Excited to present our poster evaluating the efficacy and safety of the addition of SBRT to atezolizumab and bevacizumab in advanced HCC at #GI24. Thanks to @Salthecancerguy for the 📸
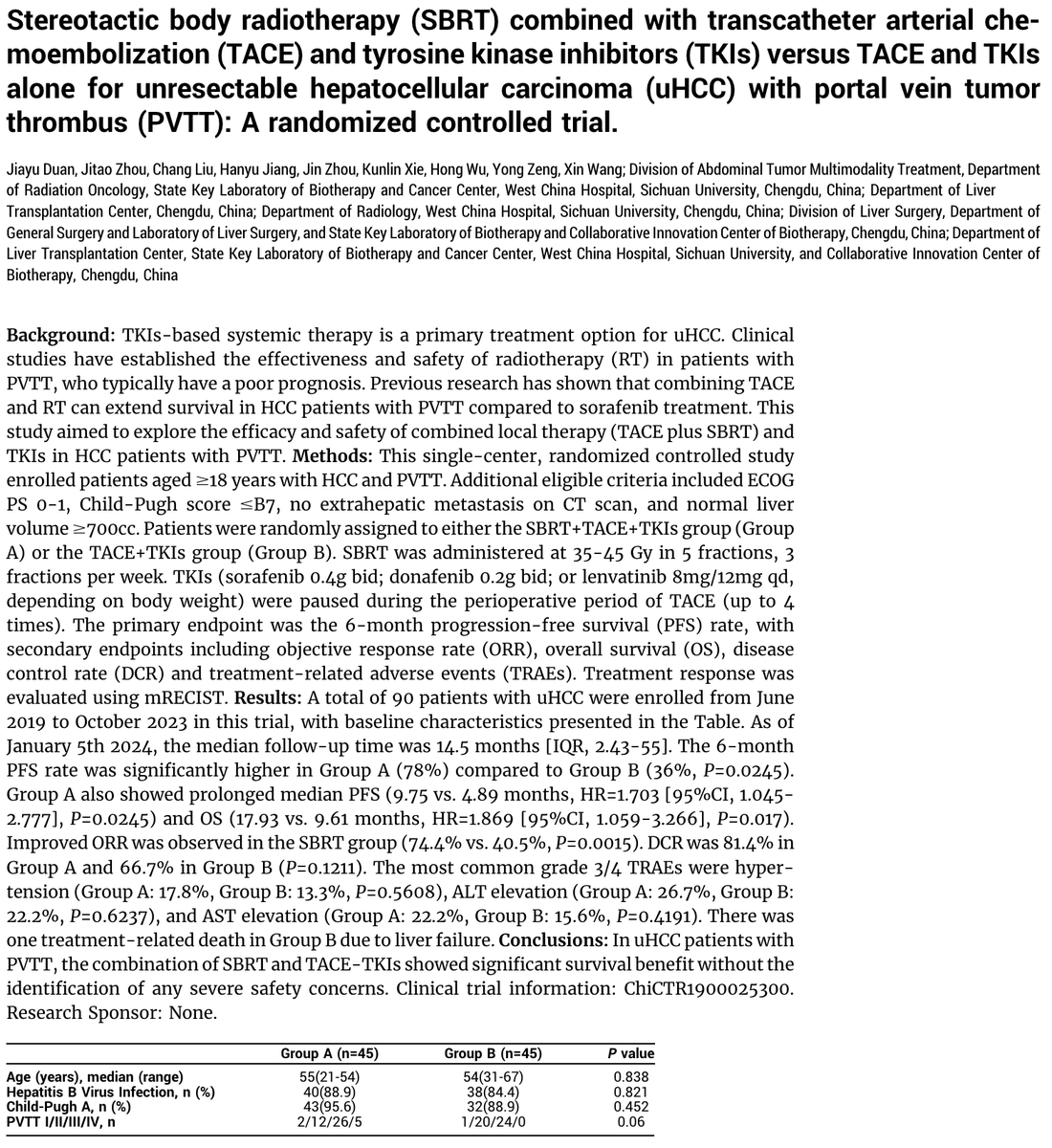
🚨🚨Ph2R Trial of M0 HCC with PVTT (n=90)
Comparing:
TACE + TKI + SBRT
vs.
