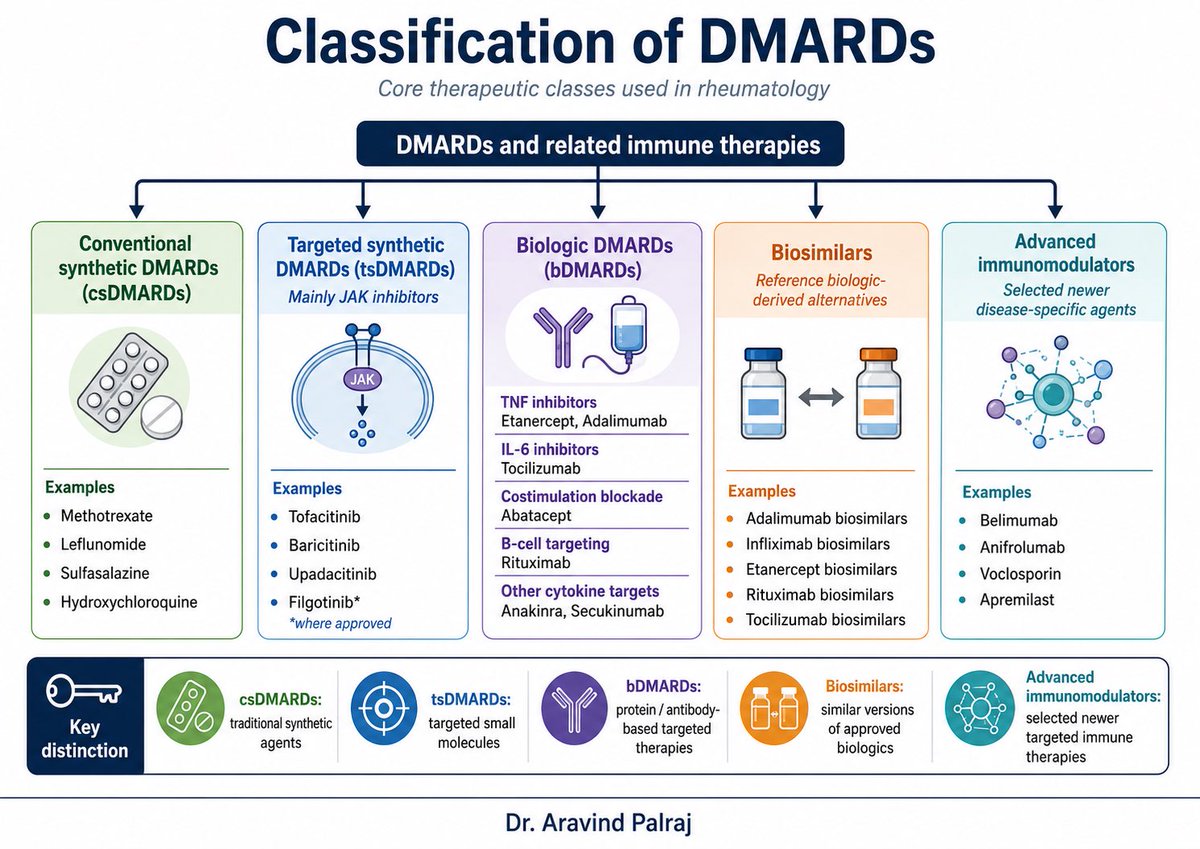
DMARDs are the backbone of modern rheumatology treatment.
They include conventional synthetic DMARDs, targeted synthetic DMARDs, biologic DMARDs, biosimilars, and newer disease-specific immunomodulators.
Knowing the class helps us understand the mechanism, monitoring needs, safety issues, and treatment sequencing.
Right drug. Right patient. Right disease phenotype.
Dr. Aravind Palraj
#Rheumatology #DMARDs #MedicalEducation #AutoimmuneDisease #ClinicalImmunology @IhabFathiSulima@docakx
ESR tells you that inflammation has left a slow systemic footprint.
