The cost and slowness of Phase I clinical trials is one of the main reasons why the US is falling behind China in drug discovery. There are countless patients with terminal cancer who miss on novel therapies & countless of never discovered drugs. More👇
https://t.co/bGuzB7AXzu
Zoning adds $300 - 500k to the price of a home in cities with good jobs. High-speed rail takes 30 years to build. New drugs cost $2B. We pay 5-10x what peer countries do for the same infrastructure.
People call this "regulation." It isn't, exactly. It's stranger and worse. 🧵
AI dangers: Epic used #AI in computerized medical record to predict #sepsis, touted it highly, widely used. First investigation, sensitivity 33% (missed 2/3 of cases, specificity 83%, 88% alerts false positives, alert burden: 6,971 of 38,455 hospitalizations (18%). Withdrawn after 4 years of damage.
https://t.co/3QYM1XreEW
Many aspects of American healthcare that patients dislike are downstream of having a third party (insurance) pay for services that should simply be paid in cash or HSA. Probably true for physicians too.
Health insurance should be insurance, not some weird group purchasing scheme. You don’t need to submit to the humiliation of 8 pages of paperwork and several frustrating phone calls to buy a haircut and it shouldn’t be true for a primary care visit either.
Nor does someone who does a new haircut need to lobby the haircut board to create a haircut billing code like 92133 “ZOOMER BROCCOLI CUT W/ FADE”.
We know markets work. Healthcare isn’t some magic part of the economy that defies the laws of physics. E.g. LASIK which is all cash pay has gotten cheaper in real terms and better since the ‘90s.
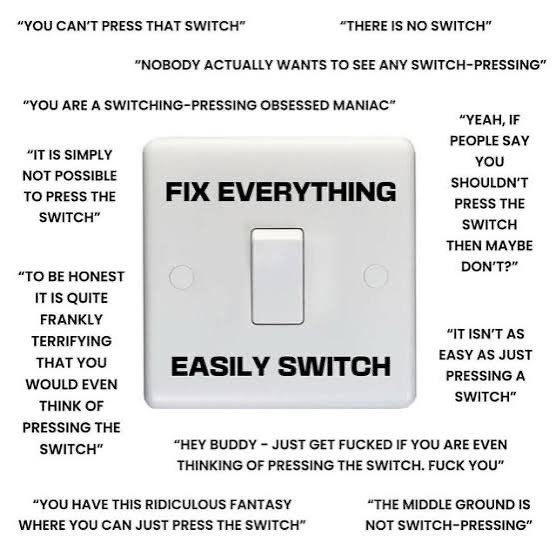
The preciousness of healthcare doesn’t need to blind everyone to common sense and evidence. There is a button and you can just push it.
1/14
Why can't you use direct oral anticoagulants (DOACs) in patients with mechanical valves (MVs)?
DOACs have been one of the most important advances in my career. And yet, the presence of a MV is one of the few contraindications.
The reason highlights the unique nature of thrombus formation in those with a MV and provides insights into the evolution of human hemostasis.
Another midwit healthcare take.
Other countries have better life expectancy than the US. That is not the same as better healthcare outcomes.
Life expectancy is primarily affected by things that kill the young. In the US, that is violent crime, car accients, overdose, and suicide. You can argue that healthcare might be able to influence the last two, but only minimally. Those things are driven by lifestyle choices. Add in our obesity rate, which is also only marginally mitigated by proper healthcare, and you see why our life expectancy is lower than the rest of the OECD.
We are fat, violent, depressed, and like driving on freeways.
Now, if you acutally get sick, there's nowhere else you'd rather be. We have some of the best outcomes in cancer, stroke, heart attack, and trauma. The wealthy from around the globe travel to our hospitals for care. There are entire wings at some prominent hospitals for ultra rich international patients. They aren't going to the NHS for their care.
We excel at coverage for actue care. 98% of Americans are within 90 mintues of a cardiologist who can open up the arteries in your heart in the middle of a heart attack. Meanwhile, in canada, that number is around 80%. They have 10x worse access to acute coronary care than the US.
If you're going to have a heart attack, you want to have it in the US.
If you're going to have any health issue requiring high specialty care, you want to be in the US.
🫀 Grading severe aortic regurgitation — time to upgrade our TTE approach.
