GI Oncology standard regimen doses remain too high for many real world patients. Retrospective and prospective trials demonstrating benefit of reduced doses or dose escalation are accumulating. #meded#gionc#crcsm#pancsm
Clear that interactive in person chalk talks and case based discussions in modern hem onc education are the way to go. Didactic lecture still has a role, but remains overemphasized.
📚 Medical education for trainees and fellows is a critical part of oncology training.
At @SylvesterCancer , we developed a novel Oncology Bootcamp curriculum featuring foundational "101" topics, interactive case-based discussions, and chalk talks. @HemOncMiami@AksheeBatra@Drjhoffmanmiami@DrPlatelet@Alsbihi93
The program led to significant improvements in knowledge, retention, and learner engagement.
Most importantly, this is a practical and scalable model that can be replicated across institutions and state oncology societies to strengthen oncology education nationwide. @jrgralow@ASCO@ASCOTECAG@FLASCO_ORG@GlopesMd@RManochakian
#MedEd #Oncology #HematologyOncology #MedicalEducation #ASCO26
I give the hallmarks of cancer lecture @nyulisom@Perlmutter_CC. KRAS: potential target ➡️ G12C ➡️ now complete revision of my slides! Going to be going on about this for a while to the first year medical students who do not realize how amazing this is yet. 🎉😎🎉
As many other oncologists will also attest, we were taught this was a dead end
It was, dogmatically, never going to work — kras was too much of a “greasy ball” to be targeted
And yet here we are, with truly meaningful survival curves👇
Inspiration on multiple levels #ASCO26
Thrilled and honored on behalf of the whole team, patients, scientific community and more- congratulations and good luck to @BrianWolpin this afternoon @MSKCancerCenter@DanaFarber@RevMedicines - next step is translate to practice!
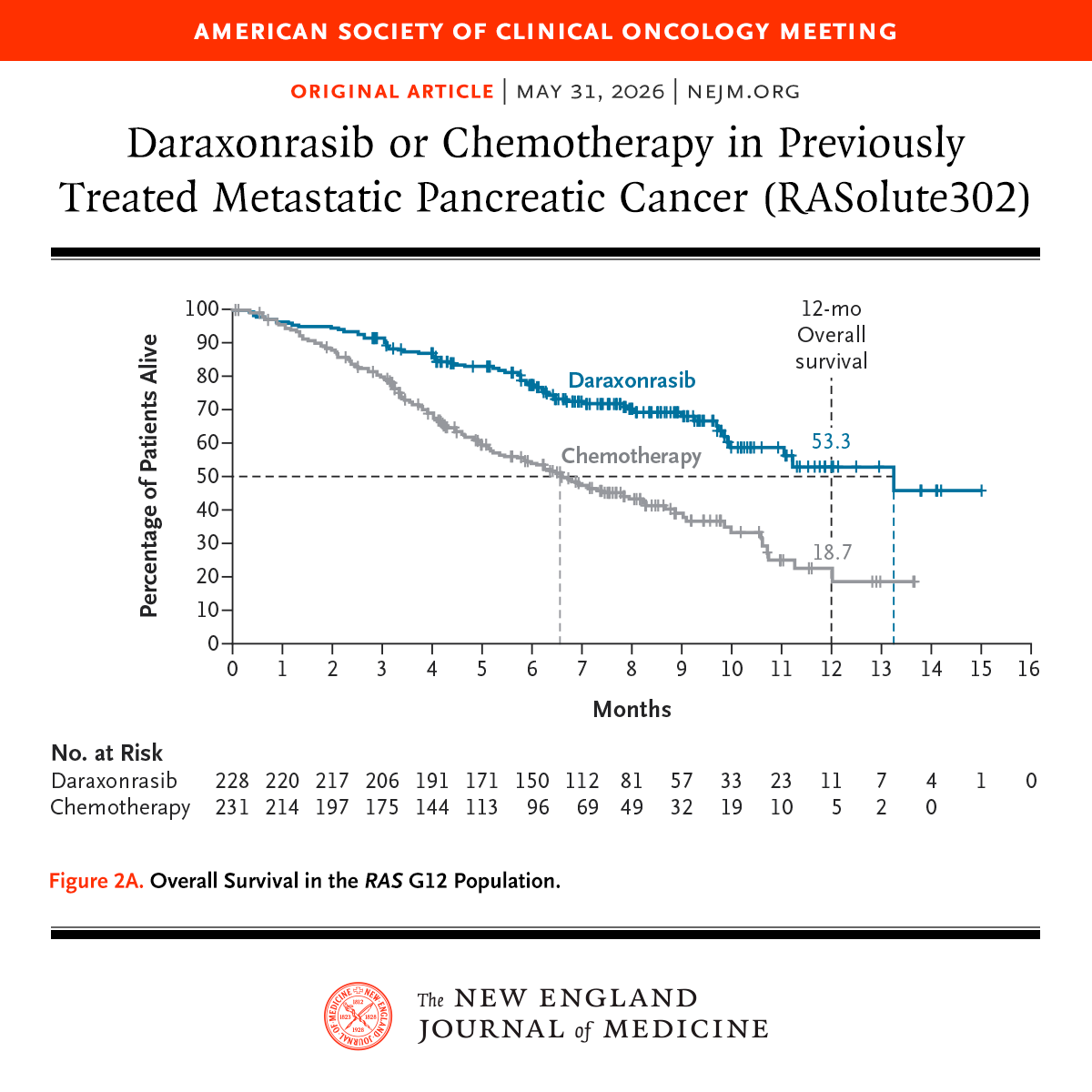
🚨 The highly anticipated data from RASolute 302 have arrived—and the results are turning heads at #ASCO26.
