More evidence for prehospital transfusion?
A very timely paper on prehospital transfusion, with all of the recent conversation around SWIFT.
This study compared WB to PRBC’s across 9 prehospital transfusion programs in the US. Note the difference in mortality between UK HEMS study and US ground EMS: 27% vs 12.7%. Prehospital time in SWIFT 67 minutes vs median 23 in the US study (34 min total from 911 call to ED arrival!). WB associated with lower in-hospital transfusion requirements and improved survival for blunt injury patients, with a trend toward improved survival in the total cohort.
Key lessons learned from this paper:
1) prehospital transfusion is possible and effective in ground EMS agencies, even with short transport times
2) whole blood may be better, particularly for blunt injury
3) earlier resuscitation for hemorrhagic shock improves outcomes (which may be why neither SWIFT nor RePhill showed any difference)
4) availability of whole blood should not be the rate limiting step in getting a prehospital transfusion program started
https://t.co/H5SBkrI1w3
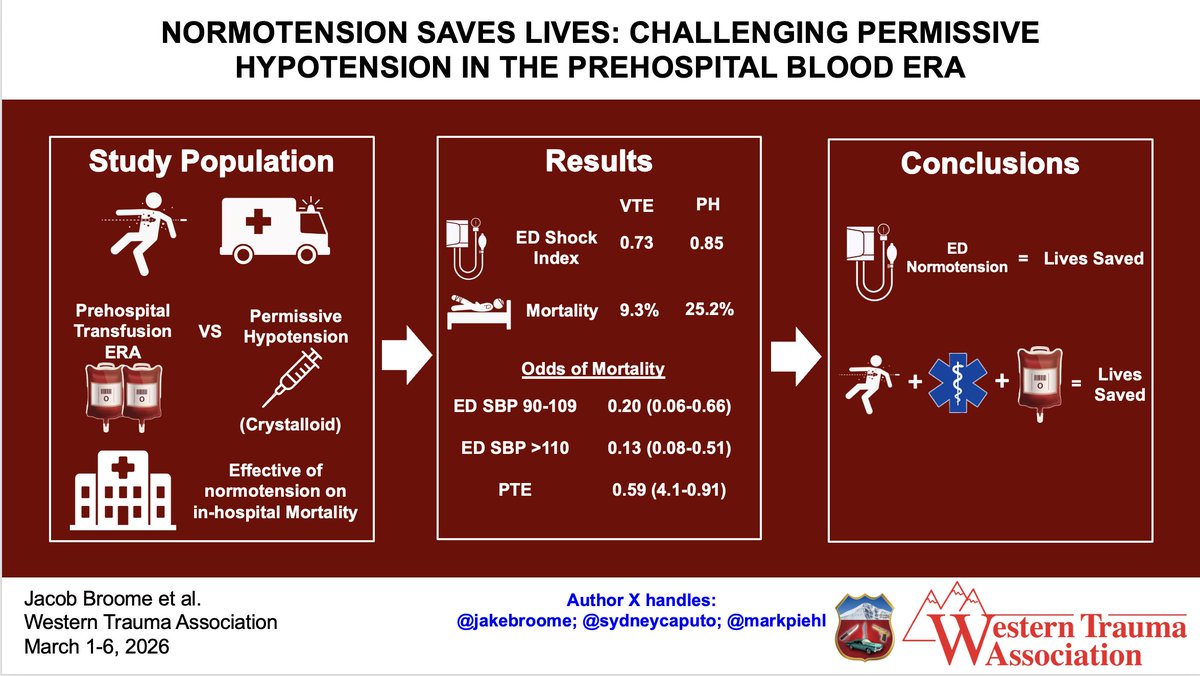
@WesternTrauma@JakeBroome@SydneyCaputo We definitely need to re-evaluate traditional permissive hypotension targets when blood is transfused in the field. This study and another presented this week @WesternTrauma suggest 110 may be optimal, even for NCTH. Less duration of shock = better outcomes
