Time to revisit something I’ve been saying for years: TaHG bladder cancer is not intermediate risk. The clinical outcomes, molecular biology ... all point in the same direction.
Yet some frameworks allow < 3cm TaHG tumors to be downgraded into “intermediate risk” alongside low-grade disease.
That classification has real consequences for patients:
• undertreatment
• less rigorous surveillance
• in some studies, these patients are even placed on observation as a supposedly appropriate “control arm.”
TaHG is high risk. 🧵 @BladderCancerUS@WorldBladderCan@IBCG_BladderCA
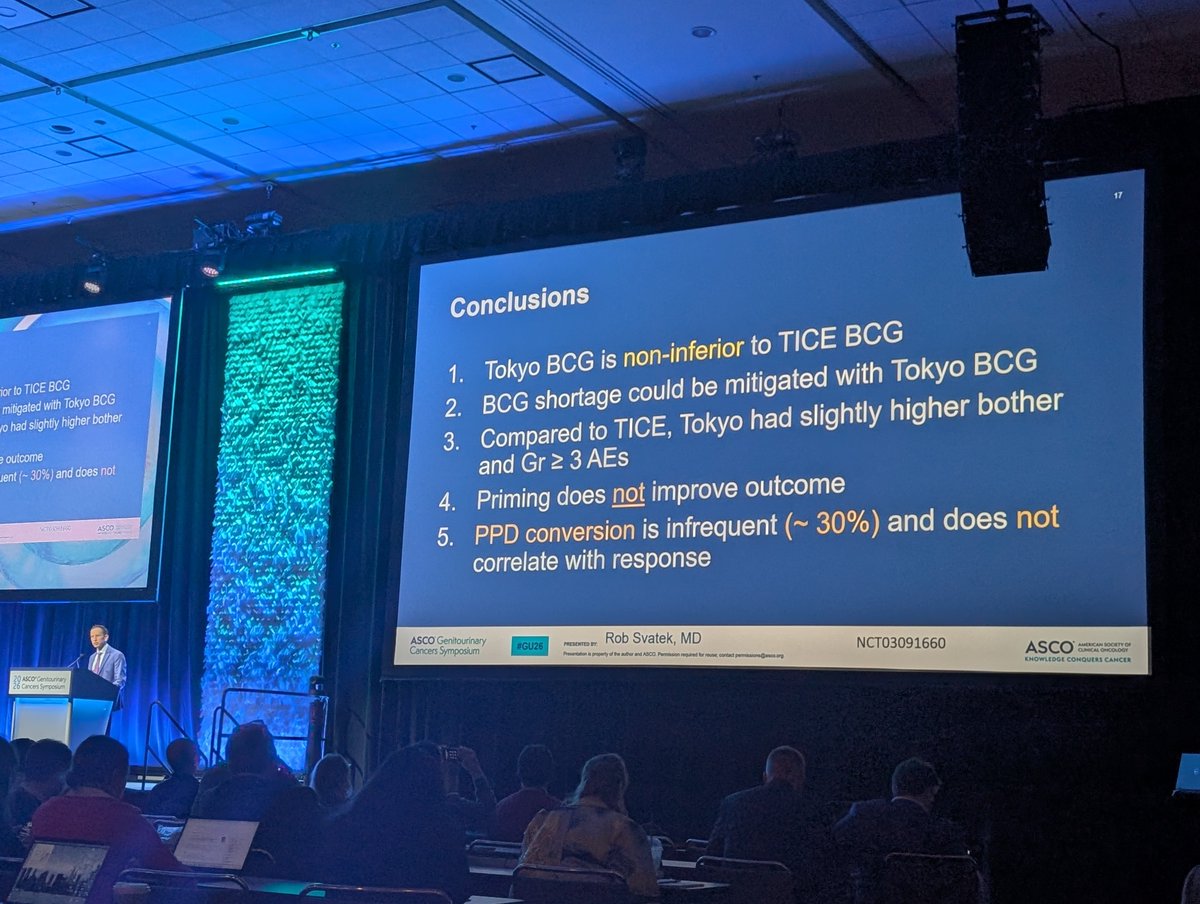
A common concern: reduced dose BCG = inferior outcomes.