#Daraxonrasib met all primary and key secondary efficacy end points in previously treated PDAC, marking a major milestone for KRAS-targeted therapy in a disease with few effective options.
Our coverage includes key perspectives from Brian Wolpin, MD, MPH, and @rachnatshroff on the practice-changing implications of these results!🔬
Read more 📰: https://t.co/Wjogm5VXbc
@ASCO #pancsm #oncology
#ASCO26 Benefit for daraxonrasib as expected primarily for G12D/V mutations. Not clear based on based on supplemental if benefit other RAS mutations. Still a major breakthrough and amazing to have contributed to study! Congrats @md_oberstein@Perlmutter_CC co-author on paper!
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
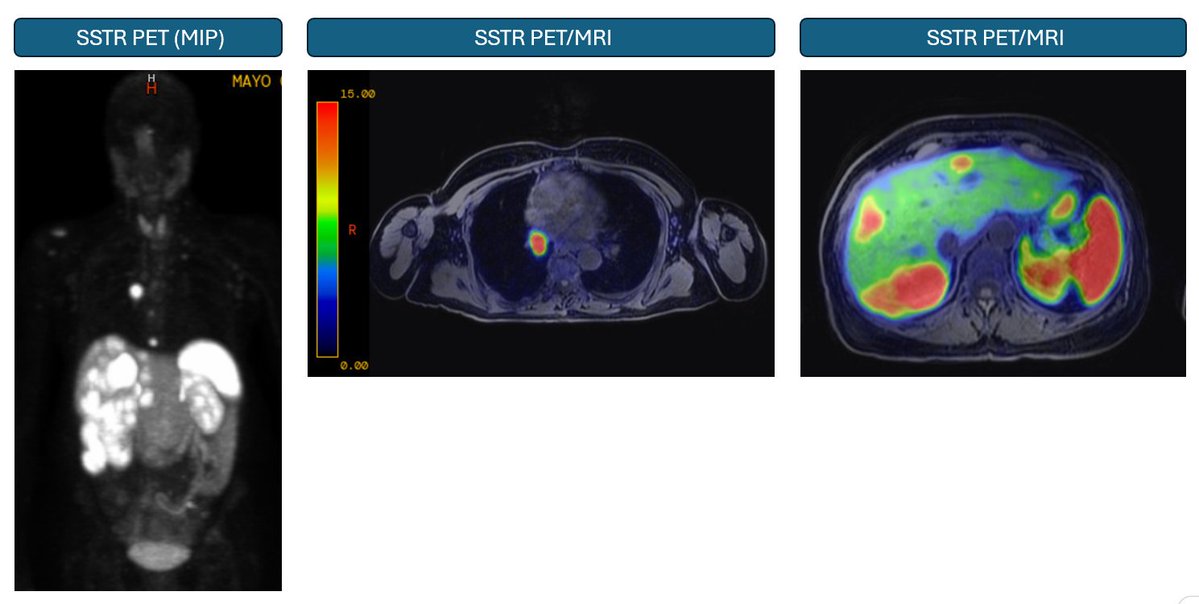
Images from the NET clinic...
Working in the NET clinic is often humbling... Tumors do not read textbooks and sometimes, things just do not make sense but yet are happening right in front of you. As I often say, every patient with NET is unique (of course, every patient with cancer regardless of cancer type is unique...) with their own clinical presentation.