TACE + TKI
✅⬆️ mOS with addition of SBRT☢️ (17.9m vs. 9.6m)
✅⬆️6m PFS with SBRT (78% vs. 36%)
🔥🔥🔥 The data supporting SBRT for localized HCC w/ PVTT continues to pile up!!!
#ASCO24
@PBlanchardMD at #SABR2025 - as usual a nuanced, balanced discussion of the role and risks of the role of SABR in head & neck cancers - upfront, in oligomets and re-#radiotherapy#radonc
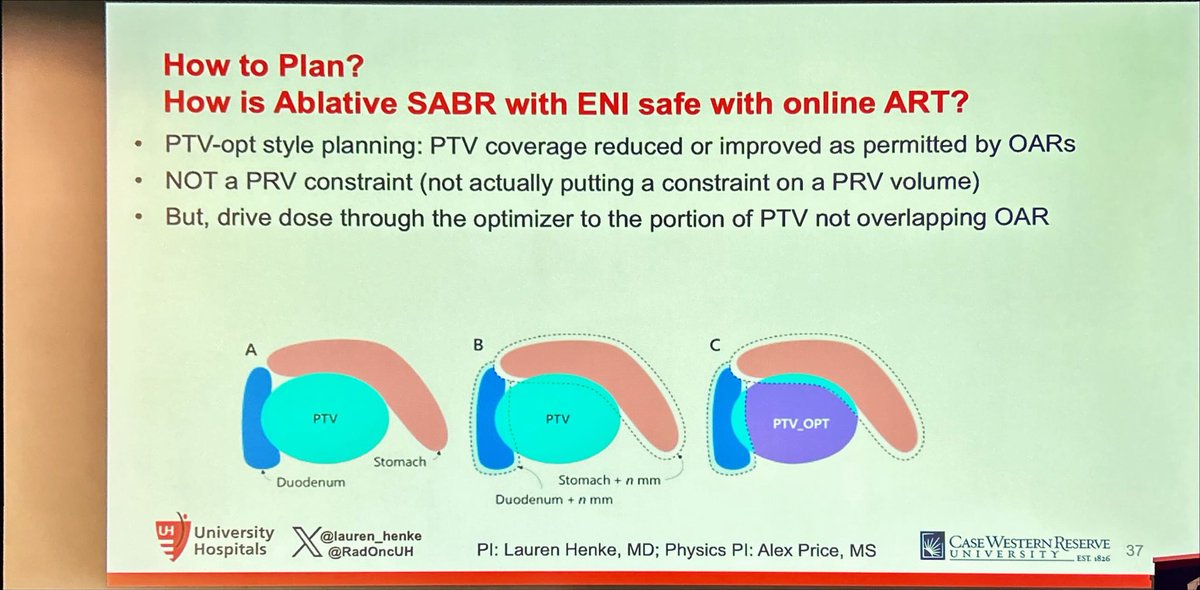
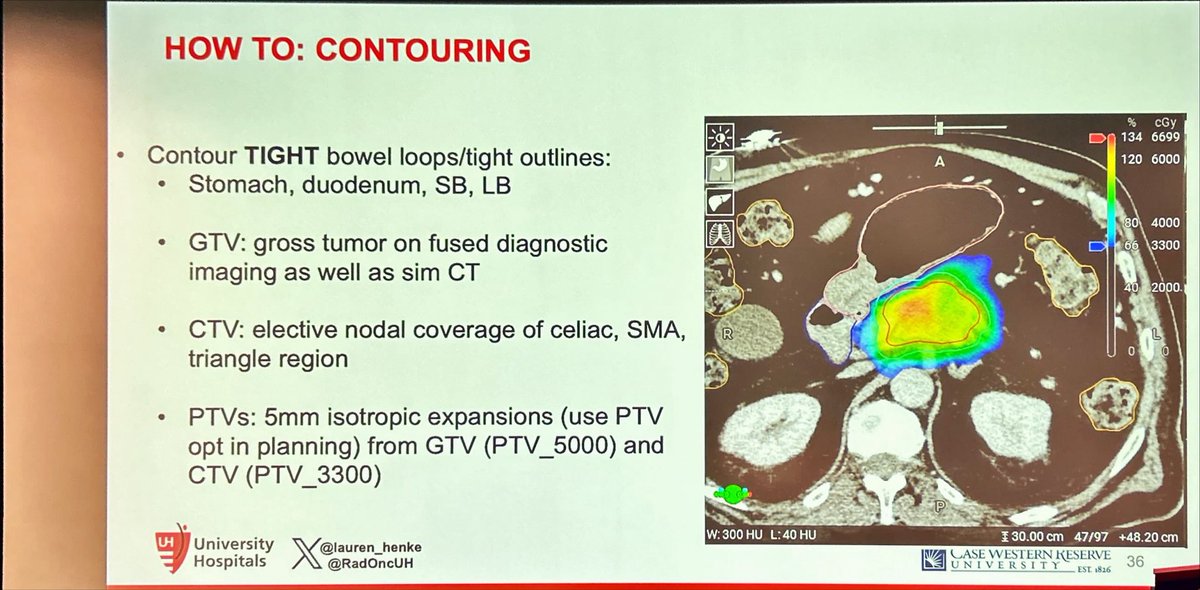
