🔬 Critical Evaluation of TNT in LARC
🔗 https://t.co/sLoLUmvHYZ
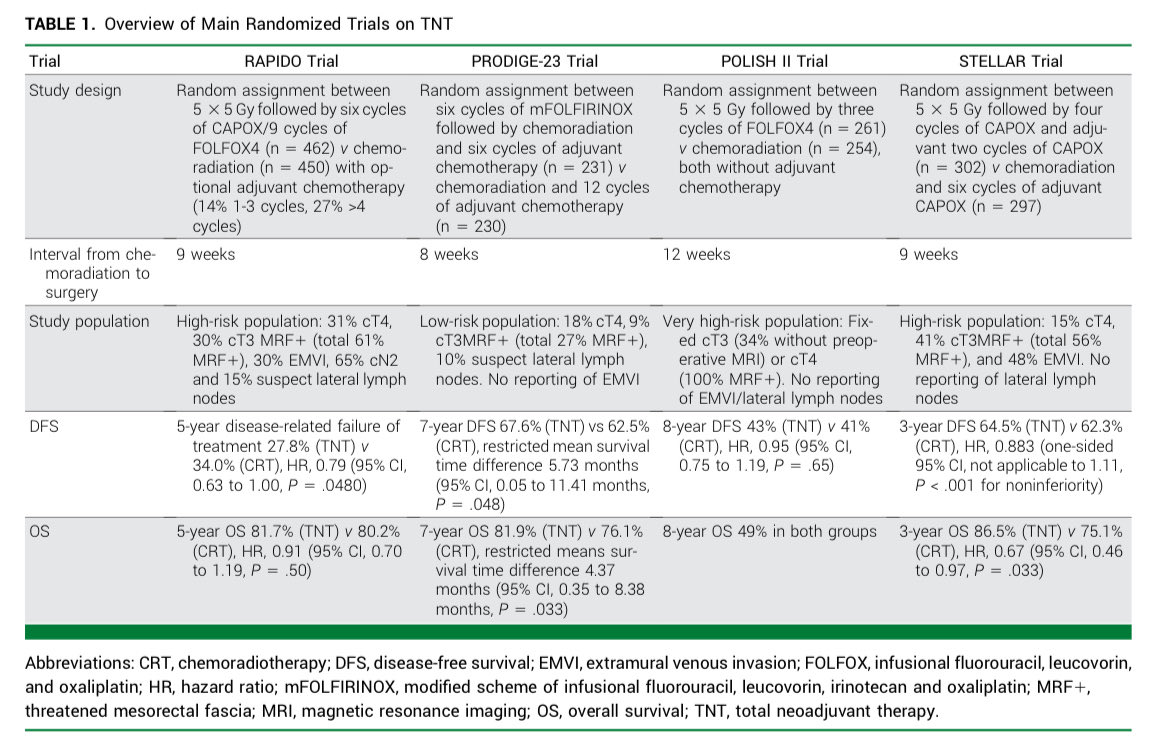
🧬 Review of RAPIDO, PRODIGE-23, POLISH II & STELLAR
💊 Small DFS gain · OS benefit uncertain · Added toxicity
📊 CRT remains standard; biomarkers needed for selection
#DraMartinezLago#GItumors
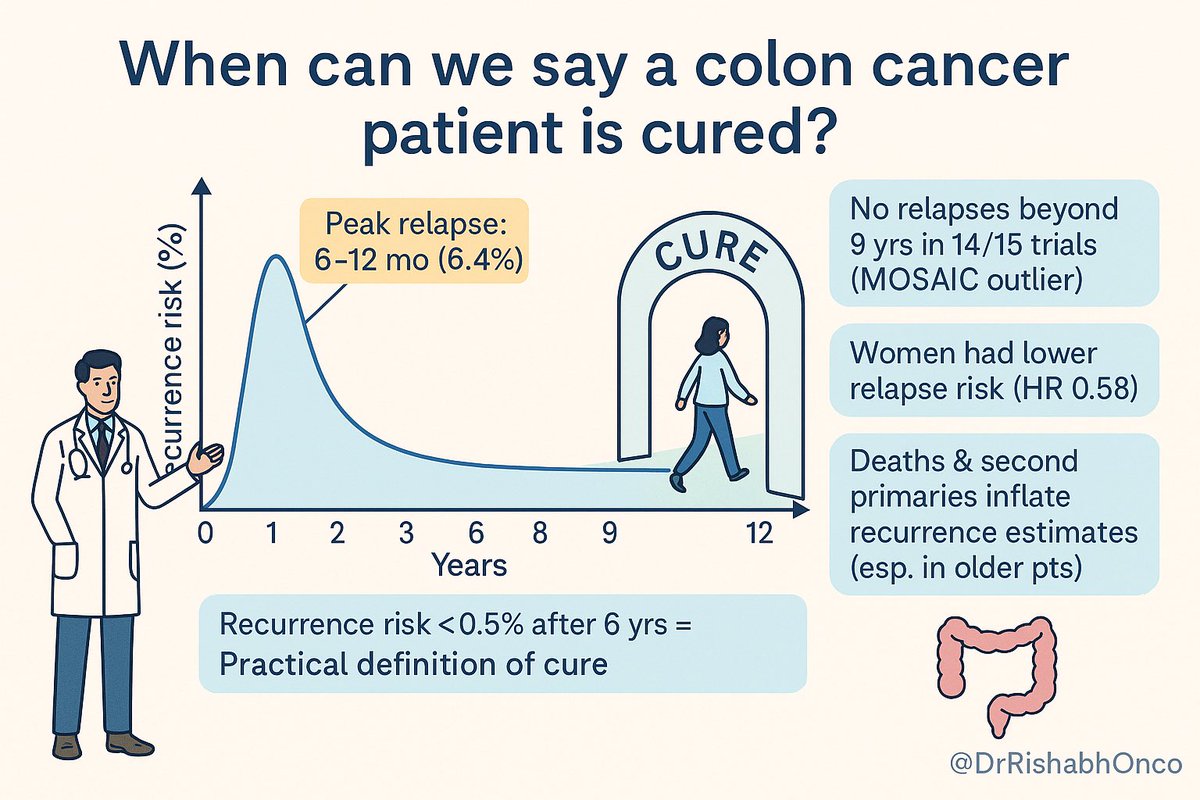
🚨 When can we say a colon cancer patient is “cured”?
🔎 Pooled analysis of 15 phase III RCTs (n=35,213; stage II–III CC, adjuvant chemo):
📉 Recurrence risk peaks at 6–12 mo (6.4%)
⏳ Falls steadily → drops <0.5% by year 6
