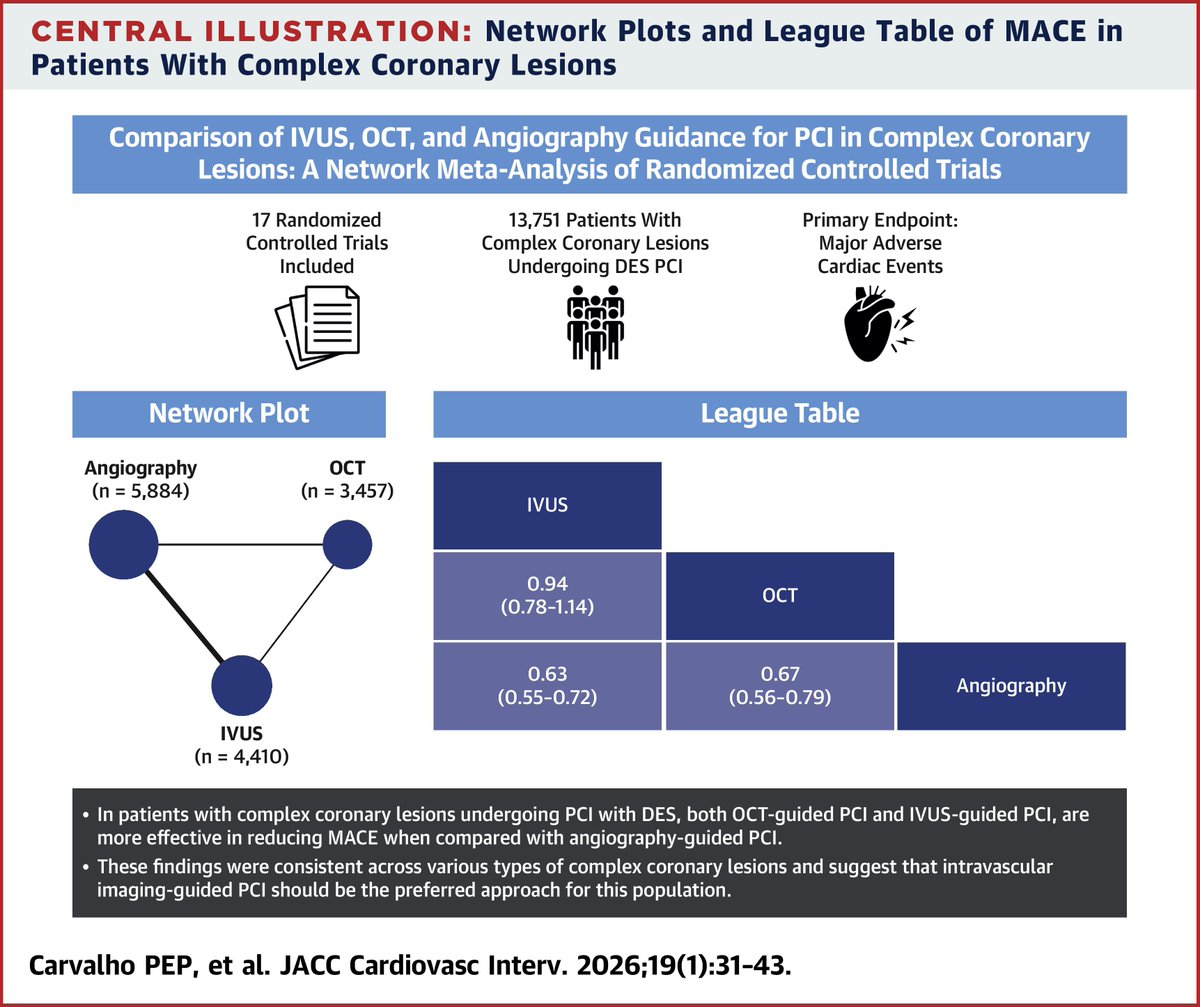
In this network meta-analysis of 17 RCTs (13,751 pts), both #IVUS & #OCT guidance were superior to angiography alone for 📉 #MACE in complex coronary lesions (LM, bifurcations, CTOs, calcified, MVD). There was no difference between IVUS vs OCT 🫀 https://t.co/cg7UvSTbpT #JACCINT
📊 New meta-analysis in #JACC: GLP-1 RAs reduced CV death, MACE & HF risk across 99K+ patients.