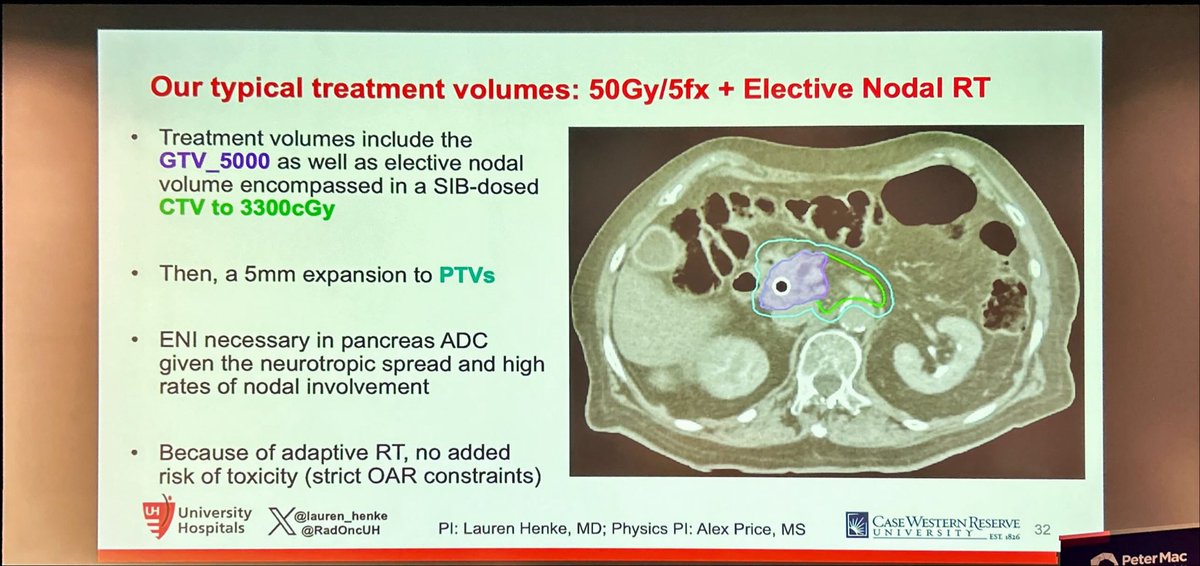
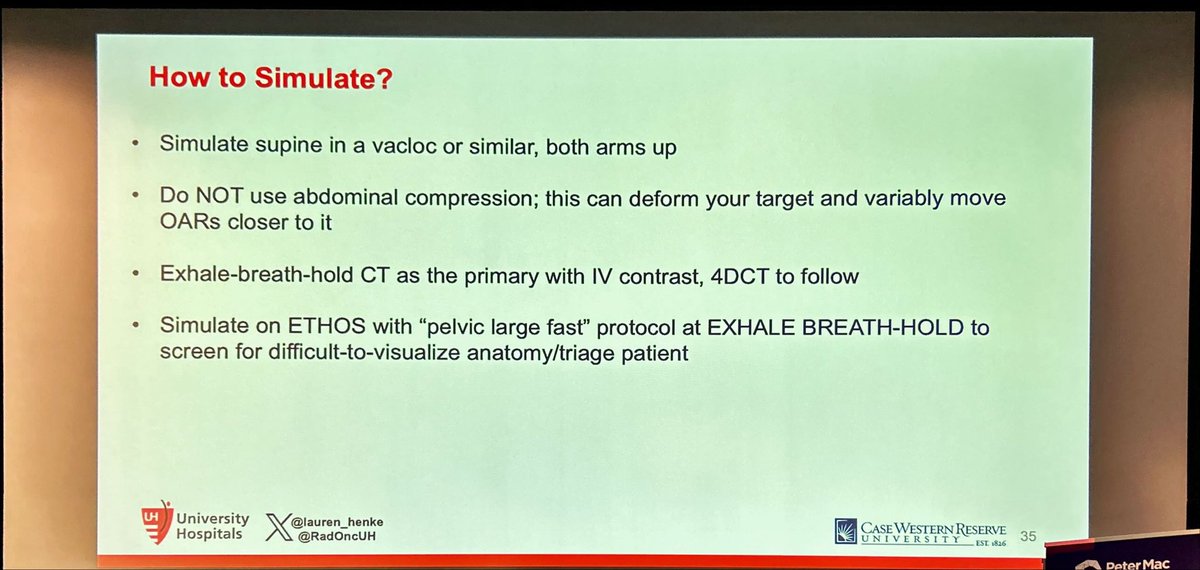
Practical step by step guidance on how to perform pancreatic #SBRT by @lauren_henke at #SABR2025#SBRT is the best way to deliver BED>100Gy to this tumors, which likely drives superior survival in #PancreaticCancer
📣@DrewMoghanaki - “this talk is going to make some of you uncomfortable”… 🥹 good on you Drew for pushing the boundaries in #lungcancer#radonc - Final talk of #SABR2025 🙏🏽