Thank you @HandtevyMD for sharing this amazing case and for the incredible care provided by the Palm Beach County Fire Rescue and City of Palm Beach Gardens EMS crews! Similar to the trauma case you presented a few weeks ago, this patient needed active resuscitation provided quickly so that BP and perfusion could be restored and he didn't progress to cardiac arrest. The immediate improvement in mental status tells the story. Obviously I'm biased, but for patients with severe shock like you describe here, gravity or a pressure bag just can't deliver the fluid (or blood in hemorrhagic shock) needed when minutes truly matter. This is particularly true with an IO. You also show that effective resuscitation doesn't mean a lot of fluid, rather just enough given quickly to reverse shock. That's the point of LifeFlow
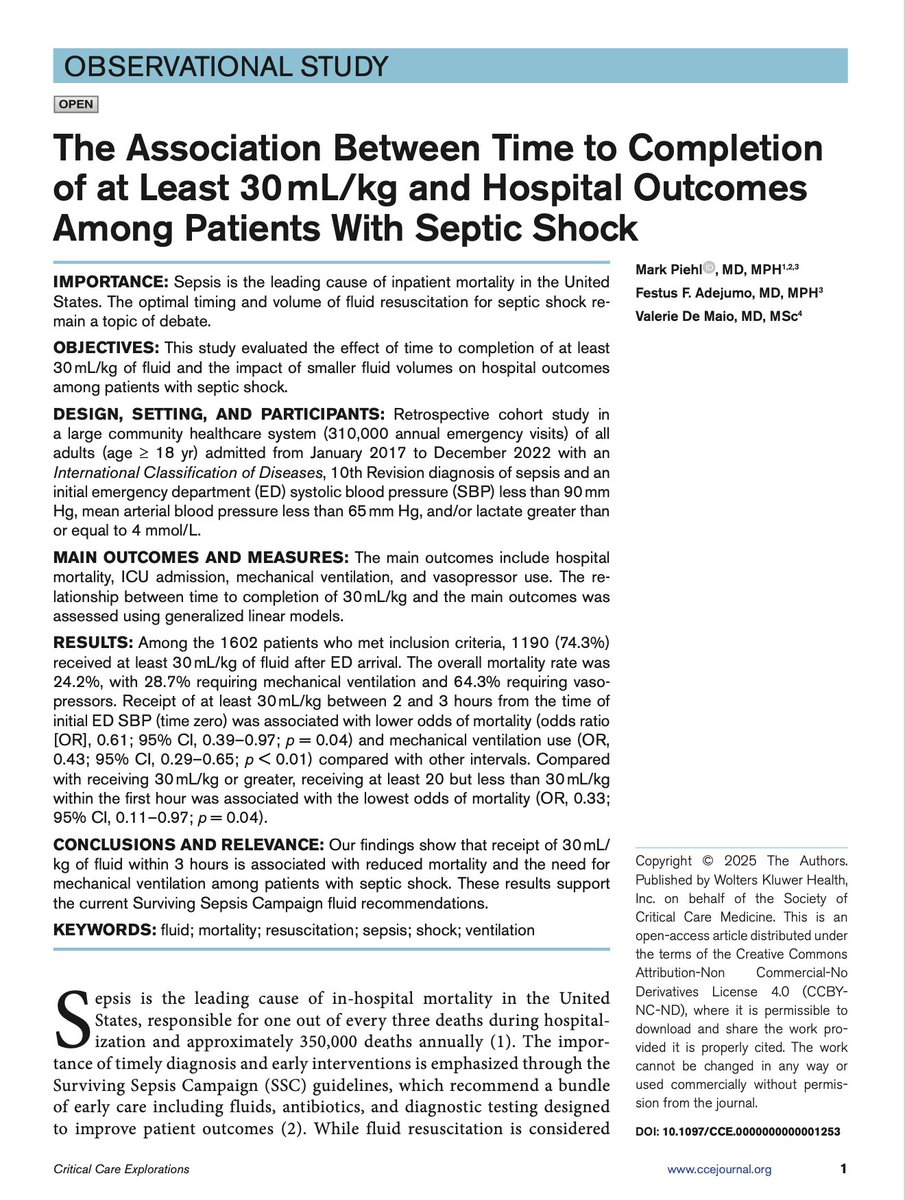
Is the Surviving Sepsis Campaign fluid recommendation of 30mL/kg safe & effective? Turns out it is. Not every patient with sepsis may need 30mL/kg, but for septic shock (SBP < 90 and/or lactate >4), 30mL/kg by 3hrs is associated with lower mortality and less mechanical ventilation. And 20-30mL/kg in the 1st hour may be the optimal volume and timing for these patients. Check out our observational study of 1600 patients @WakeMed
here: https://t.co/hi9CYzW3lU
#sepsis @SCCM #CritiCareExplore
@VCFD_PIO@OxnardFire@CountyVentura@AMRVENTURA@VCMC_TraumaDept@VitalantCA Thank you @VCFD for sharing this incredible story and for saving a life by delivering whole blood within minutes of arrival to the scene. You are leading the way to improved trauma care in California, hopefully many other agencies will soon follow!