🛑 After 6 yrs relapse-free → practical definition of cure
👩 Women had lower relapse risk (HR 0.58 vs men)
🏁 Most trials showed no relapse beyond 9 yrs (MOSAIC outlier)
💡 Takeaway: Colon cancer cure can be reasonably declared if no relapse at 6 yrs post-surgery + adjuvant therapy → may reduce unnecessary long-term surveillance.
📖 Pastorino et al. JAMA Oncol. 2025.
🔗 https://t.co/rgXJQOo5ZT
#OncoTwitter #ColorectalCancer #Survivorship
@OncoAlert@myesmo@asco@JAMAOnc
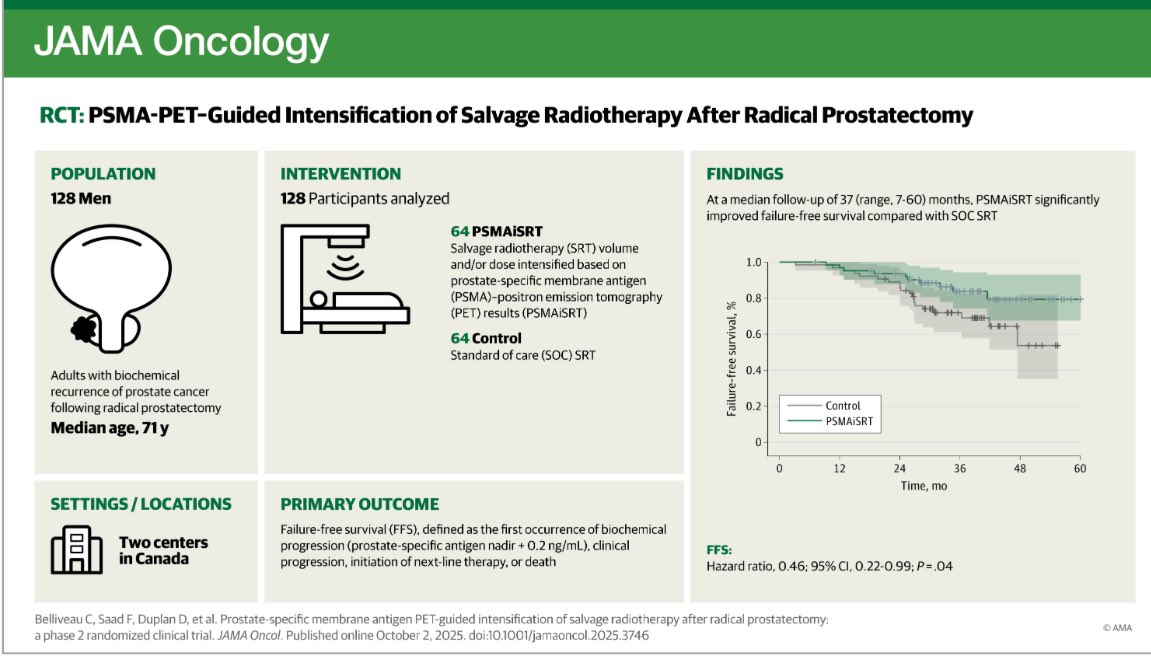
⚖️ TNT in Rectal Cancer: Promise or Premature?
