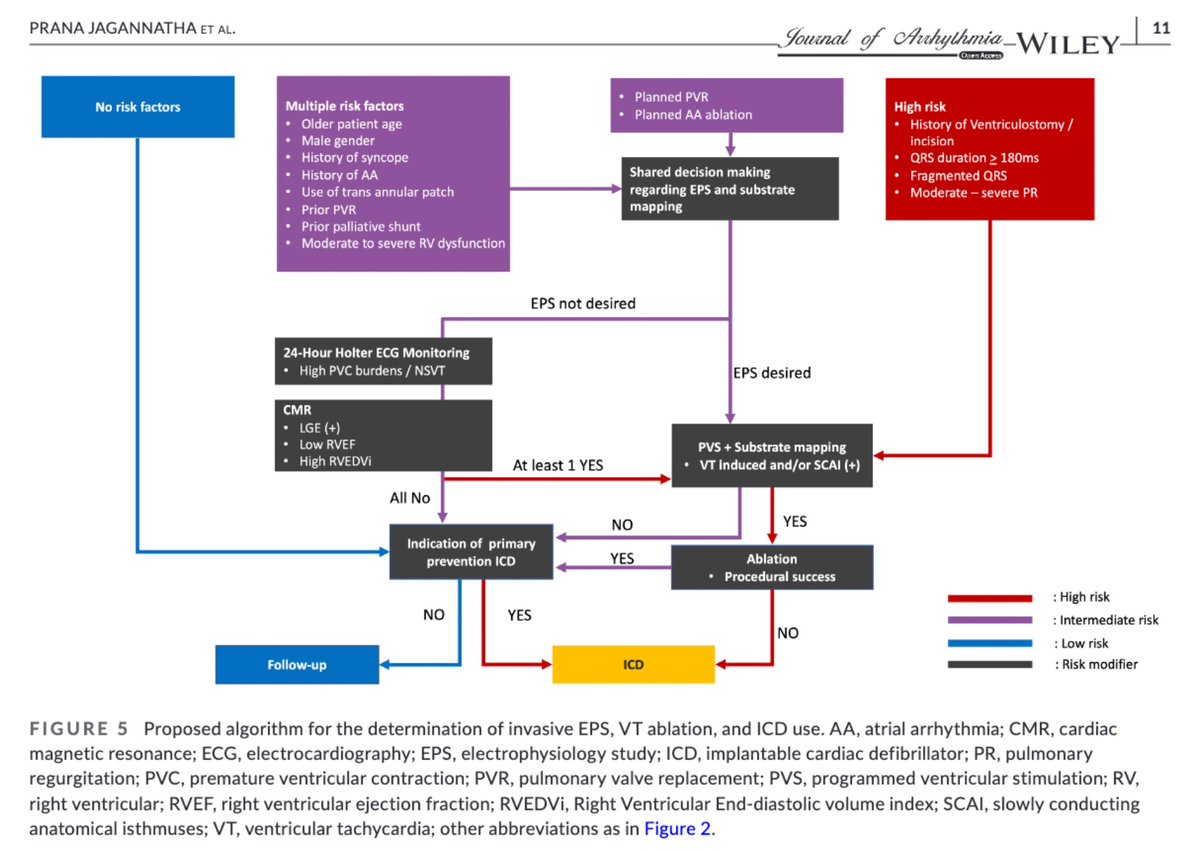
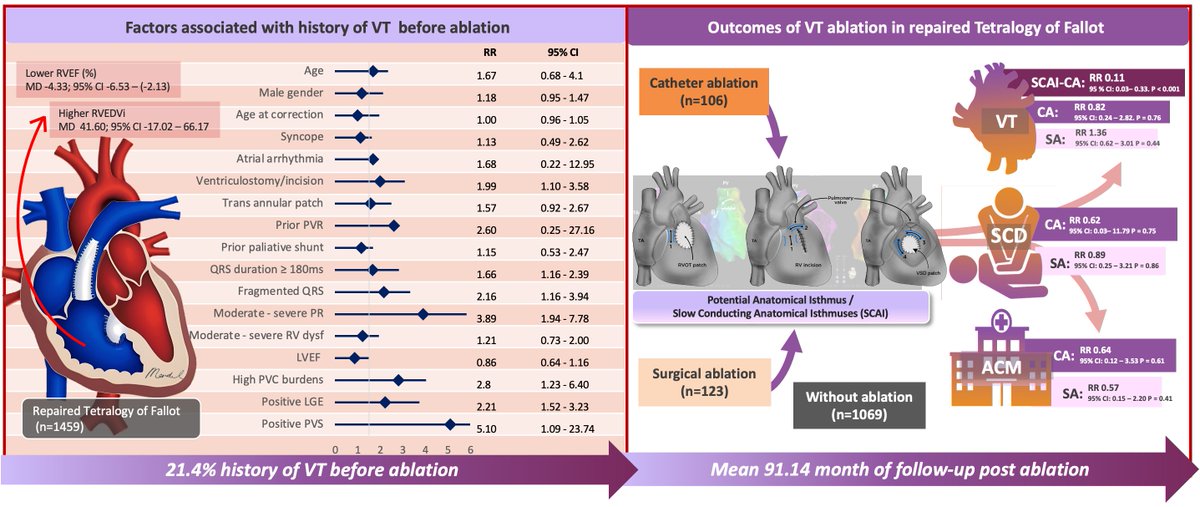
Proud to share our publication in the @aphrs_jhrs_joa "Long-term outcomes of #VT ablation in repaired #TOF : Systematic review and meta-analysis." We also propose a stepwise approach of risk stratification for VT ablation of repaired TOF. #Epeeps
https://t.co/YjFfHRN32w
🌟 SAN and AVN: The Elegant Coordination and “Backup Command Center” of Cardiac Electrophysiology 🌟
The sinoatrial node (SAN) and atrioventricular node (AVN) form one of the most beautifully coordinated systems in the human heart, working in perfect harmony to maintain stable cardiac rhythm.