✅ Consistent benefits across diabetes, obesity, CKD & HF
⚠️ ↑ GI & gallbladder events
🎯 Personalize therapy by patient profile
Read more in the new issue: https://t.co/7hWeZqRHhk
Very cool - caffeine blocks adenosine receptors, which leads to faster heart rate, coronary vasoconstriction, and has historically thought to be a classic trigger for AFib episodes (thinking that caffeine amps up the heart as much as it amps up the mind).
By blocking adenosine, seems like caffeine could lengthen atrial cell refractory period, reduce ectopic triggers, and actually reduce the likelihood of AFib/flutter.
Keeping up with this topic is really exhausting. Stop everything—here’s a new meta-analysis, this time in patients with myocardial infarction and preserved ejection fraction (≥50%). The first piece of news is that, after I don’t know how many years since the last cardiovascular one, it’s published in @NEJM (and yes, it’s very concise but stylish, of course). The second piece of news is that my post below, which was somewhat of a guess, turned out to be correct. Patients who have had a myocardial infarction and maintain a normal ejection fraction cannot expect any difference in mortality, reinfarction, or heart failure if they take a beta-blocker. If their ejection fraction is below 50%, however, benefits can be expected—and that is what I will do from now on. Until the next trial is published the day after tomorrow, of course. #AHA25
https://t.co/EEy72YqUaJ
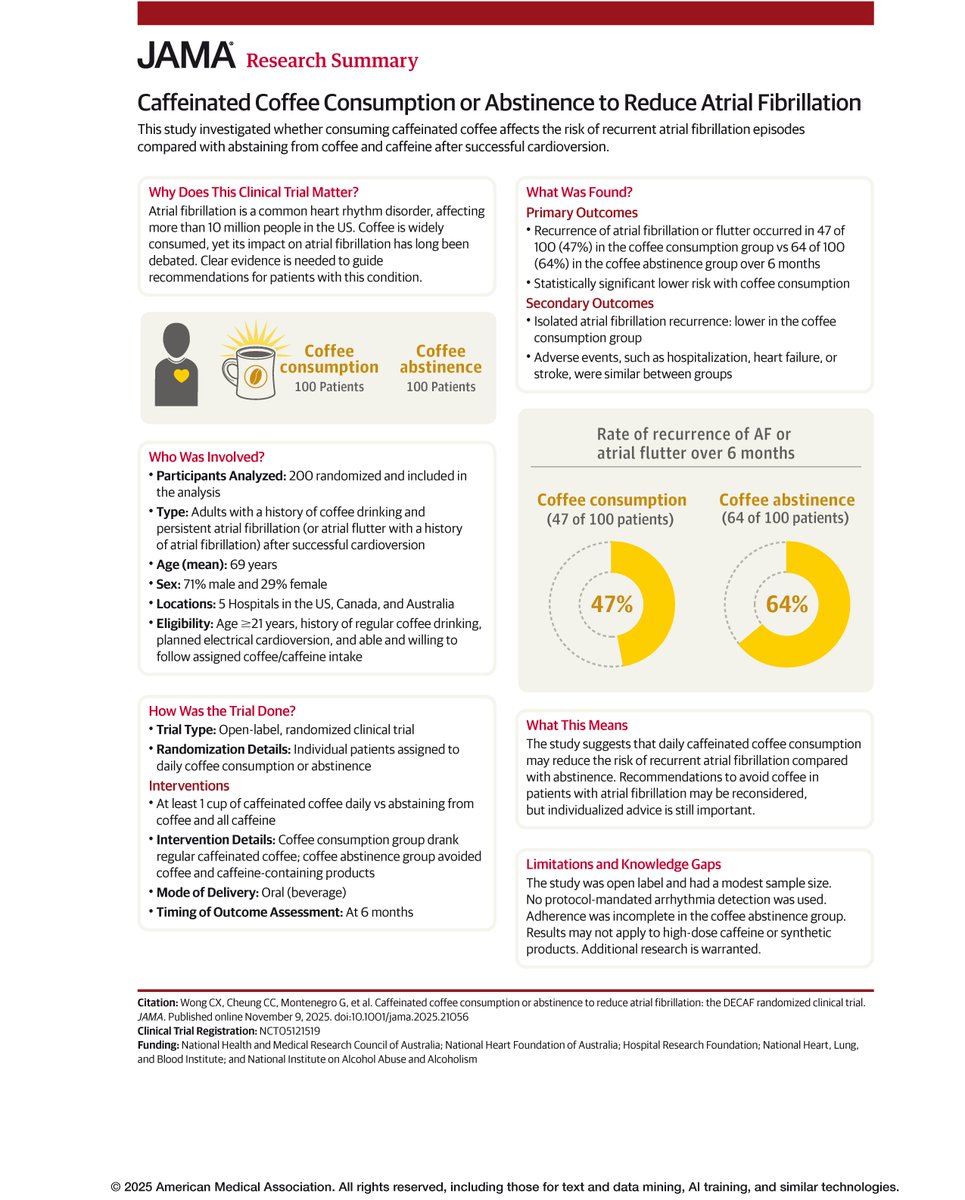
📊 Research Summary from @JAMA_current: Adults with #AFib who drank at least one cup of caffeinated coffee daily after successful cardioversion had a lower risk of recurrence than those who abstained from coffee and caffeine.
#AHA25@AHAScience
https://t.co/uKGpjxpc9T
Get this: Coffee suppressed atrial fibrillation!
Unexpected results for recurrence from a randomized trial in participants after cardioversion from AF
#AHA25@JAMA_current ☕️ https://t.co/70dPI2R84C
RIVAWAR trial: Rivaroxaban was found to be as effective and safe as warfarin in resolving post #cvMI left ventricular thrombus at three months. #ACC25