💊 Total Neoadjuvant Therapy (TNT) has been hyped for LARC, but does it really beat standard chemoradiation (CRT)?
👥 4 Key RCTs:
•RAPIDO → ↓ distant mets, ❌ no OS gain
•PRODIGE-23 → ↑ DFS, small OS edge (but early curve drop & underpowered)
•POLISH II → initial OS benefit → vanished at 8 yrs
•STELLAR → ↑ 3-yr OS (86.5% vs 75.1%), but short f/u
📊 pCR rates: higher with TNT (22.5% vs 13.3%) but confounded by shorter CRT–surgery interval.
🚨 Takeaway: TNT = modest ↓ distant mets, unclear OS benefit, more toxicity. CRT remains standard until better biomarkers guide who truly benefits.
📖Ubink et al. JCO Oncol Pract. 2025.
DOI: https://t.co/OQSE3RPRPj
#OncoTwitter #ColorectalCancer #RadiationOncology #Oncology
@OncoAlert@esmo_open@myESMO@ASCO @JCOOPjournal
I think we need to reserve judgement and final analysis until seeing all of the papers from these trials….
… but are these results really so different?
- In the US trial, more IMRT patients (40% vs. 27% = 13% difference) received g-tubes.
- In the UK trial, more IMRT patients (58% vs. 45% = 13% difference) received g-tubes (with less weight loss).
- Tube placement is a very patient and MD-specific decision; nearly impossible to interpret whether it was beam or dream (that protons will protect against high-grade dysphagia).
- In the US trial, 3% of IMRT and 0% IMPT patients were tube-dependent at 1 year; no difference.
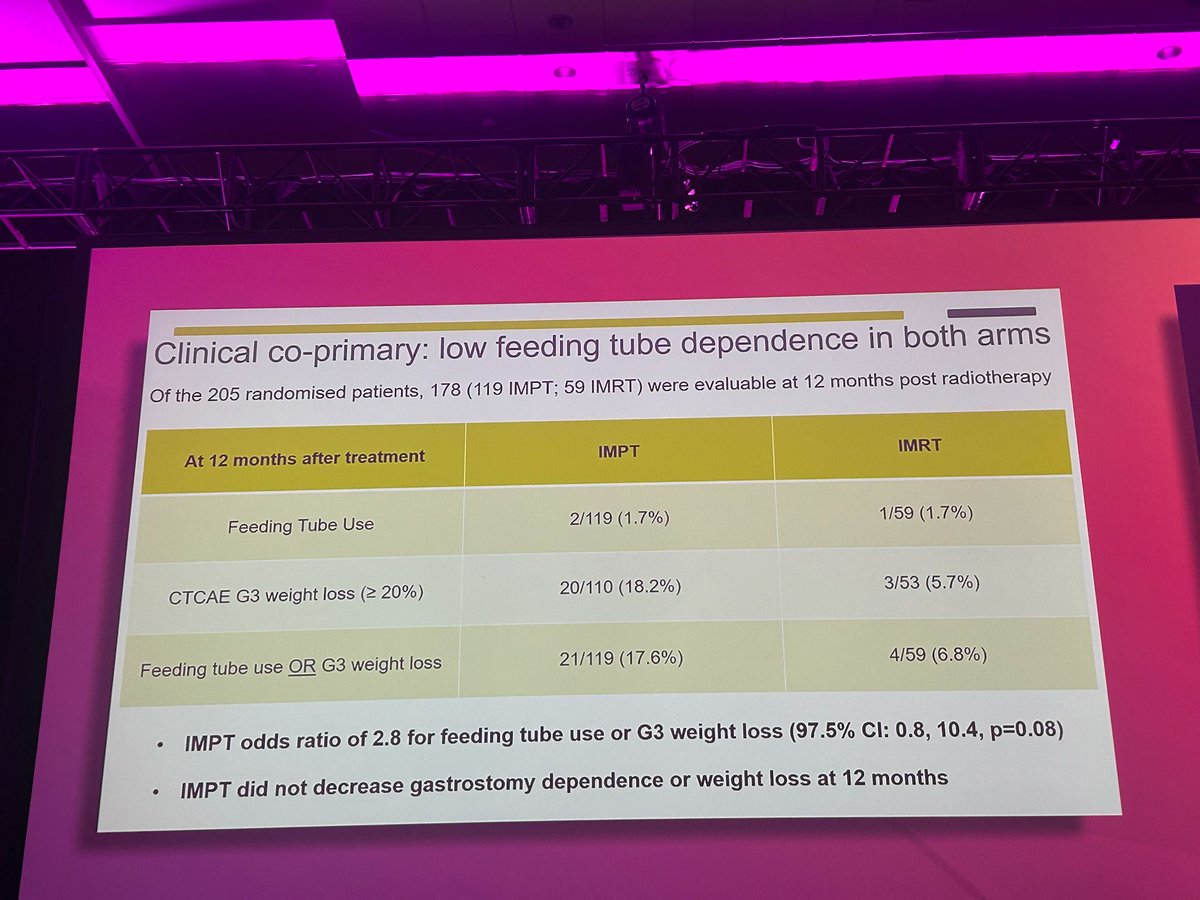
- In the UK trial, 1.7% of IMRT and IMPT patients were tube-dependent at 1 year; no difference.