But what happens when the SAN is damaged and fails to function? The AVN must step in as a reliable backup — otherwise, the heart could stop beating.
Common SAN disorders such as sinus arrest, sinoatrial block, and sick sinus syndrome raise an important question:
Why does the heart often continue to beat? The answer lies in the AVN’s intrinsic capability as a secondary pacemaker. It can generate a junctional escape rhythm (typically 40–60 bpm) when the SAN’s impulses are absent or too slow. Under normal conditions, the AVN’s slower intrinsic rate is suppressed by the faster SAN, but it stands ready to take over when needed.
This insight echoes the classic observations of cardiac electrophysiology pioneer Sir Thomas Lewis: Master the AVN, and you master much of arrhythmia disease. The AVN’s unique cellular composition and specialized tissue structure enable it to serve as a true “command center” — not only delaying conduction to allow proper atrial-ventricular synchrony, but also acting as a critical backup rhythm generator.
Atrial Conduction: From the James Hypothesis to Modern Understanding
• Classic James Hypothesis (proposed in 1963): Suggested the existence of three relatively discrete anatomical internodal tracts (anterior, middle, and posterior) connecting the SAN to the AVN as specialized fast conduction pathways.
• Modern Anatomical Consensus (Anderson School and leading textbooks): Detailed histological studies have not identified insulated, discrete tracts similar to the ventricular His-Purkinje system. Instead, atrial conduction relies primarily on anisotropic conduction — the directional arrangement and connectivity of atrial myocytes that efficiently propagate impulses from SAN to AVN.
This paradigm shift has profound implications for our understanding of arrhythmia mechanisms, ablation strategies, and advanced non-invasive diagnostics.
At PhysioSign, our saahECG (SAN-Atrial-AVN-His ECG / EpCG) technology is designed to capture the ultra-low-frequency subtle signals that conventional ECGs miss due to filtering. By enabling real-time, high-resolution, non-invasive visualization and analysis of the full conduction system, we help clinicians detect hidden abnormalities earlier and support more precise diagnosis and management of arrhythmias.
The heart’s built-in resilience — exemplified by the SAN-AVN backup mechanism — is truly remarkable.
PhysioSign
#ECG
#Cardiology
#Anatomy
#AI
The rightward extension of Bachmann’s bundle
In this new #DaVinciAnatomyCorner@JACCJournals chapter, we explore its anatomy and clinical implications for physiological atrial pacing (BB pacing) @cardiac_anatomy
We hope you find it useful .
https://t.co/typfGFxizz
A misleading concept in ECG teaching is the wrong explanation on how the septum is activated. Topics on CSP and the left septal fascicular block made me again realise the fallacy in the books.
The septum is activated in both directions ❗
These four pics show the activation of the septum in normal conduction and in LBBB. One pic shows the resultant vector from the left to right. The reality is different and the left septum can be activated from RV the way it's shown.
📄 Can we finally measure RV myocardial perfusion non-invasively?
🔗 https://t.co/Lr73MipUis
🫀 Right ventricular (RV) dysfunction is often driven by:
👉 pressure overload
👉 vascular remodelling
👉 impaired myocardial perfusion
❗ But here’s the challenge:
➡️ RV perfusion is extremely difficult to quantify non-invasively
✨ This study introduces a novel solution:
👉 Ultrafast Power Doppler (UPD)–based acFMBV
(attentuation-compensated fractional moving blood volume)
🔬 What did they do?
