A warm #ASCO26 welcome to daraxonrasib and RASolute-302 study in 2nd line metPDAC from $RVMD
My story in the post below.
Here are the OS curves you haven't seen yet.
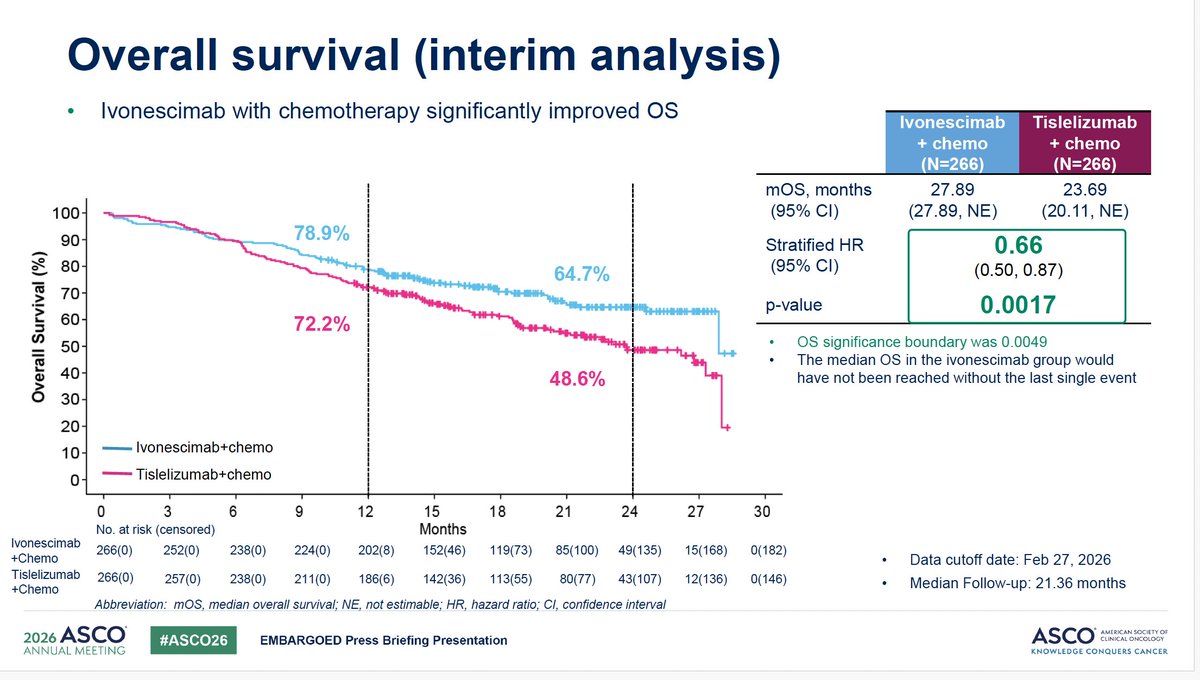
Here we, go #ASCO26. Ivonescimab HARMONi-6 for $SMMT Akeso and all those interested in PD1/VEGFs
STAT's @matthewherper story in the next post.
OS HR 0.66
mOS ivo+chemo 28 months v tis+chemo 24 months
The KM curve
Hello @JeffBezos, since you question the results of our studies on the unfairness of the US tax system, please allow me to remind you of the main conclusions of our work, the most comprehensive research to date on this issue.
When Kaplan–Meier Curves Fool You 📉
A flat survival tail can look exciting…
but sometimes it reflects very few patients remaining under follow-up.
The curve alone is never enough.
Always check: • Number at risk
• Censoring patterns
• Follow-up maturity
• Late-tail denominator
A “long-term survivor plateau” is meaningful only when enough patients are still being observed.
One of the most important lessons in interpreting immunotherapy trials.
#Oncology #MedEd #Biostatistics #Immunotherapy #ClinicalTrials #KaplanMeier #MVOnco
New @JCO_ASCO * analysis of ~5,000 HCC patients treated with external beam radiation therapy across 30 centers in 11 countries.
Median overall survival:
-BCLC-0 (very early stage, a single tumor 2 cm or smaller): 6.8 years
-BCLC-A (early stage, single tumor of any size or up to 3 tumors ≤3 cm each): 4.6 years
-Treatment-naive BCLC-A: 5.4 years
Retrospective, but the scale is striking. EBRT belongs in the frontline HCC discussion.