- There were no differences in mucositis, dermatitis, or pain between IMRT and IMPT in the US trial. There was more weight loss in the UK but not US IMPT arm.
- Any differences in PRO's in the UK trial were very modest and transient.
- We do not know the PRO results from the US trial: can’t wait to see those those data, but they will be confounded due to crossover.
- There were no statistical differences in disease control between the arms in either study.
- One interesting note from TORPEDO: there were 9 LRF events in IMPT and only 2 LRF in IMRT, more skewed than expected. It is far too early to see a survival difference in the UK trial.
The results are far less conflicting than the messages, which are diametrically opposed.
If the US trial didn’t show an inexplicable OS difference (and hard to further comment until we see the final paper; much more discussion needed when that is published), we would have two trials that showed a bit more acute dysphagia with IMRT but no obvious long-term differences, supporting IMRT as the established, high-value standard.
TORPEDO was an extremely clean, elegant study that that shows superb long-term outcomes with both modalities. I see no reason to deviate from IMRT as the standard-of-care. Whether insurance companies want to cover IMPT at the same or increased rates is up to them, but this study makes it extremely hard to justify.
Perhaps the most important message is that we CANNOT REST. Patients did very well, but radiotherapy can still do much better in the short- and long-term. Novel paradigms for BOTH volume and dose reduction are under active investigation and are far more likely to improve patient outcomes than particles.
@rweichselbaum@DrSpratticus@CJTsaiMDPhD
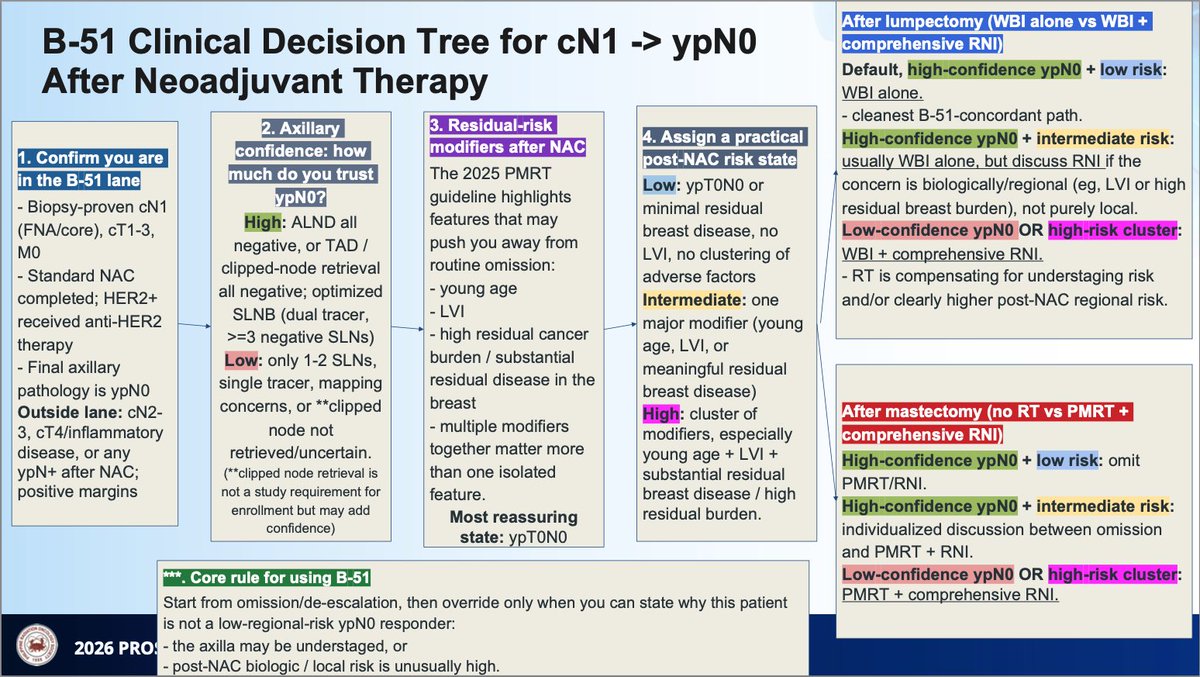
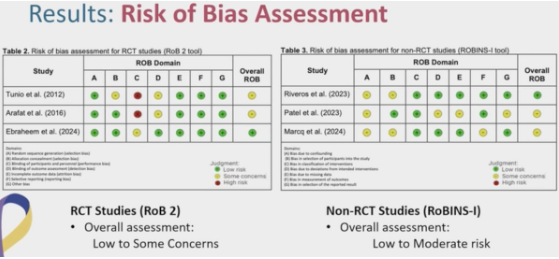
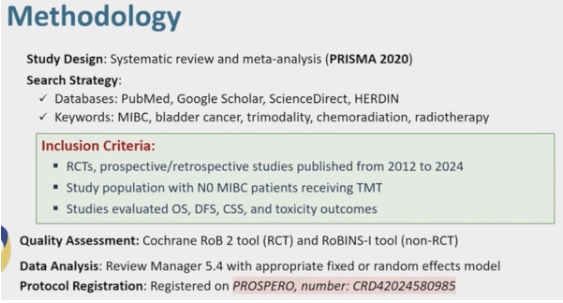
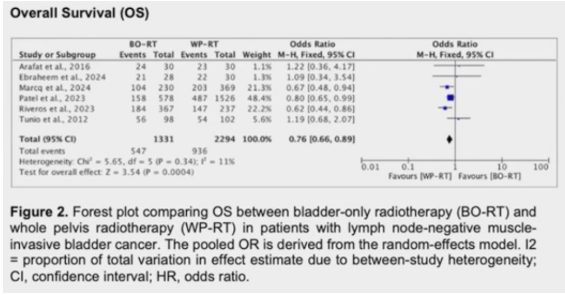
Bladder only vs. whole pelvis radiotherapy in trimodality treatment for lymph node negative urothelial muscle-invasive #BladderCancer: a systematic review and meta-analysis. Presented by Alyssa Anne Granda, MD @jrrmmcOfficial. #ASTRO25 written coverage by @RKSayyid@UAUrology > https://t.co/UQ1mA42DdG @ASTRO_org
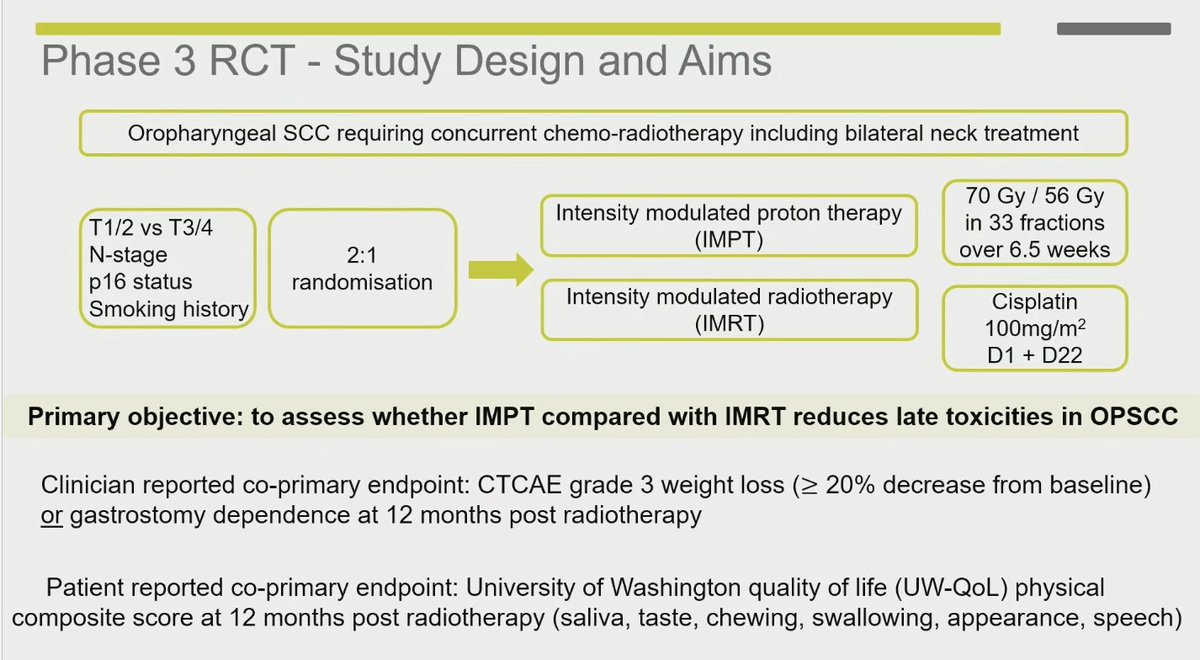
📢 Phase III RCT in locally advanced #OPSCC: proton 💠 vs conventional #radiotherapy 🔆
❌ No diff. in 12-mo gastrostomy rate, QOL, or swallowing.
