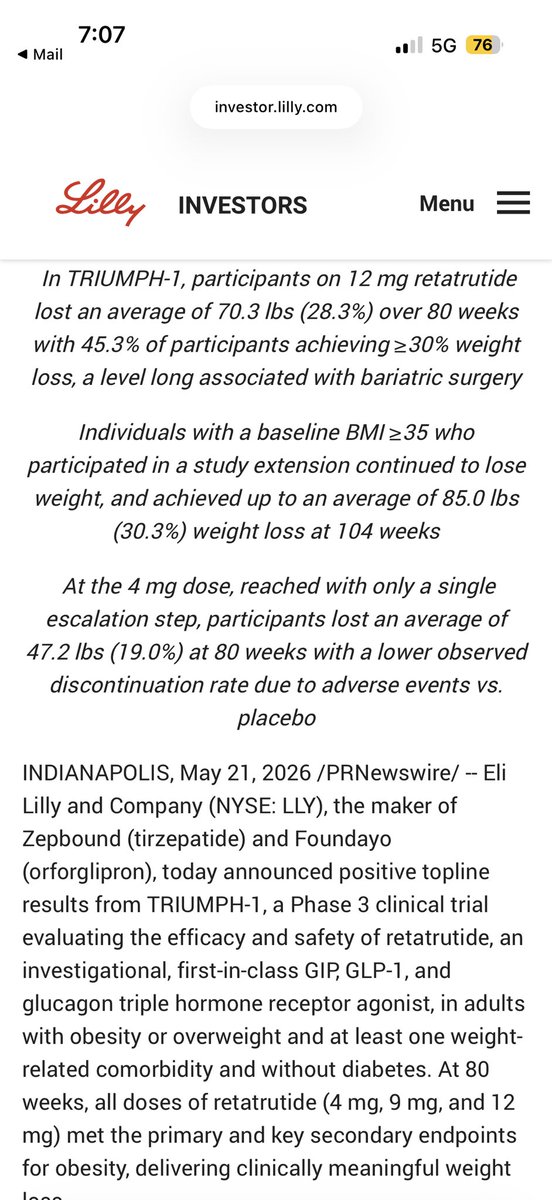
ACHIEVE-4 with Orforglipron H2H vs. Insulin glargine #T2D 2,700 people, 2 years, Cardiovascular safety, reduced risk of all cause mortality and no evidence of liver injury https://t.co/eBdD05btfD