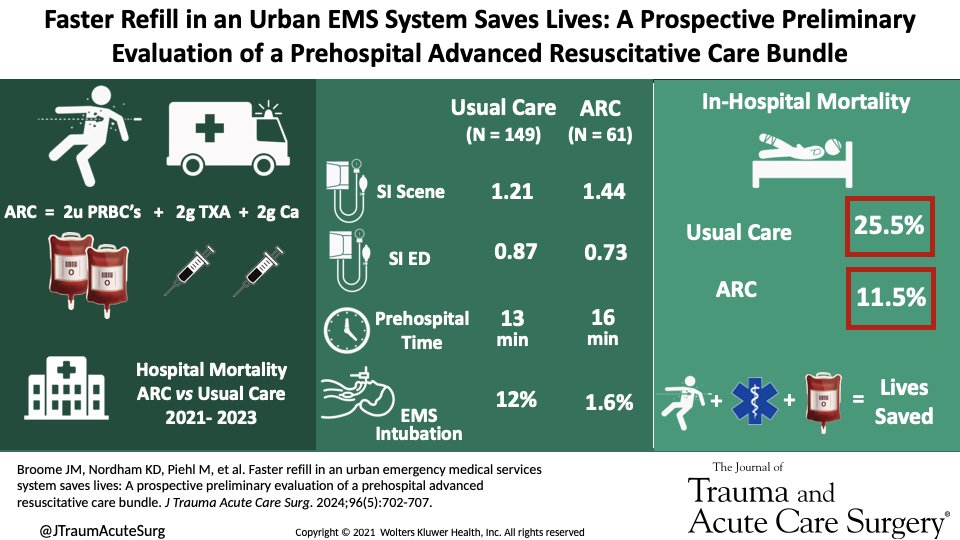
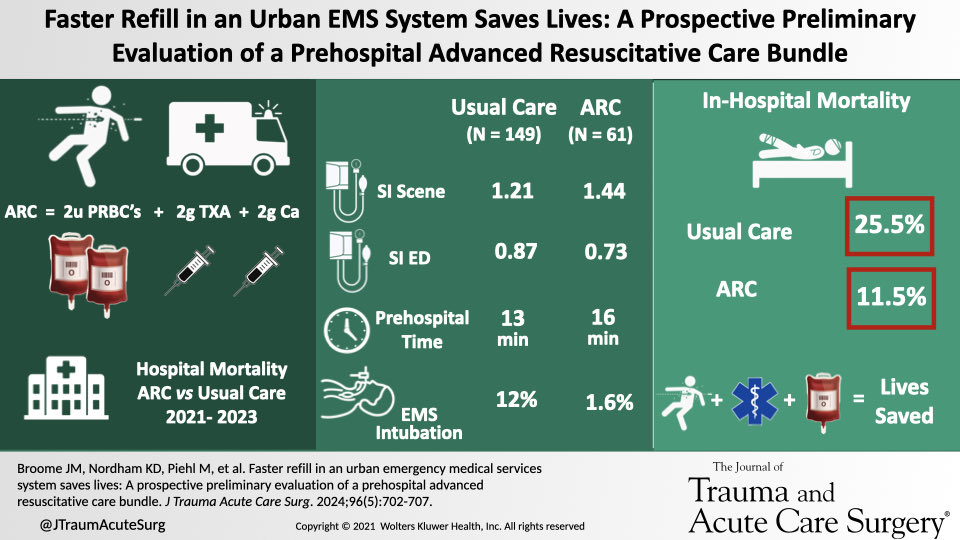
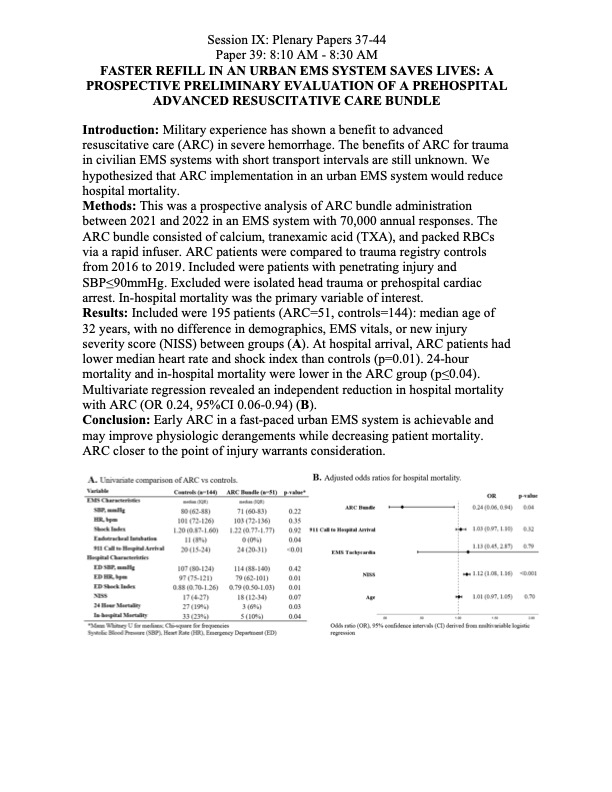
Thank you @DrJeffJarvis for a thoughtful review of our Faster Refill paper! You do make some fair points about potential methods improvements while acknowledging the strength of the results, which are the first ever to show a trauma survival benefit for blood in urban EMS @HandtevyMD@JakeBroome
🚨 New Episode Alert! 🚨
Can prehospital blood save lives? 💉 Dr. Jeff Jarvis dives into the "ARC Bundle" (blood, TXA, calcium) and its impact on trauma care with an 81% mortality reduction. 🎧 Listen now at https://t.co/SM4RlfHuKP or on your favorite platform!
The @dcfireems team under the leadership of Holly O’Byrne and @EMSPhysician David Vitberg has saved many lives, again disproving the myth that urban agencies with short transport times shouldn’t carry blood. This will be an incredible webinar!