⚖️ Similar 2-yr local control & OS (~95%).
👉 High-quality IMRT remains standard; IMPT not required.
#ASTRO25#RadOnc@ASTRO_org
🚨TOROEDO trial - superbly executed with uniform RT plan QA/no crossover.
No difference in either endpoints.
What’s next? Refine the strategy. Technology is a means to an end. Reduce volume and dose (gross/elective) with biology based therapy selection.
@ASTRO_org#astro25
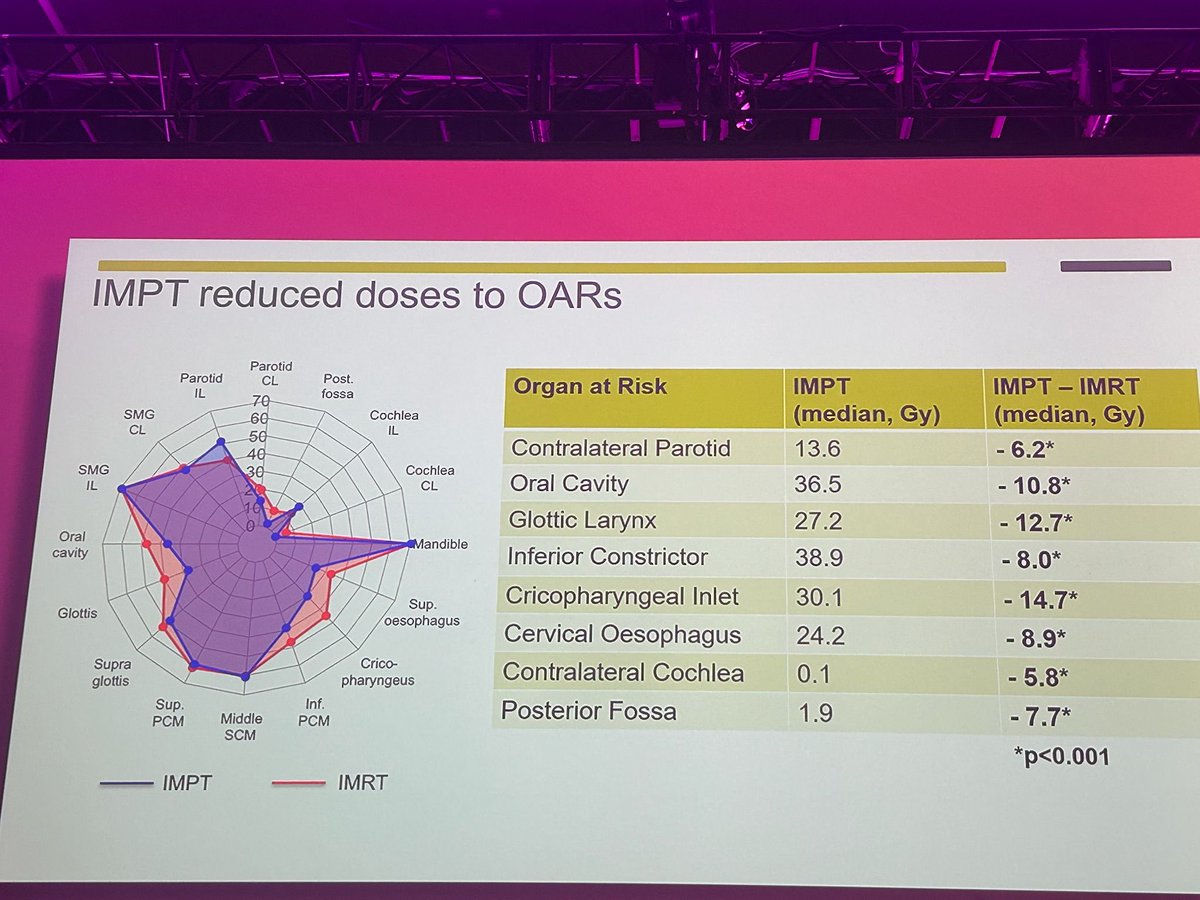
Photon vs proton . Despite less OAR doses more side effects with proton . Is it because of other uncertainties @DavidSherMD @AndrewKellerMD #astro2025
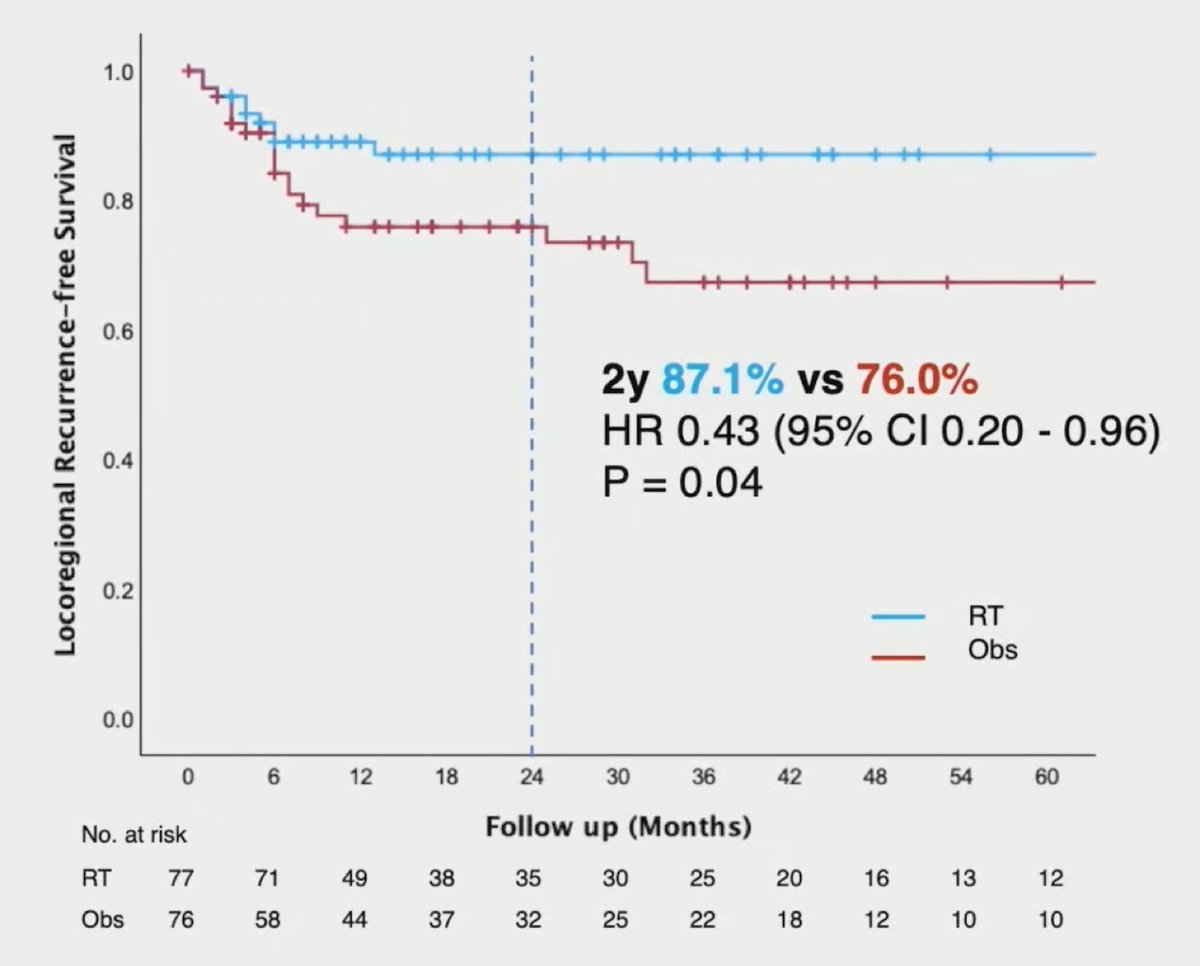
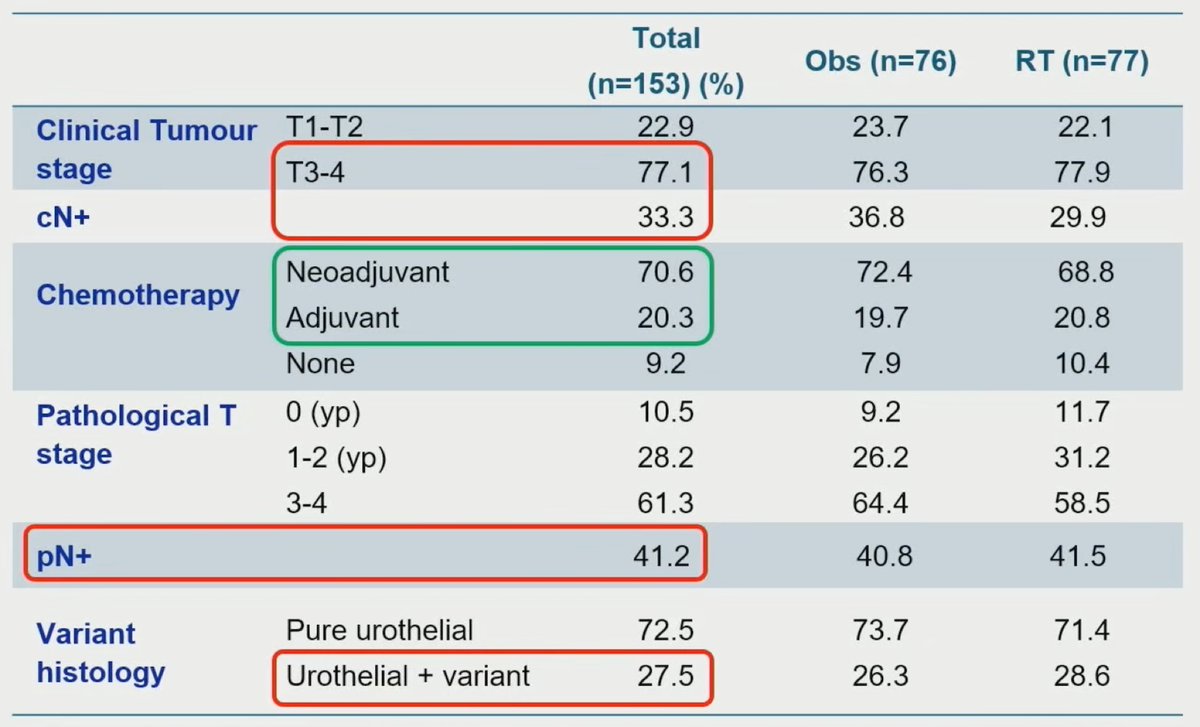