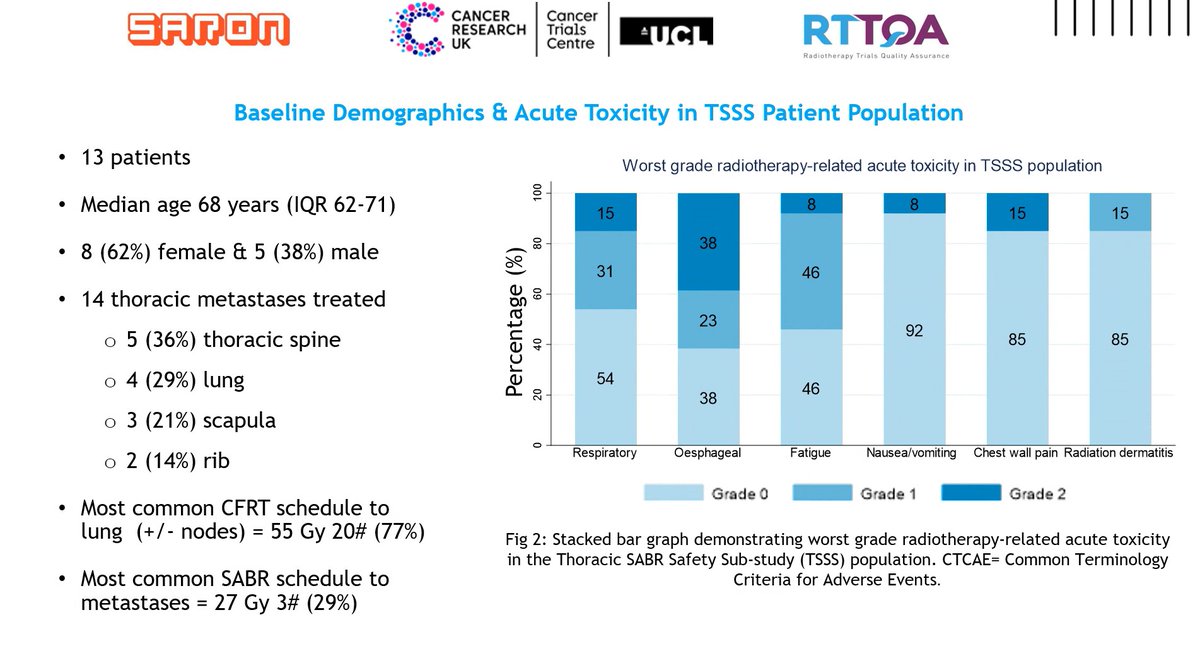
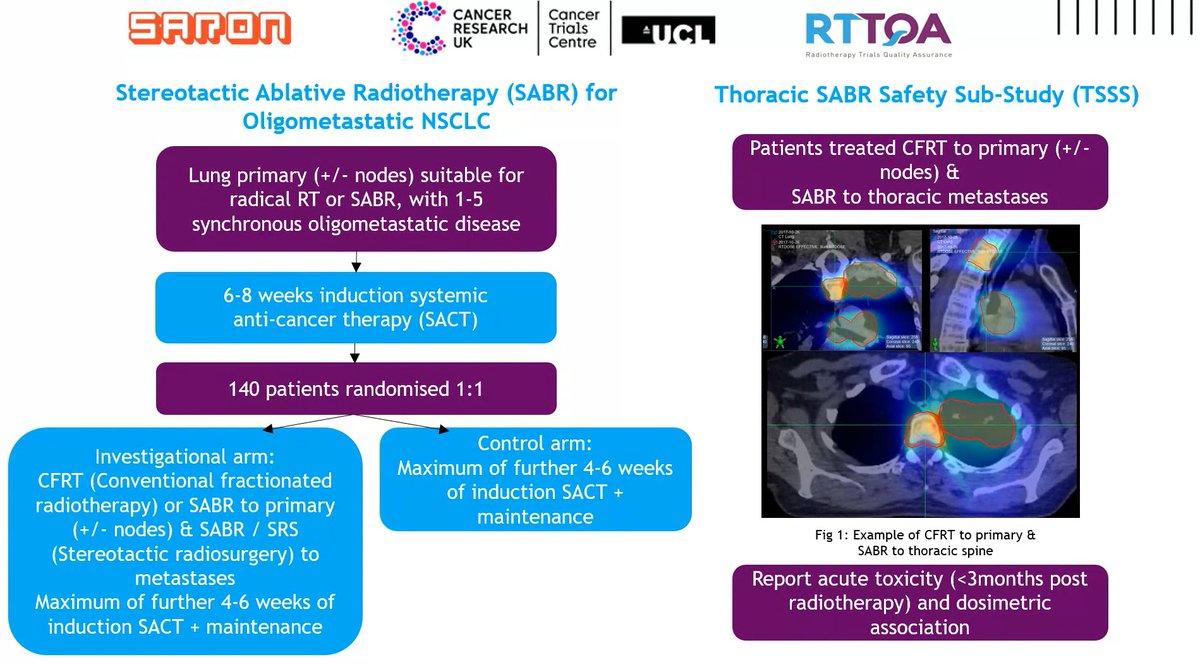
Really great to see Thoracic Sub-Study of our SARON study presented at #ESTRO25
Simultaneous delivery of CFRT to primary (+/- nodes) &
SABR to thoracic mets in synchronous OM-NSCLC
➡️Acceptable acute RT-related adverse
events
➡️No grade >3 adverse events observed
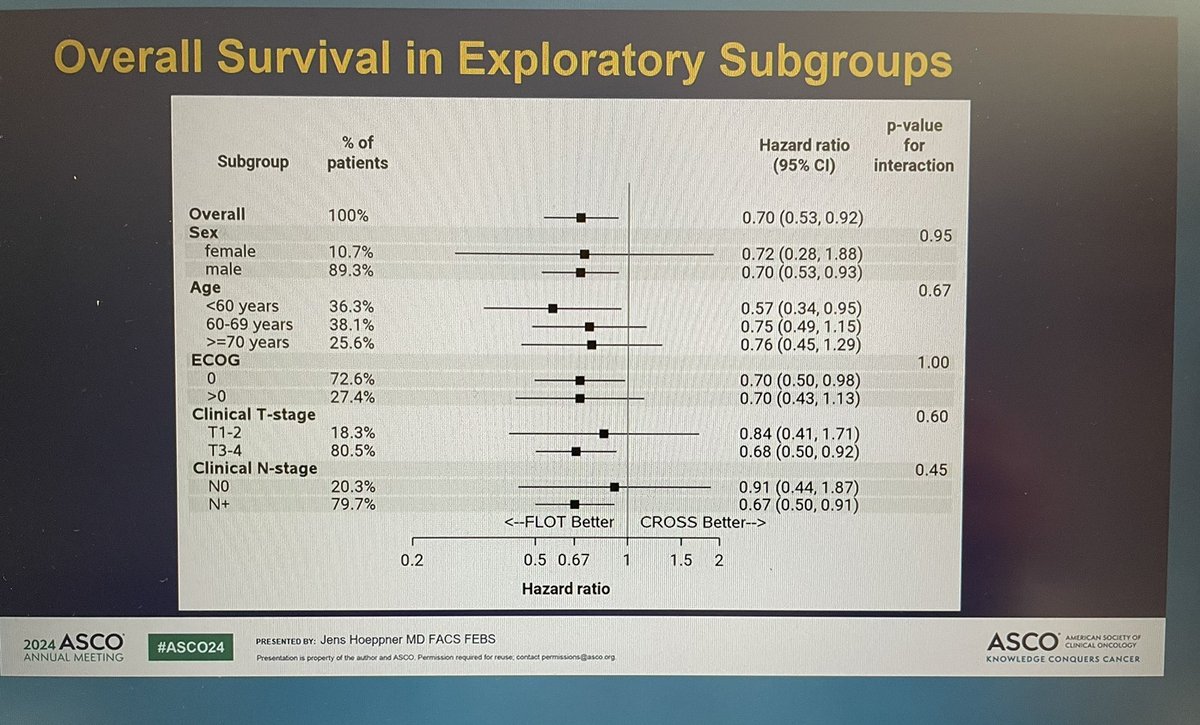
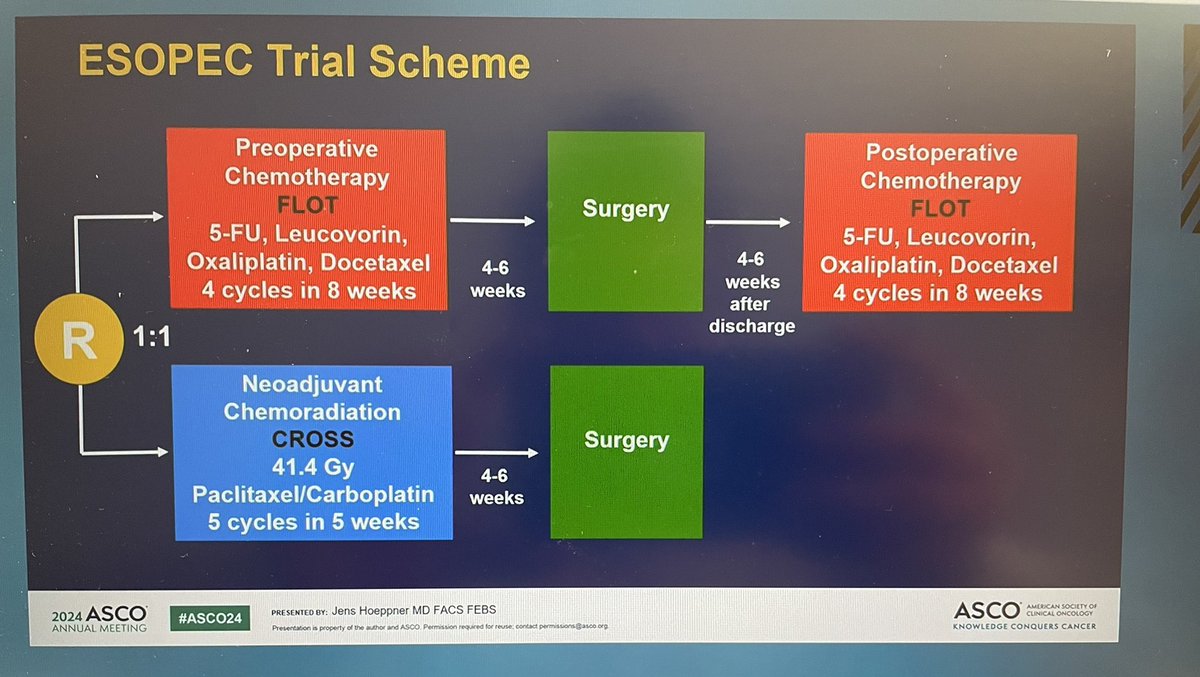