This patient below has metastatic lung NET, indolent, producing very large amounts of serotonin but with no diarrhea or flushing (serotonin does not cause flushing by the way but does cause diarrhea) so essentially asymptomatic in terms of typical carcinoid syndrome. This patient however has carcinoid heart disease with severe tricuspid and pulmonary valve regurgitation. Interestingly, there is no lower extremity edema but there is pulsatile hepatomegaly (a classic finding), both systolic and diastolic murmur, elevated JVP but not a trace of lower extremity edema.
Below you can see evidence of hepatic venous congestion in the venous phase of the CT with what sometimes is called nutmeg liver. That lobular pattern is not seen on the arterial phase or on the recent gadoxetate enhanced delayed MRI imaging.
I just thought I should share that carcinoid syndrome can present in very atypical ways without the cardinal symptoms of diarrhea and flushing. In this case, carcinoid heart disease is the only manifestation of the syndrome.
@samyamshon Agree. We wrote a review (as humans), took months to generate original ideas and gather insights into data and write it. Took a year to get back from review. It’s going to be hard to do that type of work if there is just the academic equivalent of AI Slop clogging journals.
This is exactly what most of the "AI deskilling" and "AI will not replace doctors but rather doctors using AI will replace those who don't" gets wrong.
This technology will create new workflows, with their own advantages and risks. It will likely do this faster ...
Practice unfortunately has not changed since we published. Until NCCN endorses dropping the bolus it will persist. Not sure we can get a dataset larger than > 10,000 patient analysis (https://t.co/lZs4UfIaMB). No one wants to fund a Phase 3 trial front line in this space.
#ASCO26
5-FU bolus, leucovorin and DPYD… what are people actually doing in practice?
We’re running a quick 1–2 min survey looking at real-world patterns across adjuvant + metastatic CRC.
Would appreciate input from both academic + community providers.
https://t.co/nLga01z3lT
We’ll share results back.
Topline data from 55 ptnts in $IMRX Phase 2a trial of atebimetinib + mGnP demonstrates 17.3 mth median overall survival in 1L #PancreaticCancer - more than 2x standard of care. Full data to be presented on June 1st at the #ASCO2026. Learn more here: https://t.co/zLdlIApPC0
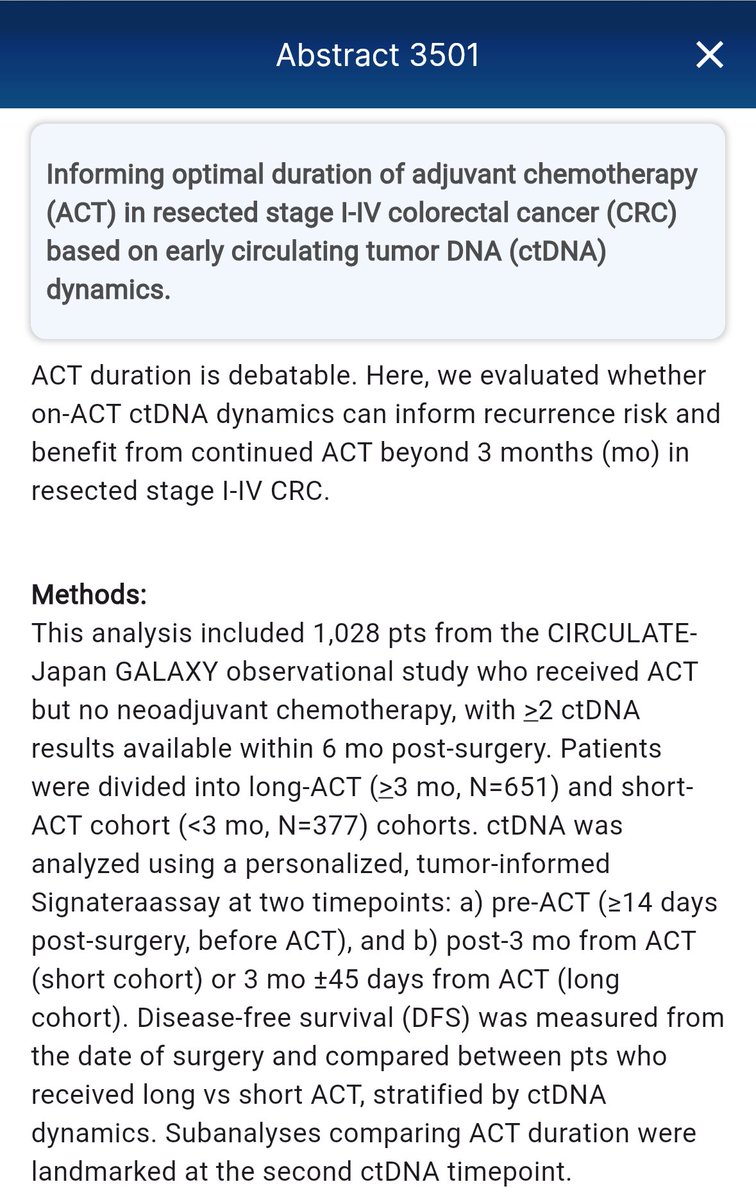
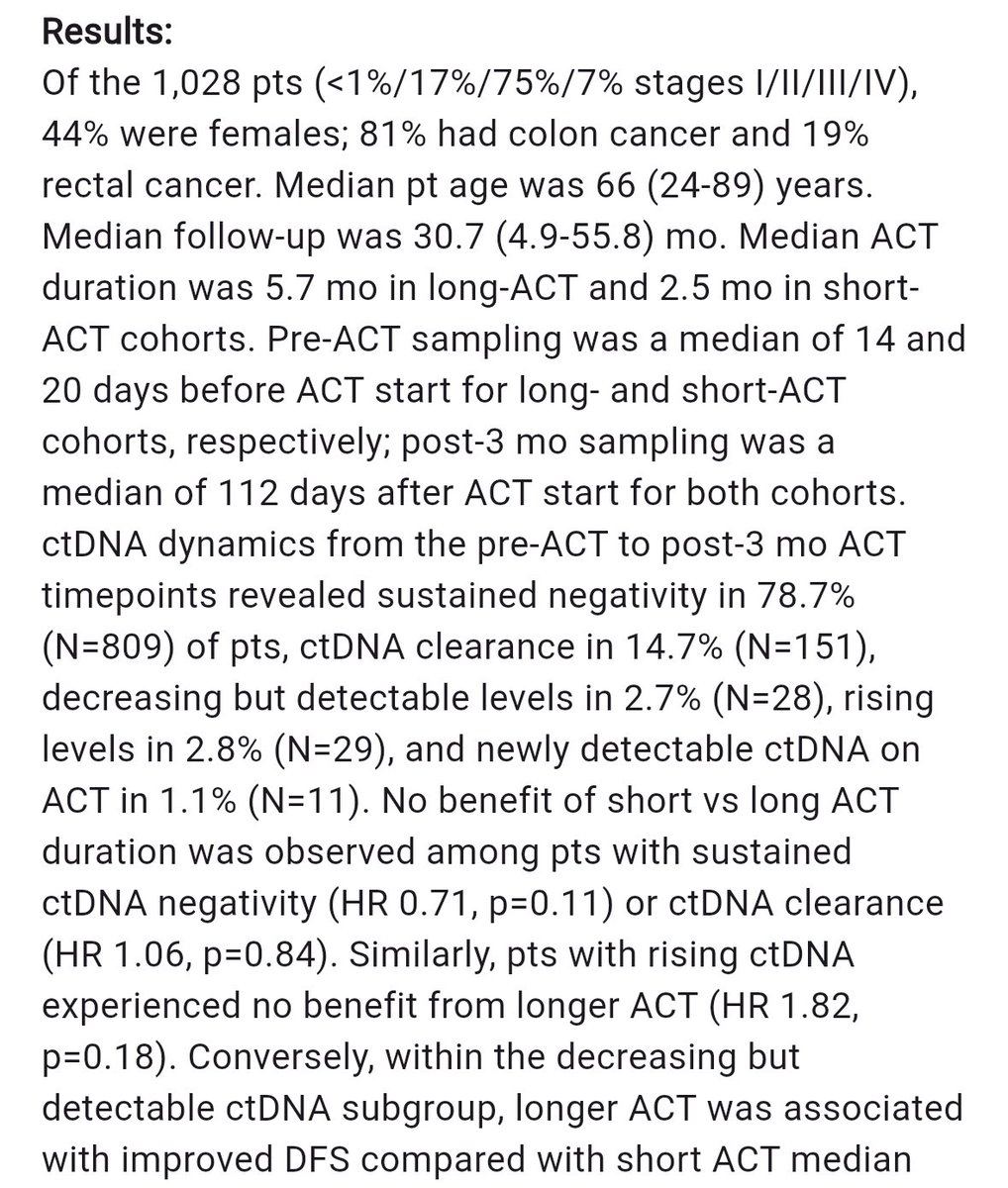
CIRCULATE-Japan GALAXY adj chemo (ACT) in StII/III CRC ➡️ 14.7% #ctDNA clearance, no benefit b/t short vs long ACT in this w/sustained #ctDNA neg or clearance, no benefit to longer ACT w/rising ctDNA but DFS benefit w/longer ACT in those #ctDNA+ and decreasing #ASCO26@OncoAlert
SBRT (50Gy/5fx, MR adaptive) in locally recurrent PDAC.