ASE criteria alone show an AUC of only 0.58 on prospective validation. This novel 2-step algorithm, benchmarked against CMR, does better:
1️⃣ AR regurgitant volume ≥ 45 mL (PISA or Doppler)
2️⃣ LVEDVi ≥ 93 mL/m²
→ Both met? Severe AR. AUC up to 0.76 with PISA method.
Simple. Reproducible. CMR-validated.
EHJ Cardiovascular Imaging — doi: 10.1093/ehjci/jeag012
#Cardiology #Echocardiography #AorticRegurgitation #ValvularHeartDisease #CMR #CardioTwitter #MedTwitter #EACVI
this claim is always funny for 2 reasons — (1) you can’t pick a non-quantitative profession in the world more explicitly didactically trained in bayesian stats than physicians, (2) you can’t pick a group of people more interested in low PPV tests (MRI/labs/etc) than Bay Area tech
Password rotation or Forced changes lead to "password hedging," where users just add a number or change one letter (e.g., Summer1! becomes Summer2!).
It is biologically impossible for most people to memorize a high volume of complex, random strings every few months, leading to "sticky note" security risks.
When security is a hassle, users find dangerous shortcuts, like reusing the same "strong" password across every site they own.
The most important fact is that NIST (National Institute of Standards and Technology), the global authority on cybersecurity standards, officially retired this method
In its Digital Identity Guidelines (SP 800-63B), NIST now explicitly states that organizations "SHALL NOT require" periodic password changes.
They’ve shifted the focus to Length over Complexity.
They recommend allowing passphrases of up to 64 characters and only requiring a change if there is actual evidence of a compromise.
This is, imo, the most achievable and best singe answer to this question as well. the local municipalities issue is probably our single greatest. it holds back immense economic growth and general societal development.
https://t.co/vXTuFydCs5
Yesterday I spent more time helping patients figure out how to pay for their medications than discussing their actual medical concerns.
This is how the souls of physicians die.
Not all at once, but one paper cut at a time.
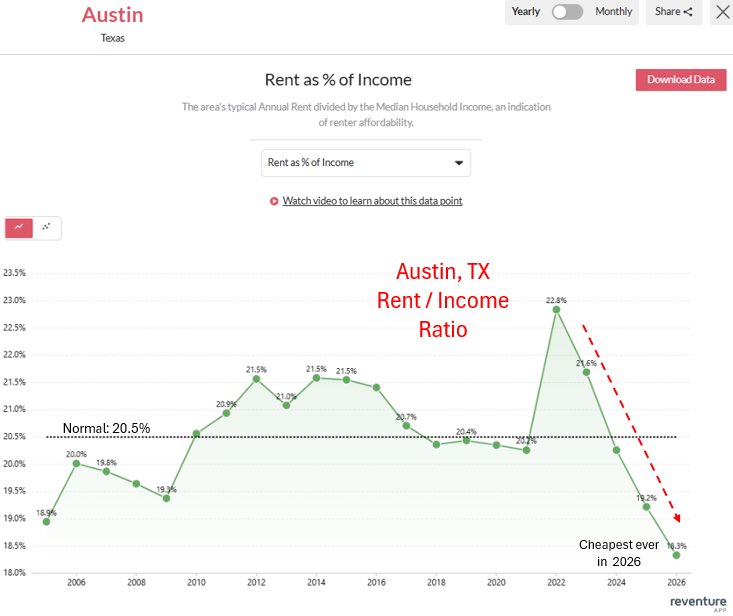
Austin tried to pass rent control, but the state didn’t allow it. Instead, we allowed developers to build. Now it’s cheaper to rent in Austin as a % of income than in decades.
Move to states and cities that build things instead of having virtue signaling policies that don’t help
Whenever you see a contextless large number you should be pretty skeptical.
My hometown of 17,000 people uses 1.5 million gallons of water per day. Enough for 21 data centers like this. If you saw someone saying that the American west cannot afford to have 17,000 more people move there I think you'd be a little suspicious.
Irrigated alfalfa farms use about 3-4,000 gallons per acre per day, and there are 6 million acres of irrigated alfalfa in the west. That one crop (which mostly goes to feed livestock) is using as much water as 500,000 data centers at this size.
Data centers are always going to basically round to zero on the list of the west's water issues.