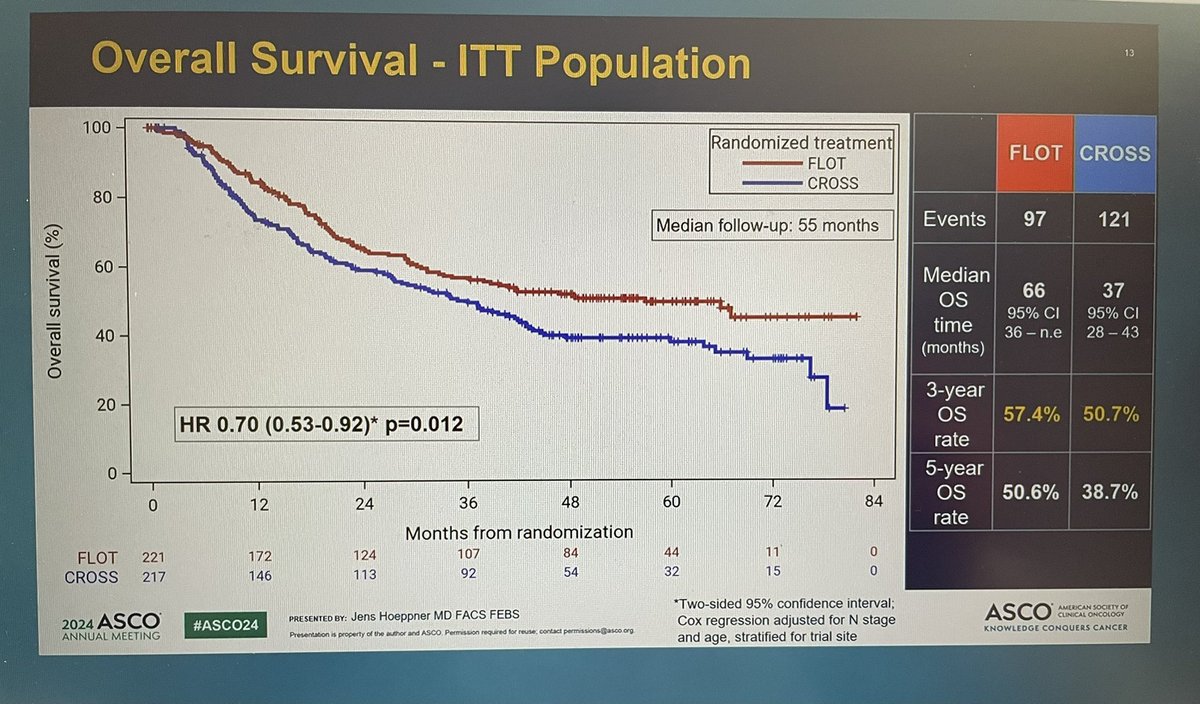
Dr. Hoeppner ESOPEC PhIII trial (cT1cN+ or cT2-4acN0/+) esoph adenoCA rand 1:1 periop #FLOT vs neoadj #CROSS ➡️ FLOT superior w/median OS 66 mos vs 37 mos, PFS, & higher pCR (16.8 vs 10%) over CROSS. 52.5% finished adj FLOT, 67.7% finished neoadj CROSS
#ASCO24@OncoAlert
Good q. If decision is for pre-op therapy for T2N0, I’d favor CROSS due to lower treatment burden, cost, & toxicity for most (obviously exact tradeoffs depend on specific scenario).