Using price transparency data, a union identified egregious pricing at NewYork-Presbyterian Hospital.
@RepBrianFitz cites charges at 358% more than Medicare.
“After this union dropped New York-Presbyterian from their network, they reportedly saved substantial resources.”
Our health care system is broken. These days, non-for-profit hospitals look more like hedge funds with hospital beds.
Today, @WaysandMeansGOP is holding a hearing with hospital CEOs as we continue our investigation into the health care empires that have raised prices and taken away access.
Politicians have refused to take on the health care empire and its lobbyists for too long. If we’re serious about lowering costs and expanding access to health care, nothing can be off-limits.
Large hospital systems are profiting off Medicare rules that pay them more for the same service than independent practices.
That means a senior in my district can pay MORE for an X-ray at a hospital than at a local doctor’s office -- and the hospital makes MORE too.
Today I asked hospital system CEOs a simple question: should we equalize payments to lower costs and expand access? They said no.
Americans deserve affordable care, not a system that rewards higher prices.
Even the CEO of the New York-Presbyterian hospital network admits the obvious; there are no “rural” hospitals in downtown Manhattan.
This is a prime example of why rural Americans face challenges accessing care and how benefits allocated for rural hospitals end up in exams rooms in big cities.
@RepCarolMiller
United Health Group (UHG) recently reported their Q1 2026 results, exceeding earnings expectations with $111.7 billion in revenue—a 2% year-over-year increase. They attribute their positive performance to “improved medical cost management.”
Just so we are all clear - medical cost management is code for prior authorization, downcoding, care denials, etc.
They take pride in denying care because it looks good on their earnings report.
¿Quienes y dónde publicaron sus resultados? Nunca lo dirás porque no resistiría ningún análisis serio.
Gente cómo tú son la razón por la que muchos no toman en serio a los economistas en la academia que se matan estudiando y publicando al más alto nivel. Eres una desgracia.
Boston biotech has been running the same playbook for years and everyone in the ecosystem knows it.
Early-stage companies are built less on validated biology and more on signaling: a splashy Nature or Science paper, a thin patent scaffold, and the reputational gravity of well-networked academic founders. That combination is often enough to unlock large funding rounds.
The problem is that high-impact publication has become a proxy for truth. It isn’t. It’s a selection mechanism for novelty and narrative.
The result is predictable:
– groupthink gets reinforced
– weak or irreproducible findings persist for years
– dissent is disincentivized
– hype substitutes for validation
In many cases, the goal is not to rigorously test whether an idea is correct, it’s to create enough mystique that it feels important. That perception alone can carry a company surprisingly far.
So it’s not surprising to see the same voices recycled across boards and advisory roles—people who helped build and legitimize this model in the first place.
The intuition makes sense. Reduce tumor burden, let systemic therapy finish the job. But intuition has a poor track record in oncology.
ORCHESTRA just published in JAMA. Phase 3 RCT, 382 patients, multiorgan mCRC. The bar for entry was high. You had to be able to take out more than 80% of disease burden across all sites before randomization. These are the best-case patients. Response or stable disease after 3-4 cycles of CAPOX or FOLFOX, then chemotherapy alone versus chemo plus debulking.
Median OS: 27.5 months versus 30.0 months. HR 0.88, 95% CI 0.70-1.10. p = 0.26. PFS essentially identical, 10.4 versus 10.5 months. Serious adverse events significantly higher in the debulking arm, 53% versus 39%.
That said, this isn’t the whole story. Symptomatic Krukenberg tumors, oligometastatic disease with curative intent, isolated liver-only disease. Those conversations should still be had.
The cytoreductive surgery literature gave us hints this was coming, but the use cases that make biological sense still stand.
What changes now? At minimum, “we can get more than 80% of it” is not a sufficient reason on its own. Except in NETs, NETs are weird.
https://t.co/yBHjrfGkO6
@gutonclab @oncoalert
I had largely decided to give up my oncology boards, which is depressing thinking of how hard I worked to get them, but I hate feeding the evil empire that rules our certification process. So I decided to sign up for LKA just to give it a try. @ABIM no happy ending to this.
@2StefanMoore He's trying to rewrite the rules of drug approval. He wants, "Let me just show you how it works on paper and you approve it because it 'makes sense'". I don't want to bother with the messy business of performing expensive, large, long phase III trials.