CRP tells you that the liver is actively responding to cytokines
Procalcitonin tells you that the inflammatory programme may be bacterial or septic in nature.
They are not interchangeable clocks.
They are different biological readouts.
📚🩺💡 New #LFNguidelines review! @BlaneyMD
Key highlights:
🔹 Diagnosis and evaluation of ascites
🔹 Prevention and management of SBP
🔹 Recognition and treatment of HRS
🔹 Practical, guideline-based clinical pearls
Read here ⬇️
🔗 https://t.co/yvO7PEh4EB
ANCA Vasculitis made simple 🔥
🔹 GPA → ENT + lung nodules + c-ANCA(PR3)
🔹 MPA → renal + pulmonary capillaritis + p-ANCA(MPO)
🔹 EGPA → asthma + eosinophilia + neuropathy
One of the highest-yield topics in rheumatology & medicine.
Which pattern do you find hardest to remember?
#Rheumatology #Vasculitis @docakx@IhabFathiSulima #MedTwitter #InternalMedicine #Nephrology
🔬 Significance of Serum Free Light Chain (SFLC) in Multiple Myeloma
My latest comprehensive infographic on this key biomarker that has transformed diagnosis, prognosis, renal monitoring & treatment decisions in MM.
Covers everything in one visual: ✅ Basic concept & what SFLC actually measures
✅ Normal ranges + κ/λ ratio
✅ IMWG myeloma-defining event (involved/uninvolved SFLC ratio ≥100)
✅ Light-chain, oligosecretory & non-secretory myeloma + AL amyloidosis
✅ Risk stratification & prognostic implications
✅ Myeloma cast nephropathy & renal failure
✅ Rapid treatment monitoring (half-life 2–6 hrs!)
✅ Early relapse detection & practical clinical pearls
Save 📌 this as your quick reference guide!
Cancer Concepts Explained by Dr Rupam Manna
Follow for more → @DrRupamOncology
#MultipleMyeloma #SFLC #Myeloma #Oncology #HemOnc #MedEd #MedTwitter #Hematology
You know APS is antibody-mediated.
We test anti-β2GPI.
We test anticardiolipin.
We test lupus anticoagulant.
In pregnancy, we give heparin.
But lupus anticoagulant isn’t a single antibody.
And heparin isn’t just a blood thinner.
Yet both revolve around one molecule: β2GPI.
Let me explain.🧵👇
1-APS is NOT truly about phospholipids
Despite the name “antiphospholipid,”
the main pathogenic target is β2-glycoprotein I (β2GPI) -a phospholipid-binding protein.
Cardiolipin is the surface.
β2GPI is the antigen.
2-What is lupus anticoagulant (LA)?
LA is not a specific antibody.
It is a functional laboratory phenomenon:
An antibody that prolongs phospholipid-dependent clotting assays (like dRVVT or aPTT) and corrects with excess phospholipid.
3-Why does LA prolong clotting in vitro?
Clotting assays require phospholipid surfaces.
In many APS patients:
• β2GPI binds phospholipid
• Anti-β2GPI antibodies bind β2GPI
• This interferes with coagulation complex assembly
→ Clotting time prolongs.
That’s why it’s called “anticoagulant.”
4-But not all LA is anti-β2GPI
Important nuance:
Some LA activity is prothrombin-dependent (e.g., aPS/PT antibodies).
So LA is heterogeneous.
But in high-risk APS (especially triple positive patients),
LA is often β2GPI-dependent — and strongly associated with thrombosis.
5-Now shift to obstetric APS
Pregnancy loss in APS is not just thrombosis.
Placental studies and animal models show:
• Complement activation
• Trophoblast injury
• Impaired placental remodeling
Sometimes with minimal thrombosis.
This is immune-mediated placental dysfunction.
6-β2GPI at the maternal–fetal interface
β2GPI binds trophoblast membranes.
Anti-β2GPI antibodies:
• Inhibit trophoblast invasion
• Increase apoptosis
• Trigger complement cascade
The placenta becomes the target.
