Following breakthrough results, we’re bringing longevity medicine to human trials.
We’ve raised a $435M Series C led by @foundersfund to make it happen.
Reprogramming cell age has the potential to create more healthy years for everyone. We're closer than ever to realizing it.
$ABVX As a follow-up to a few posts that I saw regarding the perceived elevated rates of NMSC and malignancies in the 50 mg arm specifically in the phase 3:
A few thoughts:
1) The phase 3 50 mg dose is actually a small minority of the patient years of safety data acquired -- the much larger dataset for that dose comes from the phase 2b long-term open label follow-up, which can be reasonably pooled with the phase 3 results given the same dose and detection protocols (Note, we have seen some analyses that pool 25 mg and 50 mg arms. We would NOT recommend doing this as it is not fair to claim that the risk of developing cancer in the 25 mg arm is known to be the same as the 50 mg arm). Pooling 50 mg phase 2b and 50 mg phase 3 data sets yields a much lower rate of events across the board. (I suspect it was just a bit of bad luck on the smaller phase 3 dataset for the 50 mg dose in isolation, see below chart for what we've been working off of after integrating these phase 2 data -- note there are some assumptions that go into this but the variability should be pretty de minimis);
2) Two ways things generally cause cancer: DNA damage from some oxidative/radiation/something else source that damages DNA or inhibits DNA repair mechanisms at their core OR substantial or highly targeted immunosuppression. Because both of these events are total exposure related, typically events accelerate over time. The phase 2 had the much longer follow-up with fewer patients whereas the phase 3 had more patients followed up for less time. The phase 2 had a very low number of events, and the phase 3 50mg dose was the only arm that had an elevated set. A priori, if the drug was a carcinogen, we would have expected the opposite: that the phase 2 would have a higher incidence/100 PY than the phase 3 given the individual patient exposures on a cumulative basis to such carcinogens are much higher in the phase 2 than the phase 3 in addition to the idea that there is a delay between when the carcinogen can cause the malignancy to when it can be detected (and T=0 is always the first instance in which that timer could start). Also, if the drug was as immunosuppressive as would be needed to cause cancer, you would expect to see a boatload of opportunistic infection before you'd see the cancer signal -- we see none.;
3) Pre-clinical testing confirmed that the drug is actually an anti-proliferative -- we would have expected the drug to be protective against tumor growth, not stimulating it;
4) No consistency or clustering for any cancer type at any time point;
5) NMSC carries a much different (lower) risk profile than other types of malignancies since they are caught very easily and have a low rate of metastases, and are seen at a massively disproportionately high case numbers relative to other types of malignancies (also included in the bottom table following pooling of the 50 mg arm), so FDA is less concerned about it than non-NMSC;
6) To warrant a black box, the FDA usually requires, at a minimum, consistency of preclinical and/or striking clinical datapoints such that careful consideration must be made to determine if the benefit/risk profile inverts in a subset of all patients that may receive the drug. In this case, we not only have completely disparate and conflicting datapoints, but we even have one data point relating to the MoA and pre-clinical data findings that suggest the drug should have the opposite effect. In addition, black box decisions are not made in isolation. They are heavily debated back and forth between the company, internally, require a lot of internal consensus on establishing causal link, and are not made in a vacuum to unmet need and efficacy;
7) UC patients have an elevated rate of inflammation (by definition) and, in turn, elevated rates of cancer compared to healthy individuals (~+.5 events/100PY vs non-UC). Obefazimod is now a proven highly effective therapy that leads to robust endoscopic remissions and attenuation of much of this inflammatory effect. I would hypothesize if you ran a large enough study and followed patients for long enough, you would find that there would be a cancer benefit from the drug secondary to the disease control that it would afford. The weight of this potential benefit (which makes sense given the pathophysiology) must be considered against the risk of the agent itself causing cancer (for which we have no reason to believe it actually should cause cancer).