N=46 (7 w prior RT). 1 year LC 73%, median OS 19 mo.
Ablative RT = feasible, safe in locally recurrent setting & can confer long term dz control.
Great to see this data published - congrats @adapthyun & team! @OncoAlert
Would be interested in combination therapy role in very high volume metastatic disease with risk of organ dysfunction (e.g. extensive liver involvement) as a debulking strategy.
The AGITG CONTROL NETS is finally out in paper!
Does the CAPTEM-PRRT combo perform better than CAPTEM in patients with pancreatic NETs? Well, there is more in this paper than that but let's focus on the pNETs.
Bottom line: Complex trial, many moving parts, small cohort, does not and should not change practice.
More thoughts:
The study would suggest so with longer PFS in the PRRT/CAPTEM but the bigger question is how patients who got PRRT alone compare but that was not done here. Keep also in mind that the number of treated patients was very small.
The PFS in the PRRT/CAPTEM group was 59.4 months which is very impressive (For PRRT alone reference, it was 20.7 months in OCLURANDOM and 24.5 months in COMPETE).
There were only 2 patients (3%) among those who had PRRT who developed therapy-related myeloid dysplasia which is reassuring but also goes against what others have reported where the risk is as high as 10%.
Will this change anything for me? Absolutely not as I would need larger studies to be convinced and also, I am not sure the therapy sequencing matters that much as long as you get all the effective therapy during the illness.
But what this study does is to help revive the concept of chemo-PRRT and support the development of other trials looking at combining PRRT with systemic therapy and @AmanChauhanMD, I am looking at you now... 😉
https://t.co/jY7X4snvPq
🩺 THE 10 MOST IMPORTANT GI CANCER TRIALS OF #ASCO26
🌟 PLENARY & PRACTICE-CHANGERS
1️⃣ RASolute 302 (LBA5)
Daraxonrasib (RMC-6236) vs chemotherapy in metastatic pancreatic cancer
Can RAS finally become druggable in pancreatic cancer?
2️⃣ CIRCULATE (LBA3500)
ctDNA-guided adjuvant therapy in stage II colon cancer
Potentially the defining trial for escalation and de-escalation strategies.
3️⃣ EMERALD-3
Durvalumab + tremelimumab + lenvatinib + TACE in unresectable HCC
How aggressive should frontline liver cancer therapy become?
🧬 COLORECTAL CANCER PRECISION ERA
4️⃣ BREAKWATER Cohort 3 (LBA3503)
Encorafenib + cetuximab + FOLFIRI in BRAF V600E mCRC
Important real-world sequencing data beyond oxaliplatin-based therapy.
5️⃣ SWOG S2107
Sequencing optimization in BRAF V600E metastatic CRC
A major unmet-need clinical question.
6️⃣ STELLAR Update
Long-term survival update for TNT in rectal cancer
Do pCR gains translate into durable survival benefit?
🎯 GASTRIC, GEJ & RARE GI SUBTYPES
7️⃣ HERIZON-GEA-01 (4010)
Zanidatamab-based frontline therapy in HER2+ gastric/GEJ cancer
Could bispecific HER2 targeting redefine frontline care?
8️⃣ KEYNOTE-811 Mature OS
Final long-term OS update for pembrolizumab + trastuzumab + chemotherapy
Clinicians have been waiting for these mature survival curves.
9️⃣ ATTRACTION-6 Update
Checkpoint inhibitor strategies in advanced gastroesophageal cancers
The IO sequencing debate continues.
🔟 Bezuclastinib + Sunitinib (11500)
Phase III data in advanced GIST
A key resistance-targeting strategy in rare GI oncology.
Which GI abstract will change your clinic most?
#GIOnc #OncTwitter #ASCO26 #PanCan #ColorectalCancer #MedTwitter @ASCO@myesmo@esmo_open@OncoAlert
Evaluation and Treatment of Iron Deficiency for the Practicing Oncologist | JCO Oncology Practice https://t.co/OlPqUor0xf @JCOOP_ASCO@ASCO@OncoAlert one of the most common consults in General HemOnc Clinics