Under the IRA, Part D plans have responded to lower out-of-pocket limits with higher deductibles
The result is a sharp "tilting" of OOP spending through the year. Average OOP costs for brand fills are now higher in January, but sharply lower in later months as people hit the cap
AHRQ-funded researchers calculated the US could save $150M every year by switching from low molecular weight heparin to aspirin for blood clot prevention in orthopedic trauma patients. (That grant cost <$100K.) https://t.co/NqWBB3X0rx
Very interesting to get a deeper look at what Medicare coverage of the weight loss drugs might cost, taking into account existing rebates & considering the counterfactual that many are likely to gain coverage through other indications over time regardless.
Tough day for a 🚨new paper🚨, but nevertheless!
How much would it cost if Medicare was allowed to cover drugs approved for weight loss?
We estimate $3.1-6.1 billion per year in the near term.
Just out in @Health_Affairs (with @jlevy2)
https://t.co/2Q0ZkT88nF
🚨 New publication alert 🚨
I am so excited to share that I published part of my dissertation work in JAMA HF. A huge thank you to these co-authors: @KellyAnders0n, @jlevy2, @healthecon_dan, and the twitterless Thomas V Johnson and Jerry Anderson
https://t.co/LdwyWqeFRb
We've drafted a response to the recent CMS RFI on additional data collection to study the Medicare Advantage program. Want to sign on? Send me an email by Friday March 8th
https://t.co/YMTgi9jiBy
FDA approval of 2nd potent GLP-1 for treatment of obesity - Lilly’s drug Zepbound - will accelerate discounting as competition heats up, reducing costs and extending access to patients. A prior @AEIecon analysis captured magnitude of earlier discounts
https://t.co/fNouMWWgk0
@a_kaltenboeck Sorry!I missed this reply! I was not talking about list price.I was saying a good model of how prices will now evolve(absent competition) bc of IRA is net prices will increase by CPI from launch,until 9year=small molecule,13y=biologic, and then drop by min of 25% @dollendorf