7-So why does heparin help?
If pregnancy loss were purely thrombotic,
aspirin alone should be enough.
But aspirin + heparin improves live birth rates.
Because heparin does more than anticoagulation..
8-Heparin disrupts β2GPI biology
Heparin binds a heparin-binding region in domain V of β2GPI.
This can:
• Reduce β2GPI binding to phospholipids
• Interfere with antibody clustering
• Promote β2GPI inactivation in some settings
9-Complement may be the key
Animal models show:
Block complement → prevent aPL-mediated fetal loss.
Heparin reduces complement activation at the placenta.
This may be central to its benefit in obstetric APS.
10- The concept
APS revolves around β2GPI.
Lupus anticoagulant is a functional manifestation, often reflecting antibodies that disrupt phospholipid surfaces (frequently β2GPI-dependent, but not always).
And in pregnancy:
Heparin works not only by preventing clots..
but by modulating β2GPI interactions and complement activation.
Same axis.
Different angles.
One central protein.
β2GPI.
#Rheumatology #APS #ObstetricAPS #Lupus #Immunology @DrAkhilX @IhabFathiSulima
7 ideas about mycophenolate that every rheumatologist should know.👇
Concept 1: What we prescribe is not the active drug
We prescribe MMF
MMF → (in stomach) → MPA (active drug)
Only MPA suppresses immunity.
If this step is inefficient → drug effect falls.
Concept 2: Stomach acid decides how much drug works
Low gastric pH (acidic stomach)
→ MMF dissolves properly
→ more MPA enters blood
High gastric pH
→ MMF dissolves poorly
→ less MPA absorbed
This step happens before we ever think of doses.
Concept 3: Why PPIs quietly reduce MMF effect
PPI
→ raises gastric pH
→ MMF does not dissolve well
→ ↓ MPA exposure by ~25–30%
Dose unchanged.
Patient compliant.
But effective drug level is lower.
Concept 4: Formulation changes the entire pathway
MMF
→ dissolves in stomach
→ highly pH dependent
EC-MPS
→ bypasses stomach
→ releases in intestine
→ much less affected by PPIs
Same drug. Different route. Different outcome.
Concept 5: Mycophenolate has a “second absorption”
After first absorption:
MPA → liver → MPAG
MPAG → bile → gut
Gut bacteria → MPAG back to MPA
MPA → reabsorbed
This loop
→ creates a second peak
→ contributes 30–40% of total drug exposure
This is not a minor effect.
Concept 6: Kidney disease and albumin change lab numbers
MPA is 97–99% bound to albumin
Renal failure or low albumin
→ less protein binding
→ ↓ total MPA level
But
→ free (active) MPA may be unchanged
So low numbers do not always mean low efficacy.
Concept 7: The gut has silent thieves
Sevelamer
→ binds MPA in gut
→ −25–35% exposure
Laxatives
→ speed transit / bind drug
→ −50% or more
Iron supplements
→ chelate MPA
→ up to −90% absorption
These are common, overlooked causes of failure.
Clinical moment: patient flares on MMF
Before increasing dose → pause and ask:
➡ On a PPI?
➡ MMF or EC-MPS?
➡ Taking sevelamer, iron, laxatives?
➡ Low albumin? Renal impairment?
Often, the answer is here.
Final teaching pearl
Mycophenolate works well
when the stomach, gut, liver, kidney, and proteins cooperate.
If any step is disturbed → drug exposure quietly falls.
Understand the journey,
and mycophenolate becomes predictable.
#Rheumatology #MedTwitter #Mycophenolate #ClinicalPharmacology #MedEd #RheumPearls #Immunosuppression @DrAkhilX @IhabFathiSulima@CelestinoGutirr@nileshnolkha
This young girl's quest for a diagnosis ended today. She came to us after a 2.5 year ordeal in different places.