Get full details here: https://t.co/aOVMadNEtt
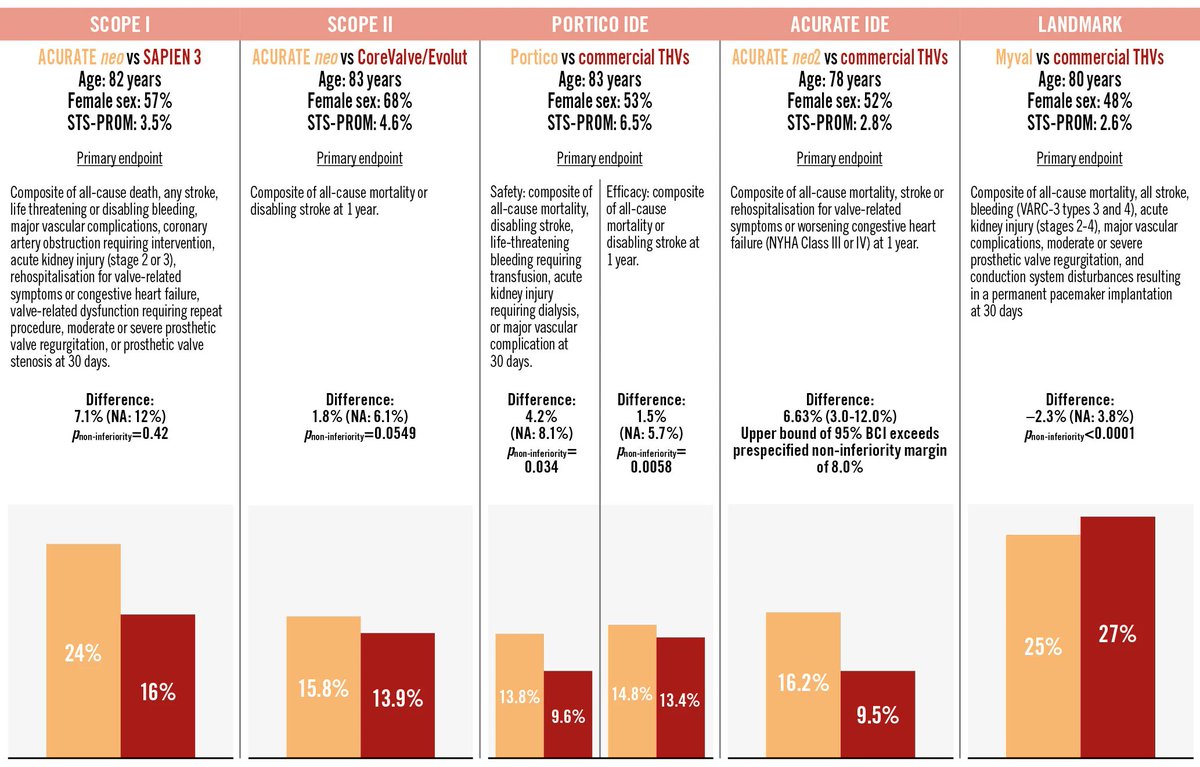
TAVI has become a key alternative to surgical aortic valve replacement, supported by strong evidence from randomized trials across all surgical risk levels. The balloon-expandable SAPIEN and self-expanding CoreValve/Evolut valves are established standards, with emerging valve technologies now undergoing direct comparisons against them. Here is a summary of such head-to-head comparisons.
https://t.co/T7nLi02dOJ
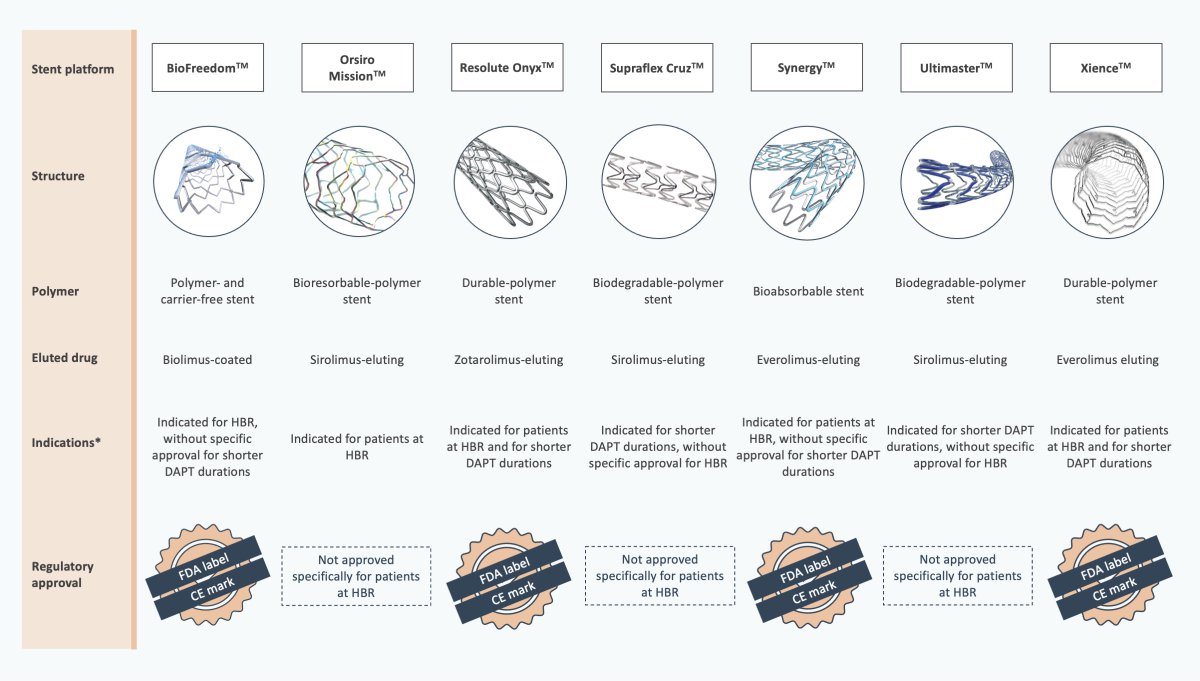
Are all stents the same for high bleeding risk (HBR) patients? BioFreedom, Resolute Onyx, Synergy, and Xience are approved for HBR patients by both the European Commission and FDA. While Orsiro Mission has strong evidence for HBR use, it lacks specific HBR regulatory approval. Ultimaster and Supraflex Cruz are not specifically labeled for HBR but are approved for short DAPT durations. We wrote a brief article on the topic of stent selection for HBR patients.