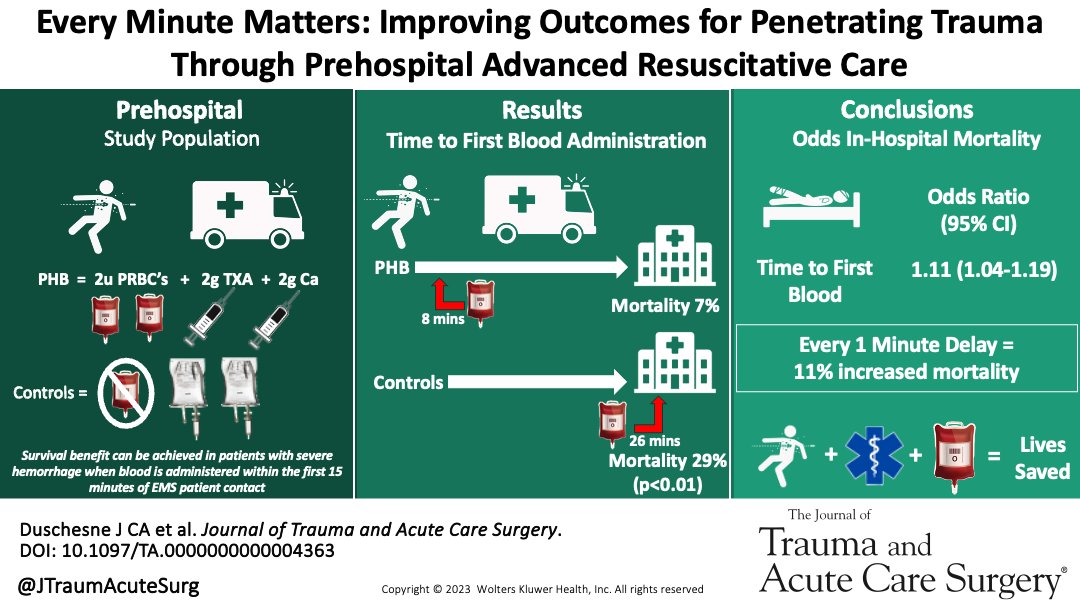
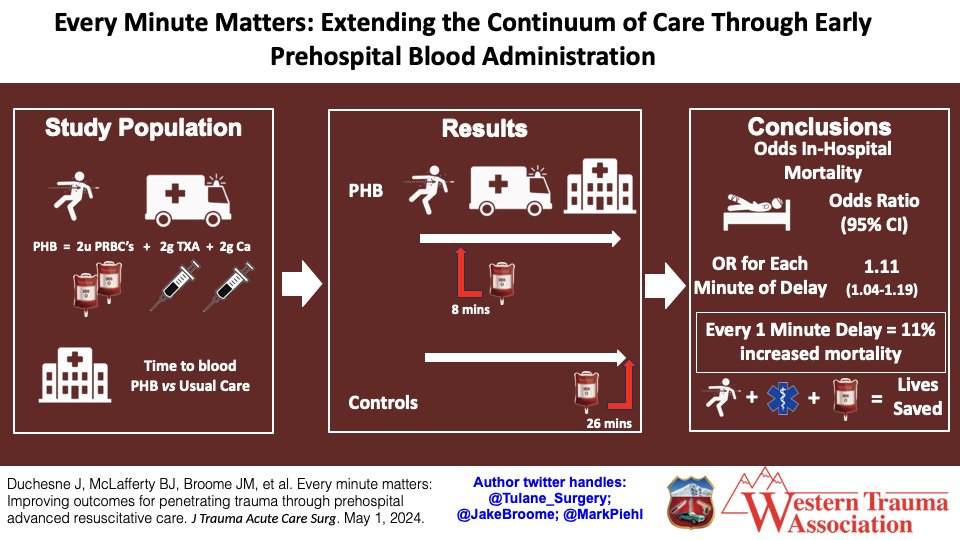
Exactly @HandtevyMD! This paper nicely addresses Myth #1 in the prehospital trauma debate: we are too close to the trauma center to bother carrying blood. Well, the data here show that for penetrating trauma with hemorrhagic shock, every single minute of delay in starting blood (and delivering an adequate volume to reverse shock) increases mortality by 11%. We don’t magically start effective resuscitation the minute a patient hits the trauma bay doors, therefore our EMS colleagues can do a whole lot of good getting that resuscitation started closer to the point of injury!
Everyone in EMS should take the time to read this…
Then go do it.
Every day you wait, people in your community are missing out on a lifesaving resource.