The data do not support that. Across RCTs and real-world series, 1/3 dose BCG achieves comparable recurrence, progression, and survival outcomes.
Why? BCG is not a fixed-dose drug. Each vial has up to 10-fold variability in viable organisms (CFUs). "Dose" on paper does not reflect true biologic exposure. 🔬
"Full dose" from a low-CFU vial can deliver less BCG than "reduced dose" from a high-CFU vial.
#BladderCancer
BREAKING:
Scientists gave healthy older adults a transplant drug once a week.
Their immune systems got younger.
Their flu vaccine worked 20% better.
Side effects? Nearly zero.
This is the most exciting anti-aging drug in human history.
Here's what the clinical trials actually show 🧵
So exciting that this is now in the NCCN guidelines!
No doubt that this will better stratify IR NMIBC patients for clinical trials.
Grateful to @UroDocAsh and the @IBCG_BladderCA team for the opportunity to lead this work
https://t.co/X1QvHxC9HV
FGFR3 targeted therapy is going though a renaissance with blood based biomarkers, new agents such a Vepugratinib and novel delivery methods (moonrise program) @giannatempopatr@OncoAlert#GUtrendingtopics
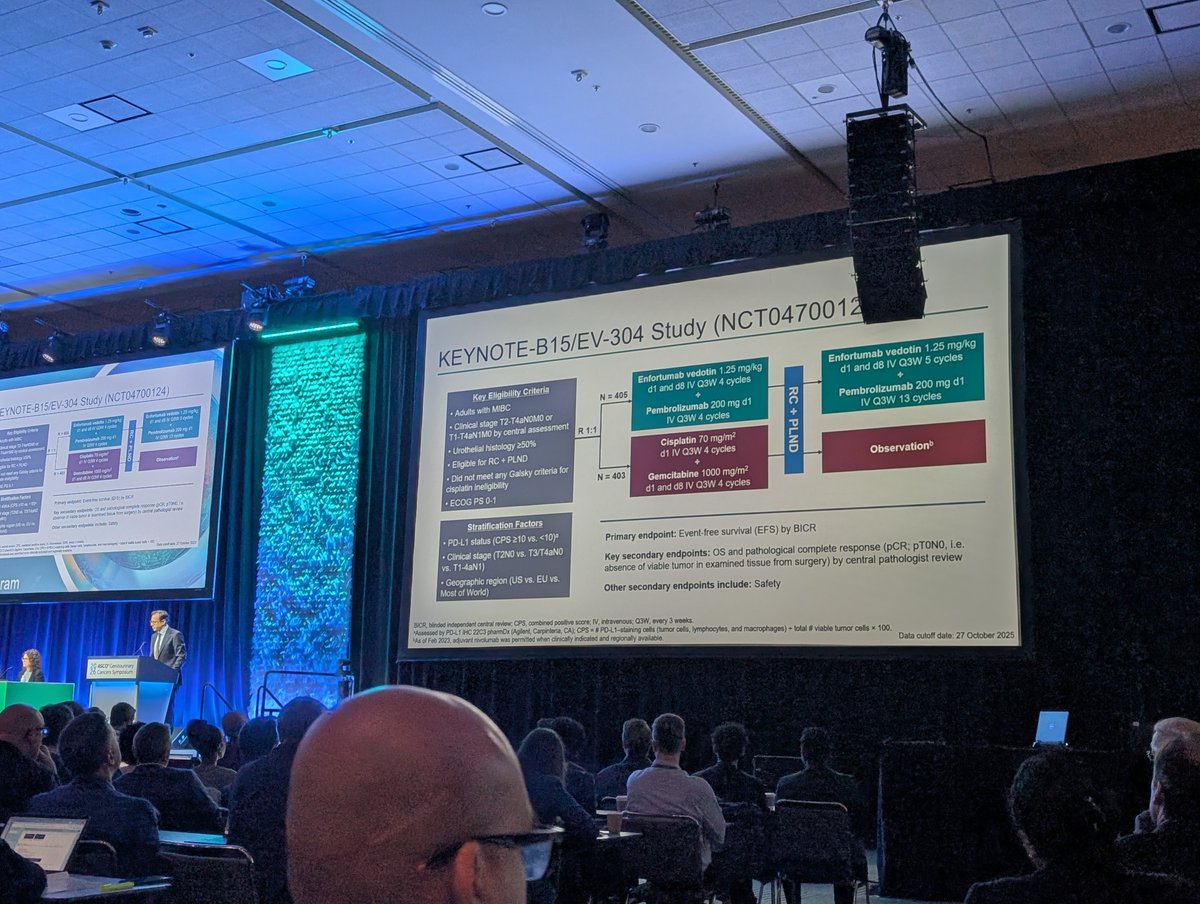
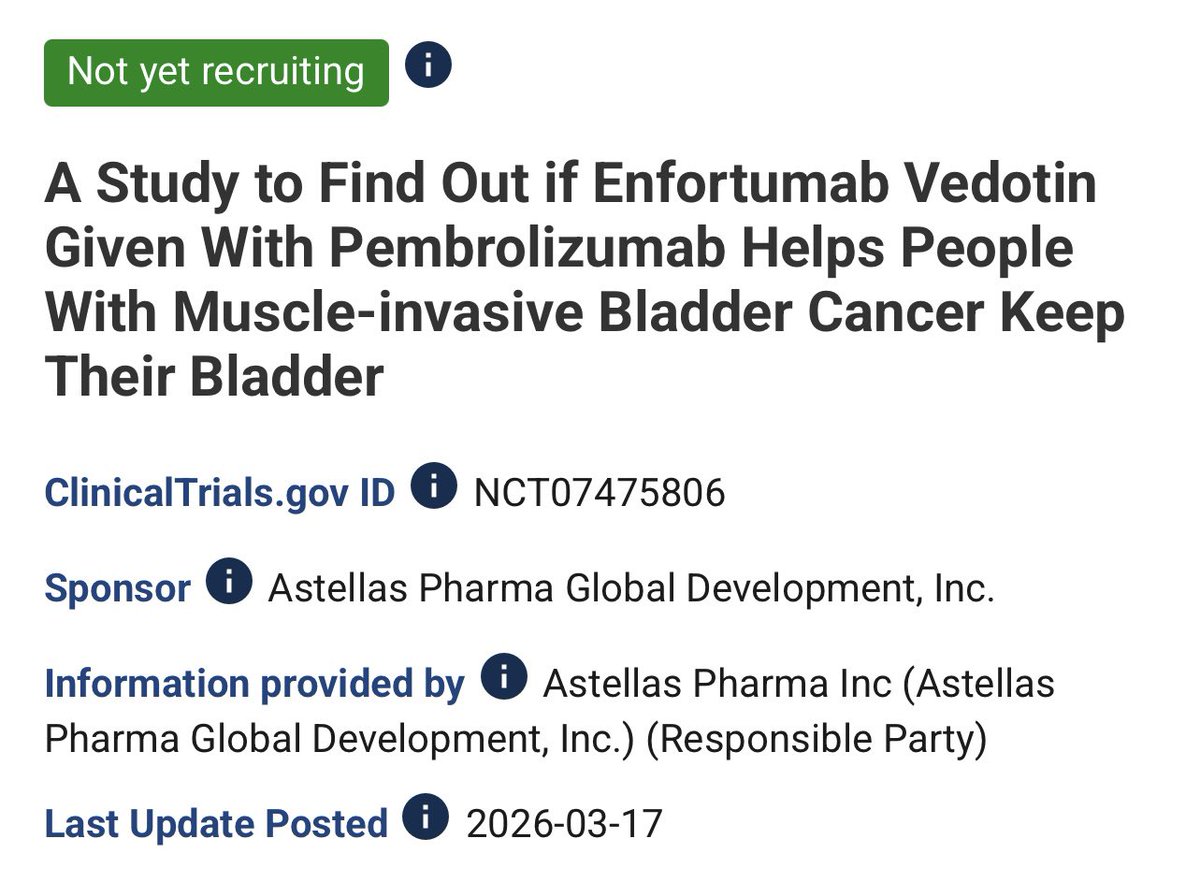
A 240 pateint single arm trial exploring 9 cycles of EVP without planned surgery in MIBC. This will answer the key questions ‘What happens if we don’t do cystectomy in those with clinical complete response after initial EVP’.It assesses cCR rates and bladder intact EFS. It will clarify ‘EVP 1st ask questions later’ #GUtrendingTopics @OncoAlert
#ASCOGU26
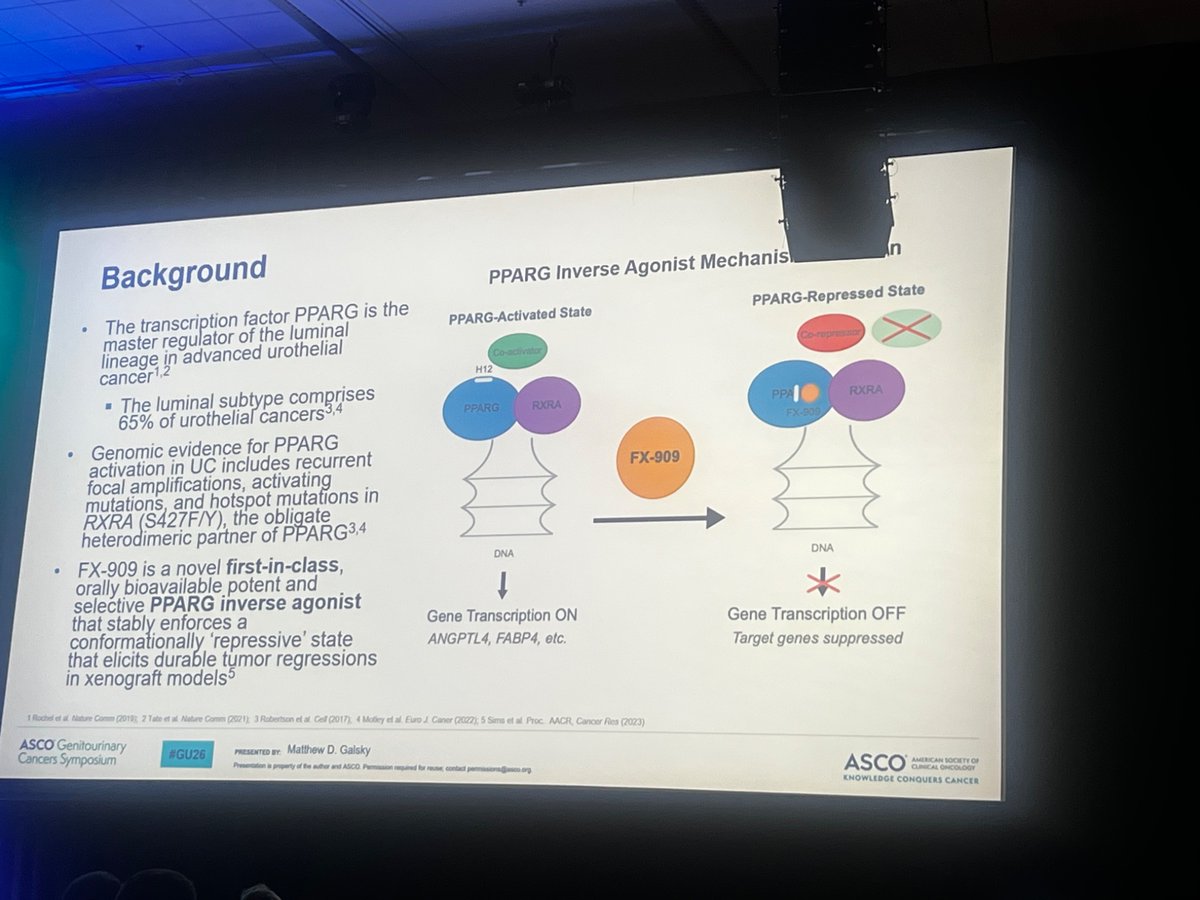
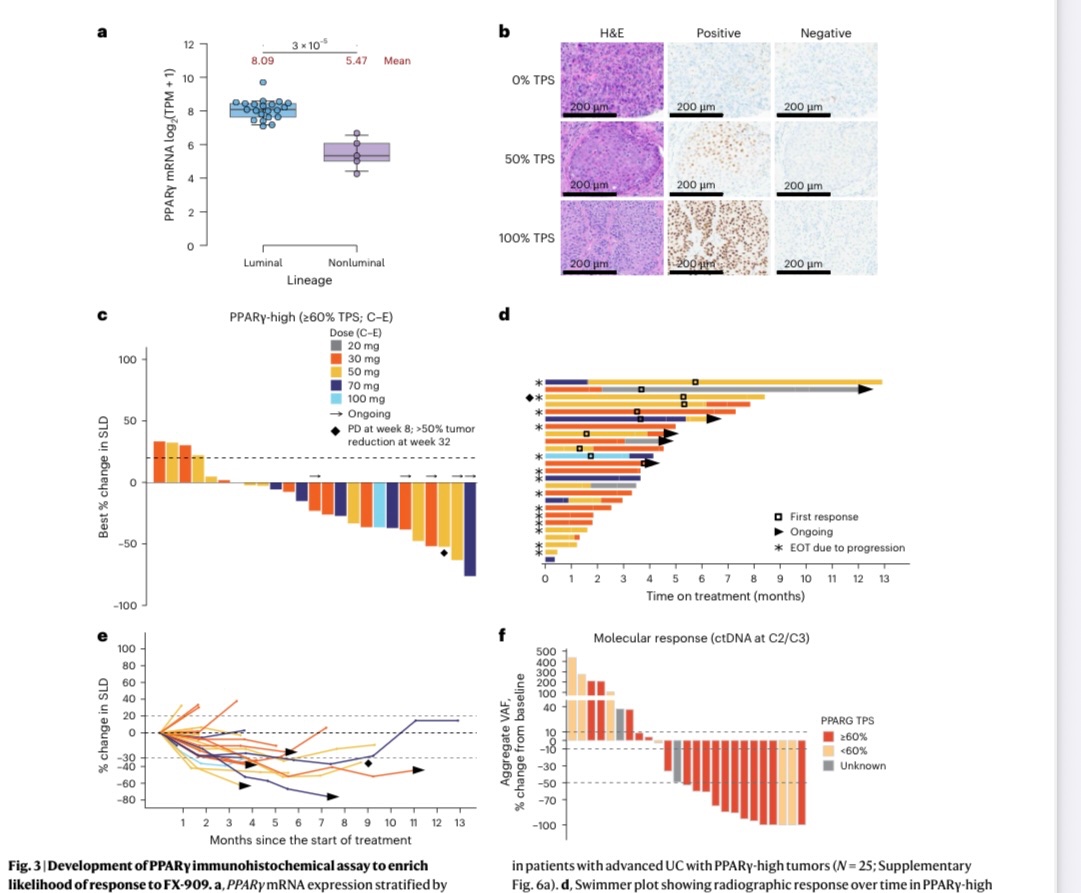
Congrats @MattGalsky on leading this novel ph 1 trial of FX-909, a 1st in class oral PPARγ inverse agonist in solid tumors including mUC.
PPARγ is a master regulator of luminal lineage & its activation drives tumorogenesis.
FX-909 shows promising efficacy in IHC selected tumors.
Key TRAEs anemia, hyperglycemia, fatigue. thrombocytopenia.
Provides rationale for dose expansion and combo studies.
Glad to be a part of this novel work.
@CleClinicMD
https://t.co/LZBXU2VK9Z
Nice progress on drugging p53. It’s true that we need to find new targets, but it’s also important to keep expanding the druggable universe with better technologies.