https://t.co/5eiCffSxdq
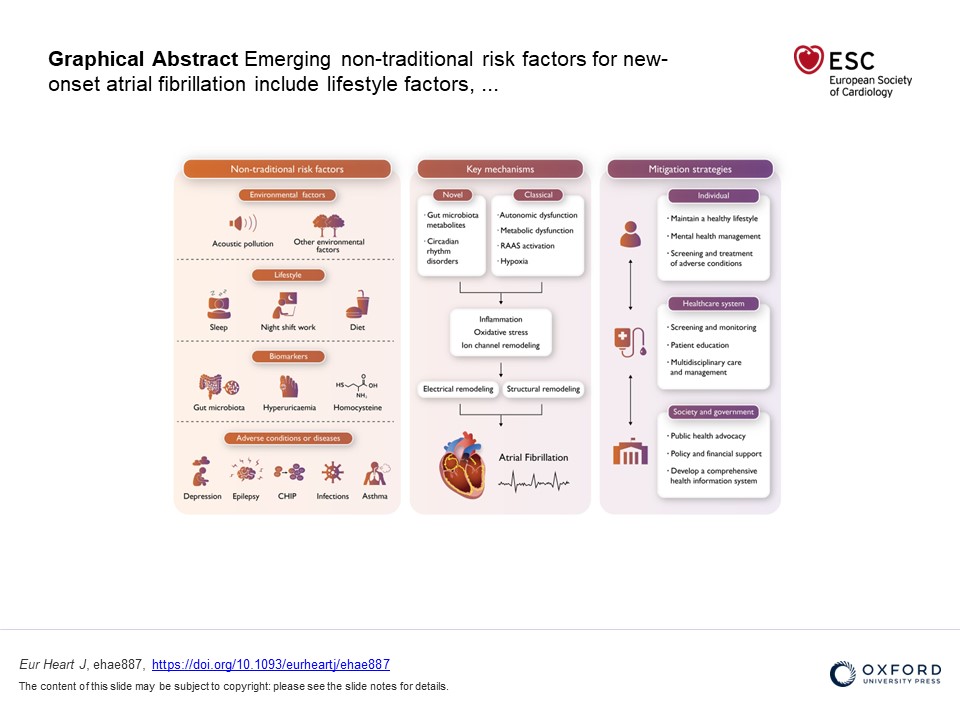
"Non-traditional risk factors for atrial fibrillation: epidemiology, mechanisms, and strategies": explore how unexpected factors impact atrial fibrillation and innovative approaches to prevention and treatment.
https://t.co/iyd54eqje7
@ESCardio@ESC_Journals#AF
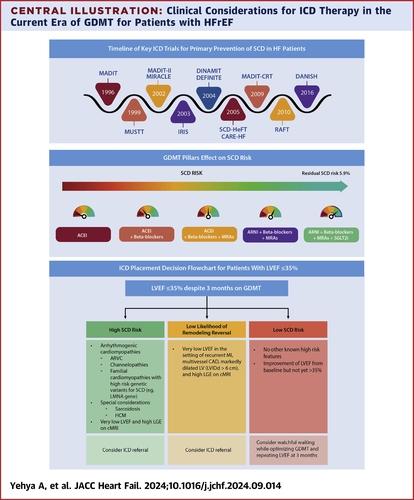
🗝️ Shared decision making for ICDs should highlight the survival benefit associated w/ them but also discuss possible complications associated w/ the device.
Read more key points on #epICD therapy for primary prevention in #HFrEF: https://t.co/YDlVBSolUi #JACCHF@JACCJournals