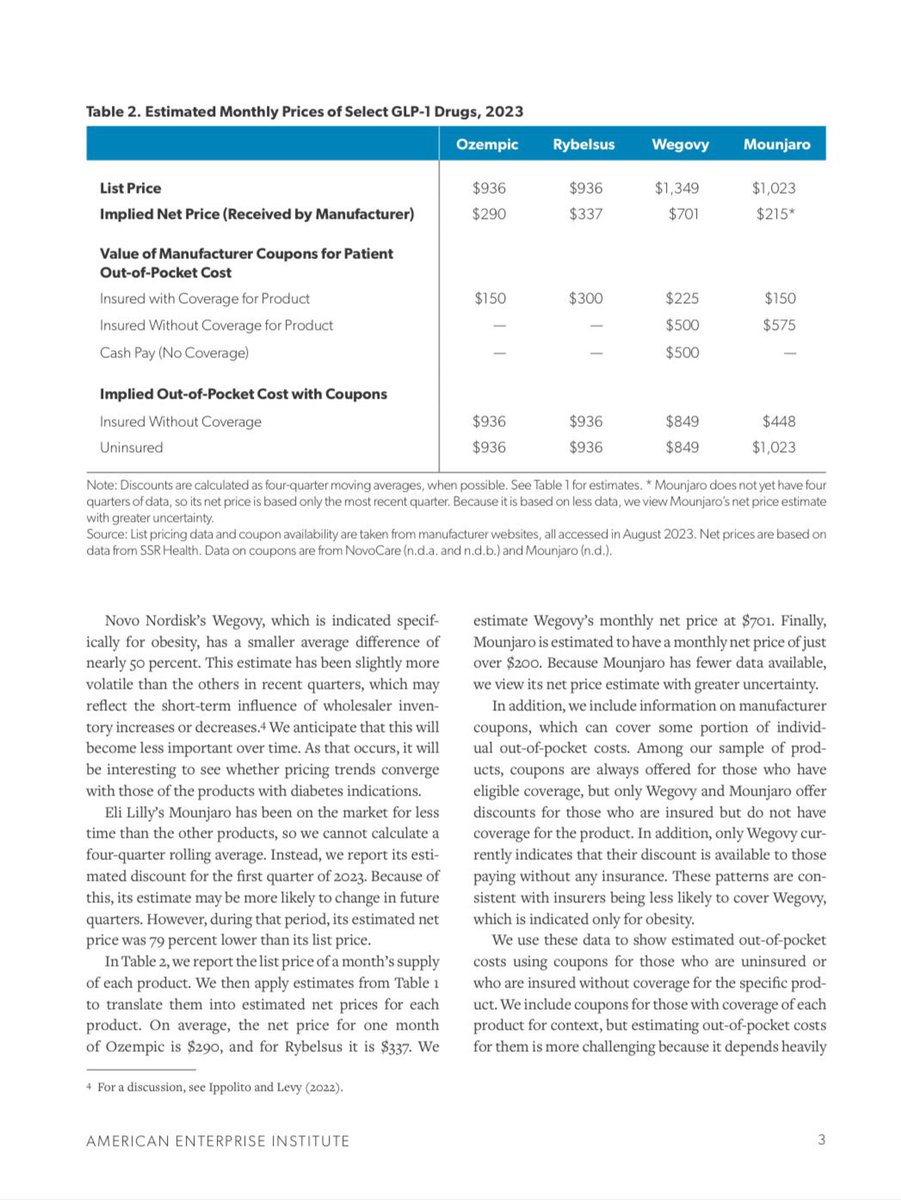
Ozempic, Wegovy, and other GLP-1s perfectly illustrate the common (and large) gaps between list and net prices of many brand drugs.
A summary of our work: "Ozempic and Wegovy Don’t Cost What You Think They Do" via @nytimes
https://t.co/eXzEeHiFr9
@a_kaltenboeck absent novel competition a now reasonable assumption is that drug prices will increase by inflation for ~7 years, then in year 8 should drop 25% (or more). If new competition enters, new CEAs that take this into account are required, and the old CEAs become irrelevant (2/2)
@a_kaltenboeck Any CEA conducted by CMS (or anyone) will know the launch price, so I don't think that is what they are arguing, of course CEA models should use the new (and I agree) likely higher launch prices. This is about how the price estimate built into the CEA should change over time(1/2)
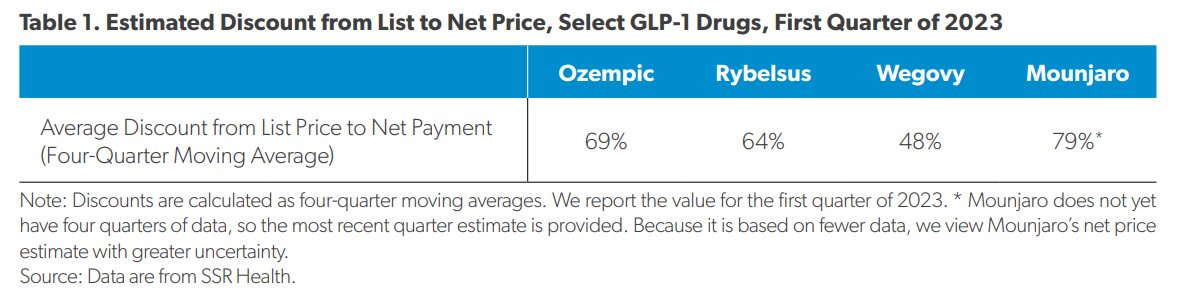
Hmm: New @AEI study estimates huge #GrossToNetBubble for GLP-1 #drugs. Net prices far below list prices due to #PBM#rebates & manuf copay support 👇
Perhaps economic impact has been overestimated?
Full report: https://t.co/hYaaFidp9A
Now in print, @jlevy2 and I test whether coverage of brand drugs in Part D differs based on whether the drug is a "good" or "bad" value relative to cost-effectiveness estimates.
In short, it does not.
https://t.co/0lbeHq3rHy
Defining “the price” of brand drugs like Ozempic can be complex. Our white paper summarizes what we know about the prices of new treatments for diabetes and obesity
Short story: Very big differences between list and net prices, even adjusting for coupons
https://t.co/wfBqEi9yYw
CMS will use comparative effectiveness to adjust the starting point in price negotiations, but how exactly?
We adapted the French system (added benefit ratings linked to domestic reference prices) to model one approach and estimate savings. @jlevy2
https://t.co/5oJpxrjo7a