🌟This 23 year old 👩🚒bariatric Surgery (Sleeve Gastrectomy) in October 2022 after which her weight ⬇️⬇️ from 120 kg to 72 kg in 8 months.
🌟Experienced GERD and was bedbound for 6 months. She developed emotional disturbances requiring Qutipin.
🌟2 months later, she developed progressive weakness in hands (2 months).
🌟o/e weakness in distal hand muscles (extensors > flexors). Brisk DTRs, flexor plantar response, normal sensory function.
🌟NCS showed a generalized motor CMAP reduction, predominantly affecting radial nerves.
🌟She was diagnosed with a unclear myeloneuropathy vs. Progressive Motor Neuropathy post-bariatric surgery.
🌟MRI Spine: normal. Holo vitamin panel normal, except high Pantothenic Acid.
🌟Creatinine 1.6 (Medical Renal Disease - ? etiology).
CRP -a story we all live daily (but rarely understand)
Today I asked my student:
“What is CRP? What is its normal function?”
He said confidently: “Sir, it’s an acute-phase reactant. It increases in infection.”
Then I asked:
“What do you mean by acute-phase reactant?”
He paused… thinking… stuck.
And honestly-most of us would also pause if we had to explain it properly.
Because we order CRP every day to “see inflammation”…
…but many of us don’t know CRP’s real identity.
So let’s see. 👇
First: why the name C-reactive?
Because CRP was discovered as a serum factor that reacted with the “C-polysaccharide” of pneumococcus during acute infection.
Second: what is CRP, conceptually?
CRP is a pattern recognition receptor (PRR)—but unlike TLR/CLR (membrane) or RLR (cytosolic)…
👉 CRP is a soluble, secreted PRR that patrols from the bloodstream.
What does this “soluble PRR” recognize?
Signals of danger: microbes + damaged self.
CRP binds targets like phosphorylcholine on microbes and on apoptotic/necrotic membranes—basically, “this needs cleanup.”
Then CRP does the work:
🧹 Opsonization (tags for phagocytosis)
🧩 Classical complement activation (via C1q)
➡️ Better clearance of debris & immune complexes.
Now the clinical beauty: CRP kinetics.
CRP is made fast—rises by ~6 hours, peaks around ~48 hours after a stimulus.
The golden fact most people miss:
CRP has a constant half-life ~19 hours (in health and disease).
So the CRP value mainly reflects how much the liver is producing, i.e., inflammatory drive.
So when should you repeat CRP?
If you want the repeat to mean something, match biology:
✅ Repeat in 24–48 hours to judge trend/response (rise/peak/fall dynamics).
When is repeating too early?
<12 hours usually adds noise, not insight—CRP hasn’t had time to change meaningfully given its kinetics and half-life.
CRP isn’t just “an acute phase reactant.”
It’s a secreted PRR + complement-linking opsonin + a real-time reporter of inflammatory production.
We order it daily.
It’s worth knowing what it really does.
👉 #MedTwitter #RheumTwitter #Immunology #CRP #ClinicalPearls #MedEd @DrAkhilX @IhabFathiSulima@CelestinoGutirr@Urchilla01@schowardjd
Here is an app that I’ve created for cognitive testing. It’s freely available and collates most of the commonly used bedside tests in Neurology/Neurosurgery. Let me know if anyone has any suggestions, recommendations or questions!
https://t.co/LUXX8sBVxs
🧵 1️⃣ Inpatient Hyperglycemia
25% of hospitalized patients have diabetes.
But even non-diabetics with hyperglycemia face worse outcomes — higher infection rates, longer stays, more readmissions, and higher mortality.
Hyperglycemia isn’t just a number. It’s a prognostic marker and a modifiable target.