@JTraumAcuteSurg@Tulane_Surgery@JakeBroome Yes it does! For penetrating trauma with hemorrhagic shock, very single minute of delay in starting blood (and delivering an adequate volume to reverse shock) increases mortality by 11%. This is one of the best arguments for deploying prehospital blood in ground EMS
Our data suggest that prioritization of prehospital transfusion improves survivability in patients with severe hemorrhage despite a modest increase in transport time.
@Tulane_Surgery@MarkPiehl@JakeBroome
https://t.co/7UZpIElL1J
Thanks @FireMedic40NJ it was a total privilege to join Mike Carunchio and @HandtevyMD on Okayest Medic! We discussed the recent @AcademicEmerMed article suggesting there isn’t enough evidence for blood in ground EMS, and our editorial challenging the authors.
https://t.co/XLUMSV9gP9
https://t.co/xoTXQfQUzz
If you can’t access our letter, here’s the basic summary:
Schoenfeld & colleagues analyzed three RCT’s on prehospital blood including:
PAMPer - an air medical trial of plasma for trauma
COMBAT - an urban EMS study of thawed plasma, and
RePHILL - a UK air medical trial comparing blood products to crystalloid
Only PAMPer showed some benefit during 40 minute transports, and in RePHILL resuscitation wasn’t actually started until about 50 min after EMS arrival. None evaluated the “advanced resuscitative care” package of blood, TXA, and calcium currently administered fast-paced ground EMS agencies, which is the new damage control resuscitation: immediate hemorrhage control where possible, basic airway support, and rapid hemostatic resuscitation with blood to reverse hemorrhagic shock en route, then advanced airway only when necessary after transfusion. Outcomes from @NewOrleansEMS, @dcfireems , Grady EMS, @TidewaterEMS, Orange County (Fl), Palm Beach County Fire Rescue, BSO, and so many others tell the story. Importantly, the Faster Refill study from New Orleans showed an odds ratio of 0.2 for mortality among patients who got blood, a huge survival benefit.
We conclude our letter by countering the Schoenfeld, et al claim that there is still equipoise on prehospital transfusion vs the old standard of care. Many details still need some good research, but we know now that early transfusion in the field saves lives
@SPARC2024
Does every meaningful clinical innovation really require an RCT before it's widely deployed, as Schoenfeld & colleagues suggest in their meta-analysis on prehospital transfusion for trauma? Our editorial questions the relevance of the studies they review and points to evidence, and to the recent experience of many urban and rural EMS agencies, supporting early resuscitation with blood closer to the point of injury.
https://t.co/XLUMSV9gP9
https://t.co/xoTXQfQUzz @HandtevyMD @ResusOne
Meta-analysis from Dr. Schoenfeld found no significant one-month mortality benefit to civilian-setting prehospital transfusion. This should give pause to EMS systems considering transfusion programs #EMS#Transfusion@BIDMCEM#AEM#EM
@georgoff@LifeFlow__ Yes sir @georgoff the team at @dcfireems is doing an incredible job bringing effective resuscitation with whole blood close to the point of injury. Excluding field arrests, survival for their critically ill trauma patients is 90%
@Eddyjoemd you are right less fluid in ICU is better, but this article misses the point: early fluid titrated to shock reversal, not liberal or restrictive, improves patient outcomes. 2 abstracts at #ACEP24 this week showed lower mortality, less mechanical ventilation, and lower cost among septic shock patients who got 30mL/kg before the 3rd hour, consistent with the earlier work of @hanikuttab & Michael Ward. Similarly a recent #SAEM24 abstract showed the lowest mortality for septic shock patients who received 20-30mL/kg in the 1st hour. Like CLOVERS, the Taniguchi paper has nothing to do with effective early resuscitation in EMS & ED https://t.co/1eTt4AtqEg https://t.co/1CxAYFbvQa
@armyemdoc@JTraumAcuteSurg@LifeFlow__ Thanks Steve! Still not clear exactly how each element contributed to improved mortality, but a simple bundle for hemorrhagic shock seems to work well, even with short transport (~8 min). The most important component is of course the blood, but TXA and calcium probably help too