🧪 Animal model (pulmonary artery banding):
✔ RV pressure overload vs controls
✔ Histological validation (CD31 capillary density)
👶 Human cohort:
✔ Healthy children
✔ Patients with RV pressure overload
📊 Key findings:
🔥 acFMBV reflects true myocardial blood volume
✔ Strong correlation with capillary density
➡️ r = 0.78 (P < 0.01)
❗ In RV pressure overload:
➡️ Reduced myocardial blood volume
✔ Lower acFMBV in animals and humans
📉 Example:
👉 Humans:
✔ Healthy: ~4.8%
✔ RV overload: ~3.1% (P = 0.03)
👉 Animals:
✔ Significant drop vs controls
📈 The graphical abstract (page 2) shows:
✔ How UPD quantifies blood volume in myocardium
✔ Direct comparison with histology
🧠 Why this matters:
👉 RV adaptation depends on:
✔ microvascular remodelling
✔ oxygen supply-demand balance
❗ Until now → difficult to measure in vivo
➡️ acFMBV provides a direct, quantitative surrogate
🚀 Clinical implications:
👉 Potential tool for:
✔ Early detection of RV maladaptation
✔ Monitoring pulmonary hypertension / CHD
✔ Risk stratification
💡 Especially valuable in paediatric populations
⚠️ Take-home message:
🧩 We are moving from structure… to microvascular function.
👉 UPD-based acFMBV may open a new era in
non-invasive RV perfusion imaging
#Cardiology #Echocardiography #RightVentricle #PulmonaryHypertension #CardiacImaging #Ultrasound #Innovation #PediatricCardiology 🫀📊
Sir Thomas Lewis (1881–1945), a British cardiologist widely regarded as the father of clinical cardiac electrophysiology, was one of the leading figures in cardiology during the 1920s and 1930s. At that time, the mainstream academic view held that most cases of paroxysmal tachycardia and the irregular ventricular response in atrial fibrillation were caused by re-entry within the atrioventricular (AV) node and by concealed conduction through it.
Lewis focused on studying the filtering effect of the AV node during atrial fibrillation. Through animal experiments conducted between 1920 and 1935, his team demonstrated that the slow conduction velocity, uneven refractory periods, and propensity for re-entry in the AV node played a central role. This led the academic community to adopt a simplified and memorable conclusion:
“The atrioventricular node is the source of arrhythmia. Whoever can master the AV node controls the heart.”
AVN electrogram😍
PhysioSign
#ECG
#AI
#Cardiology
#AVN
#POCUS en #TEP permite ver el trombo, ver el esfuerzo del VD (estratificación de riesgo) y descartar otras causas de shock (tamponade, neumotórax), permitiendo iniciar trombolisis o intervenciones avanzadas bajo un criterio clínico sólido, en lugar de una espera que sería fatal.
🫀📊 **Diastolic dysfunction: are we finally making it simpler?**
Assessing left ventricular diastolic function remains one of the most challenging areas in echocardiography. Multiple variables, load dependence, age-related changes, and often discordant findings make interpretation difficult even for experienced imagers.
A new review proposes a **simplified, tier-based approach** aligned with the 2025 ASE recommendations, aiming to improve the clinical applicability of diastolic function assessment.
🔑 **Key concepts**
✅ Diastolic dysfunction should not be viewed as a single measurement but as a combination of:
• Impaired LV relaxation
• Increased myocardial stiffness
• Elevated filling pressures.
📈 The 2025 approach starts with what may be the most clinically useful marker:
👉 **e′ velocity**, reflecting myocardial relaxation.
Additional markers such as:
• E/e′ ratio
• Left atrial size and function
• Left ventricular hypertrophy
• Left atrial reservoir strain (LARS)
are then integrated in a stepwise fashion.
💡 One of the major advances is the introduction of a **tiered framework** for estimating filling pressures, reducing the number of "indeterminate" studies that frequently complicated the 2016 algorithm.
🏃 In patients with unexplained exertional dyspnoea, the paper reinforces the value of **diastolic stress echocardiography**, recognising that elevated filling pressures often become apparent only during exercise.
🤖 Perhaps the most exciting perspective is the role of artificial intelligence.
The authors propose that diastolic dysfunction may be better understood as a **latent phenotype**, integrating dozens of clinical and imaging variables rather than relying on a few Doppler measurements alone.
Machine-learning models have already demonstrated:
✅ Improved estimation of filling pressures
✅ Better prognostic stratification
✅ Identification of high-risk phenogroups that traditional algorithms may miss.
🎯 **Take-home message**
Diastolic dysfunction is not a binary diagnosis.