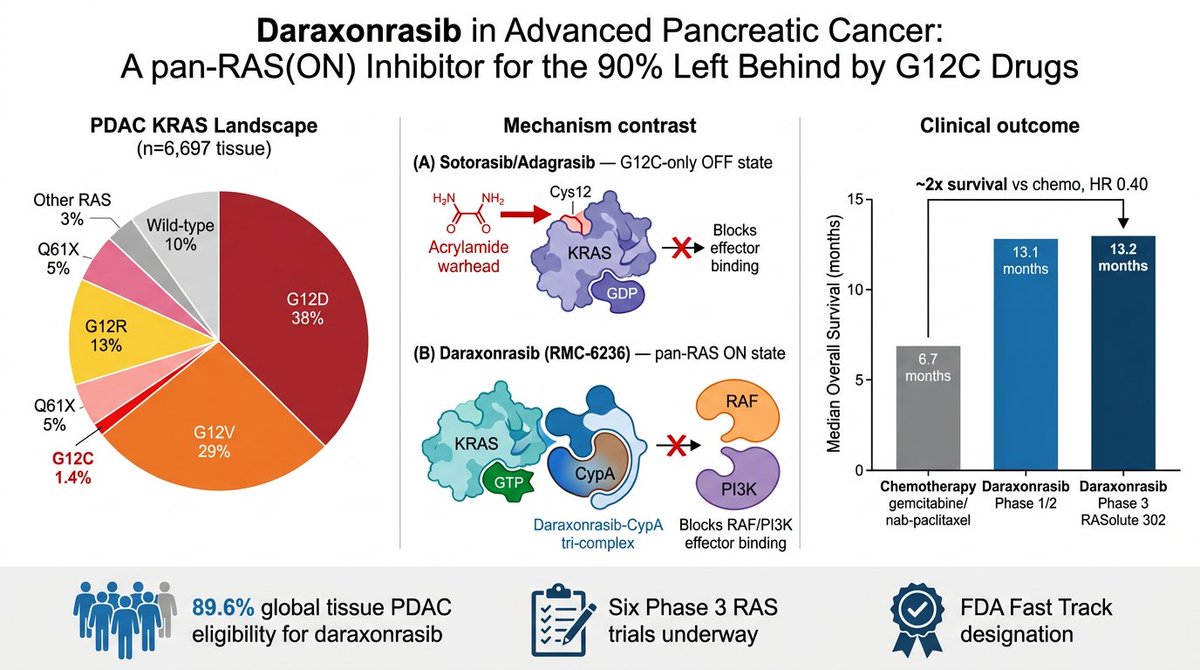
RAS finally getting drugged is one of the great stories in modern biology, and almost nobody outside oncology understands why it's such a big deal.
YOU'LL LEARN SOMETHING AWESOME TODAY.
i am going to keep this as understandable (and simple) as i can.
OPEN THE THREAD.
🧵
Personal update: I've joined Anthropic. I think the next few years at the frontier of LLMs will be especially formative. I am very excited to join the team here and get back to R&D. I remain deeply passionate about education and plan to resume my work on it in time.
The choice of words in the latest @stratechery post is just stellar:
“I don’t know what the future will bring, but I do know it will not only be different from today, but definitely different from a linear projection of AI capabilities mapped onto an ossified and simplistic model of the world that bears little resemblance to not just the incredible depth and texture of reality, but also the remarkable adaptability of humanity and the power of markets”
9/ When you look at filings of money managers, many own the same stocks but end the year very differently. Why? Not everyone knows what to do when things go wrong. And that’s when major alpha can get created or destroyed.
My latest piece on the evolution of the US-China relationship. Nothing in there that I have not said in podcasts, and written in various reports, over the years. Including the jokes. But it’s a quick read…
Anyway, this piece is unlocked. Constructive feedback welcomed…
https://t.co/eJ7EDOb9BH
It's been a long time since I posted a single piece with all my predictions on energy, so I made an update.
https://t.co/2hDLQOEcPc
Here's some free alpha for you all.
Technological innovation can be a form of participation in the divine act of creation. It carries an ethical and spiritual weight, for every design choice expresses a vision of humanity. The Church therefore calls all builders of #AI to cultivate moral discernment as a fundamental part of their work—to develop systems that reflect justice, solidarity, and a genuine reverence for life.
Death by a 1000 paper cuts. For nearly 20yrs I still struggle with this. I don’t have some BS cliche for you. It sucks, it pisses me off that I still struggle with it and there you go. Don’t know what else to say.
'The takeaway is that you should be careful about drawing conclusions from large option trades unless you have direct context on the flow. Without that color, it is easy to mistake logistics for signals.'
@therobotjames@mistman78 @darjohn25 @Gingfacekillah @emfxoptions "See that number? That's the bund. It has got some shit to do with Germany but all you need to know is it goes up and down and other cunts trade it"
Jamie. Life. 1995
Blast from the past. I wrote this piece more than 15Y ago in the forum. Still holds true today & always will of course. After interacting w/countless aspiring traders over decades it continues to be one of the toughest mandatory shifts in thinking for most to accept & overcome.🎲
Smth that has been helpful to me is the conceptualisation of growth as 'random leaps' or 'random inflections'. You hit your head against the wall FOREVER and eventually you break through and FOOM.