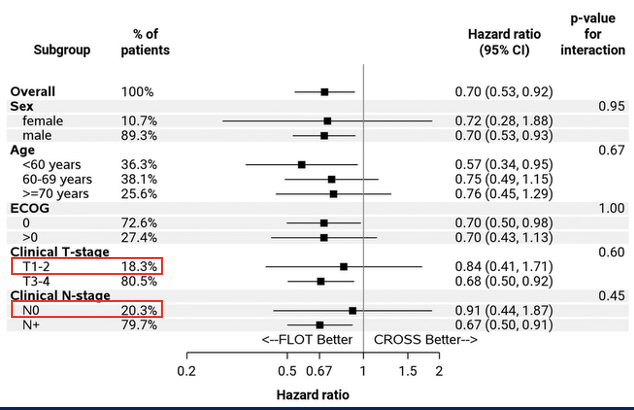
Per ESOPEC forest plot, FLOT ~ CROSS for T2 or N0. Can then add on adjuvant nivo per CM577.
A new publication from @BrendanHeiden et al demonstrates an OS benefit for patients with stage I NSCLC undergoing surgery at VA medical centers with on-site SBRT. The results show that SBRT is being appropriately leveraged to optimize patient selection when available. These data provide further evidence that MDT matters. @ZaidAbdelsattar@kelleymic https://t.co/w0NUG3QILz
@lymberis I am a doctor from Vietnam. Information on induction treatment for cervical cancer is truly important for us. Could you please share the discussion with me?
A well known thoracic rad onc refused to accept 60Gy/30fx concurrent chemoRT for LS-SCLC as an acceptable treatment regimen on the boards, despite it being the most commonly prescribed fractionation in the US (maybe world?)
I will shoot him dirty looks at ASTRO until he apologizes.
https://t.co/vR0pxai1L6
https://t.co/eLnqdYSw6l
@toddscarbrough@cpeedell@JoeChangMD How common is 60/30? In my training and at Mayo now we always give at least 66 if we’re doing daily fractions? I agree with both of you — not sure 3 extra fractions makes a difference and adopting daily fractionation in any case is massaging data for convenience…