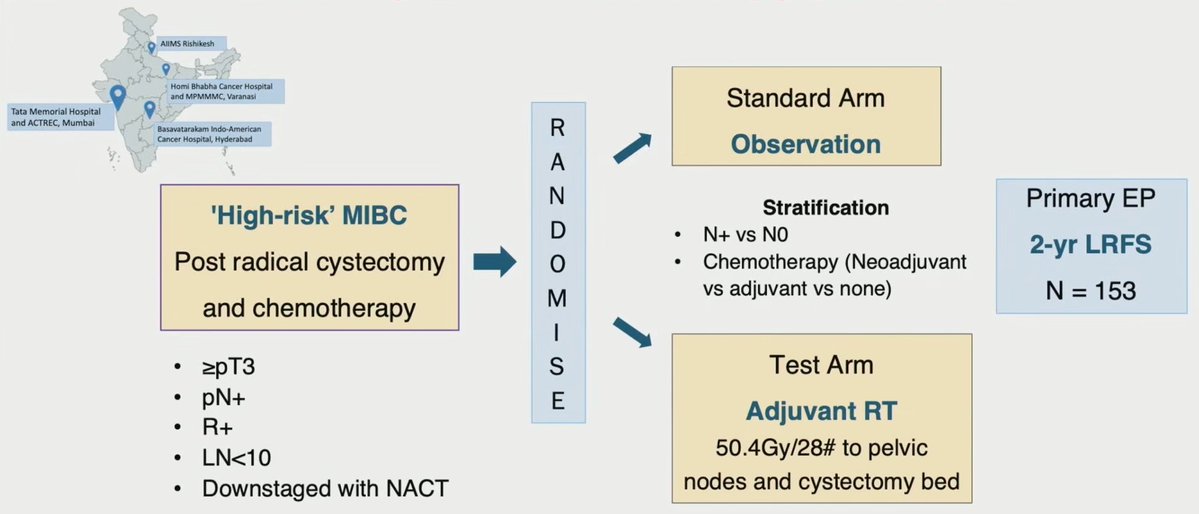
💥Phase III BART trial (n=153) in locally advanced #BladderCancer after cystectomy + chemo:
🔹 RT (n=77) vs Obs (n=76)
🔹2-yr locoregional recurrence: 8% RT vs 26% Obs (p=0.006)
🔹OS trend ↑RT (68% vs 57%), not sig
🔹No ↑ severe late adverse events
👉Adjuvant RT ↑ control & DFS, esp T3/4 & N+ pts. #ASTRO25 #RadOnc