Let’s break it down 👇
#MedTwitter #Endocrinology
@DrAkhilX @prarit_v@Doctors__squad@DoctorLFC@drkeithsiau
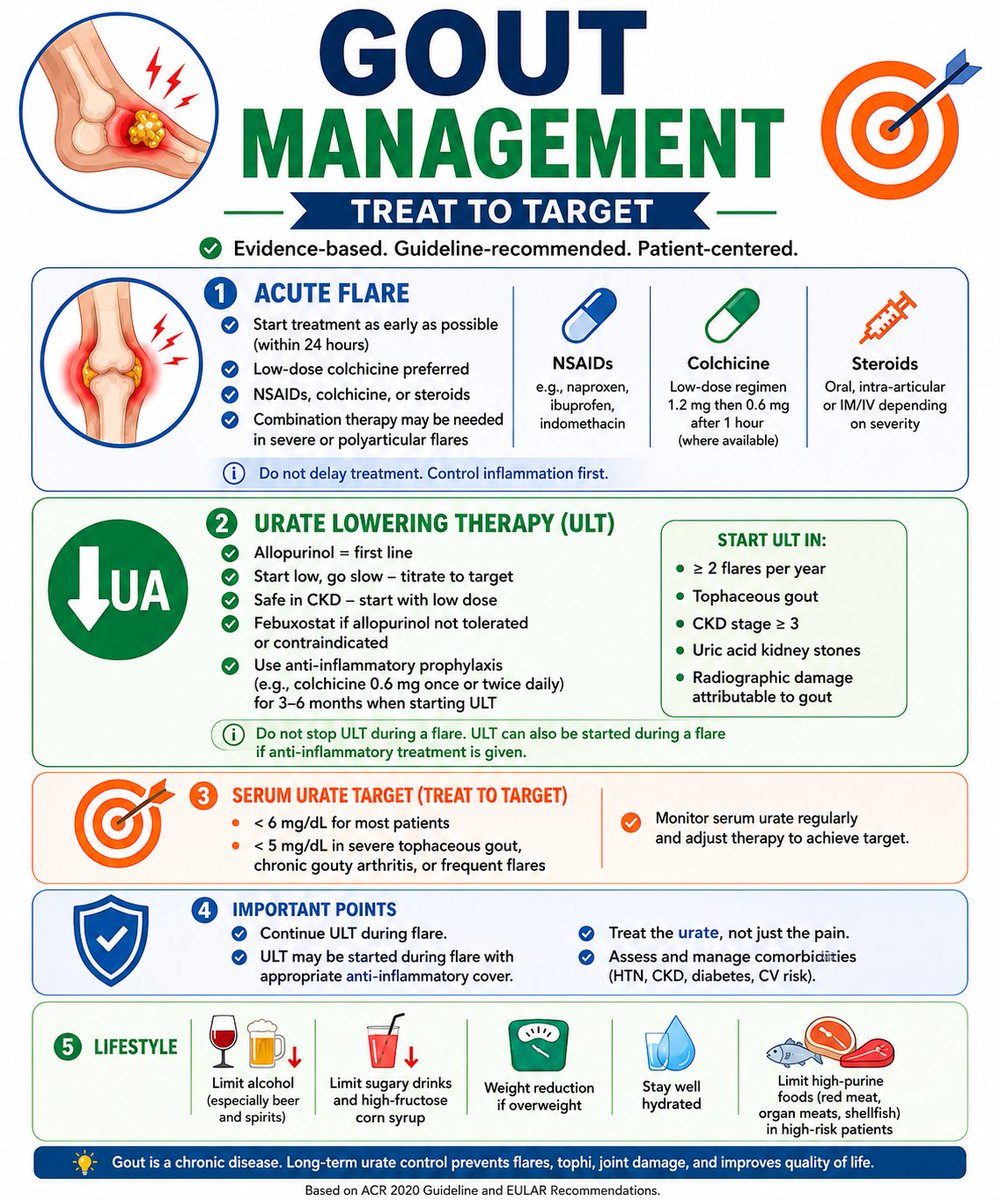
😻Favourite Nutritional Councelling for a Rheumatologist #GOUT diet
🍛A disease with robust evidence for dietary modifications
A thread…. Do 🔖 bookmark! 🚨‼️