Lots of great targets we already know about that are just waiting for the right molecule
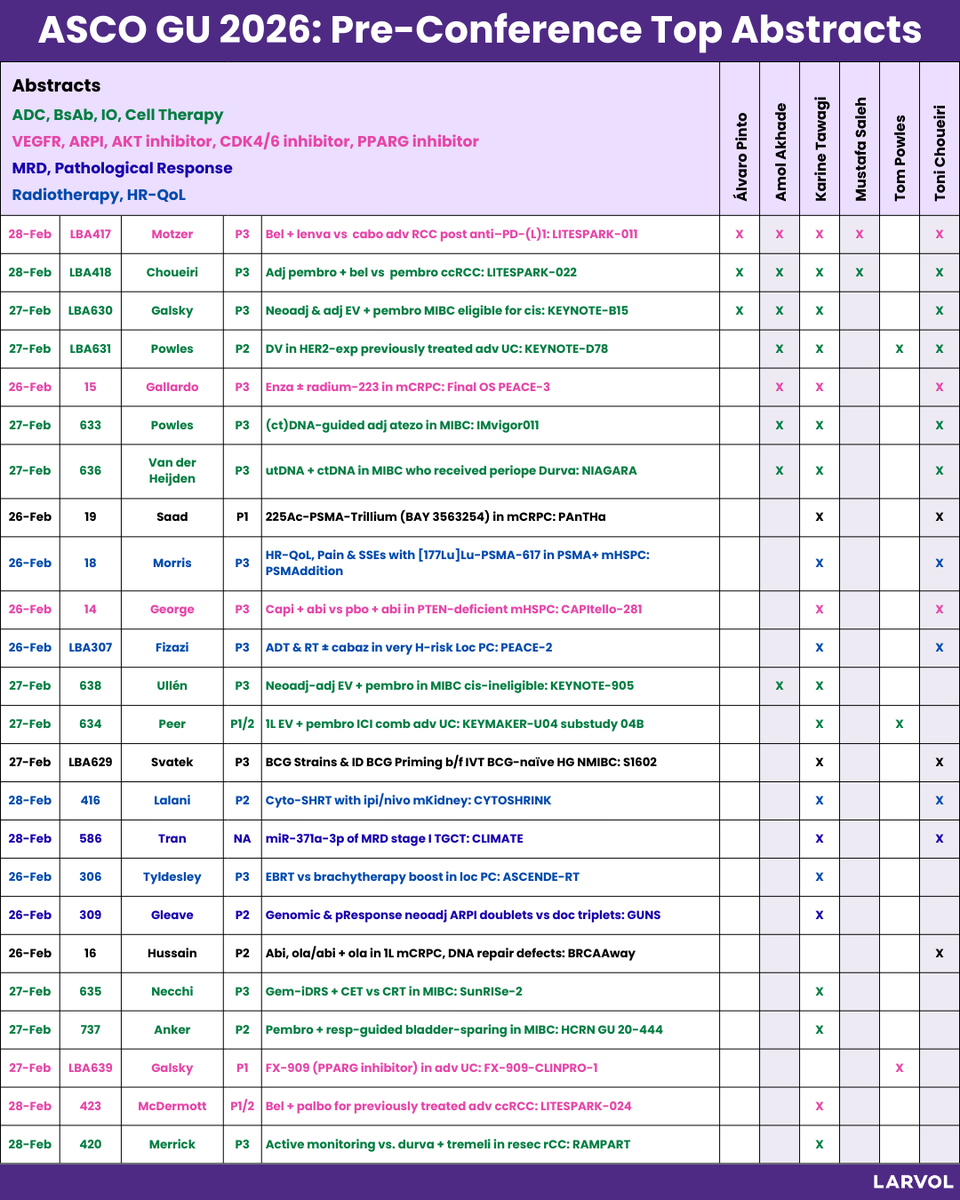
With ASCO GU 2026 upon us, oncologists are already weighing in, sharing, and debating the most anticipated genitourinary oncology abstracts ahead of the meeting.
We’re tracking these conversations in real time and analyzing what’s gaining traction across the community. Here are the pre-conference Top abstracts for ASCO GU 2026.
Special thanks to Dr. Mike Thompson (@mtmdphd) for the original idea.
Which abstract are you watching at American Society of Clinical Oncology (@ASCO) Genitourinary Cancers Symposium 2026?
Explore more insights and data from #GU26: https://t.co/hJxifSvzwe
#LARVOL #ASCOGU26 #CancerResearch #CancerData #Oncology #OncologyInsights #GUCancer #GenitourinaryCancer #GUCSM
Discussion threads:
Dr. Álvaro Pinto (@dralvaropinto): https://t.co/QzcyAcXVNc
Dr. Amol Akhade (@SuyogCancer): https://t.co/wpcQH6ZSVs
Dr. Karine Tawagi (@DrKarineTawagi): https://t.co/TEhBOdZhGQ
Dr. Mustafa J. Saleh (@Mustafajsalehmd): https://t.co/Y82NahkRkO
Dr. Tom Powles (@tompowles1): https://t.co/F1r3vN8U1i
Dr. Toni Choueiri (@DrChoueiri): https://t.co/opgp6JAJoL