That might work in SA.
𝐄𝐱𝐜𝐞𝐥𝐥𝐞𝐧𝐭 𝐚𝐧𝐚𝐥𝐲𝐬𝐢𝐬 𝐨𝐟 𝐰𝐡𝐚𝐭 𝐓𝐫𝐮𝐦𝐩𝐑𝐱 𝐠𝐞𝐭𝐬 𝐰𝐫𝐨𝐧𝐠 𝐨𝐧 𝐩𝐫𝐢𝐜𝐢𝐧𝐠
The good: Cash-pay, DTC options can bypass PBMs and help deflate the gross-to-net bubble by lowering list prices.
The bad: Several brand-name drugs are still priced far above readily available generic equivalents, raising costs for patients who don't shop around.
The ugly: Despite the spin, this does not consistently "lower costs on the most popular drugs"
👉 Read more: @STATNEWS https://t.co/mbbMDwUupU
I am going to continue to fight for this. All government/public funded research should by default be open access. Such an important trial- funded by public money- cannot stay behind a paywall. Public funded the research, now they should pay to read the results? Doesn't make sense. https://t.co/Dmxpz1NS2B
HIGHEST RANKED TRIALS for 2025
TOP 10 #cancerclinicaltrials in 2025 w/MOST Impact
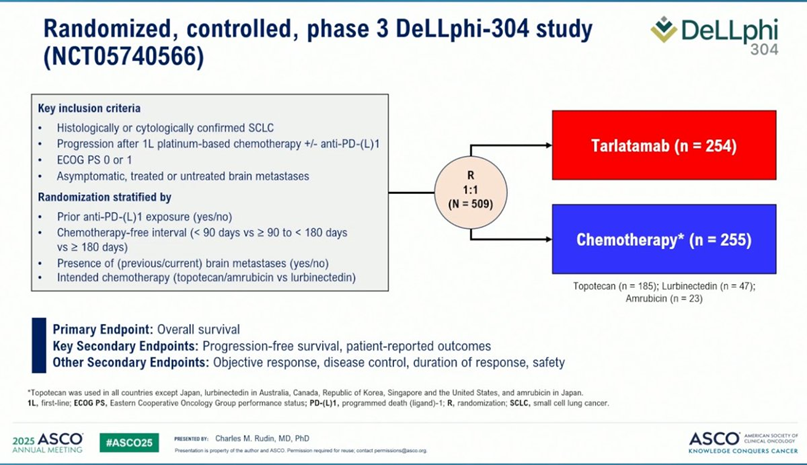
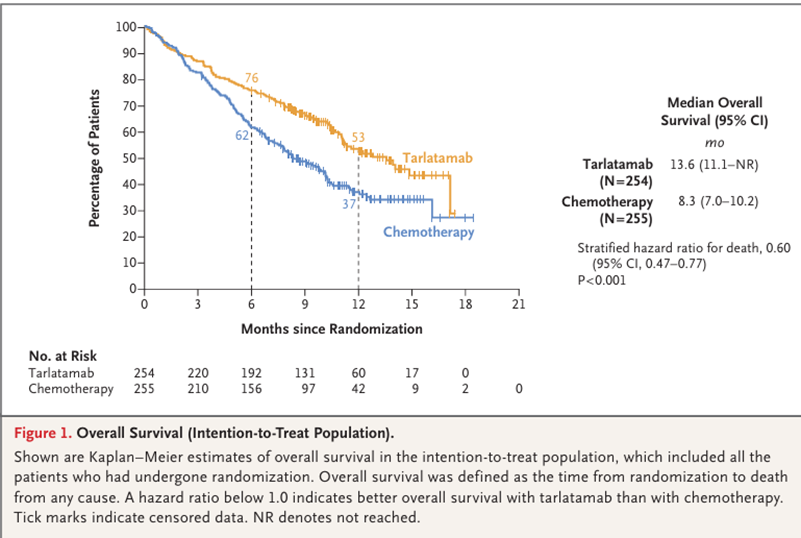
1/ #DeLLphi304@NEJM led by #Zeusofoncology@g_mountzios@HenryDunantGR : In relapsed SCLC post-platinum, BiTE DLL-3 Tarlatamab improved mOS vs. Chemo (13.6 vs 8.3 m, HR 0.60). PFS and in cancer-related dyspnea also improved.
https://t.co/dlIvlySUT9