Patient Advocate in clinical research and Guidelines in Oncology , trained by National Cancer Grid and Patientengage . studied at Vidyasagar University..
Many get CAR T-cell therapy to treat their myeloma, but what happens to your immune system afterward? Myeloma expert Dr. Joseph Mikhael explains in this short video.
@jmikhaelmd@Bethfaiman#AsktheIMF#mmsm
Good morning! Just got to know this!
1/2 A whole government Ministry is unleashed on me - because I speak against unscientific practices and primitive traditional healthcare that can harm, I communicate scientific information for public and patients alike.
This was an official memo released during the Ministry of Ayush meeting on 12-6-2026 fully dedicated towards shutting down my social media presence.
Imagine - the people in this meeting were eating biscuits and drinking tea, paid for by the citizens of the country - to decide how to gag and shutdown a citizen doctor who educates people on medical science via social media.
Yesterday, my Instagram account was briefly hacked, but I got back control and removed unauthorized access within an hour.
The Article 51A(h) of the Indian Constitution outlines the fundamental duty of every citizen to develop a "scientific temper, humanism, and the spirit of inquiry and reform". Added during the 42nd Amendment in 1976, this non-justiciable directive promotes logical reasoning, critical thinking, and rationality.
The Ayush system is not scientific, it kills scientific temper, it does not promote the spirit of inquiry, it lacks logical reasoning, has the deadest version of critical thinking and none of its products and practices are rational.
The only thing that needs to be shut down, is an unscientific body like Ayush that goes against the Indian Constitution and wastes public tax money... and not me.
Also, please look closely at the person at the end, who is copied to, by the Ministry. His name is Vaidya K P Manikandan and he is the owner and founder of CNS Ayurveda Hospital, where children are treated for chronic conditions such as severe mental health disorders, autism and epilepsy (please see an official release from the hospital in the next post). One such victim of his was saved by my team (we reported it: https://t.co/eXeWt2n6N7) and he put a criminal defamation case against me and the authors (for publishing a scientific peer reviewed paper!) which was later "stayed" by the High Court of Kerala.
This has nothing to do with service to patients, but everything to do with protecting the business of alternative medicine (especially Ayurveda). These low life complaintants should be ashamed.
PRESS RELEASE
International Myeloma Foundation (IMF) and International Myeloma Working Group (IMWG) to Honor 2026 Kyle and Durie Achievement Awardees, Dr. Hermann Einsele and Dr. Noopur Raje
https://t.co/aLu7xfzi8T
@VincentRK kicking off this years IMWG summit. The room is electric with a sense of duty, science and cure. @IMFmyeloma bringing myeloma experts from across the globe together for the singular purpose of curing this disease. It’s an honor to be in this room #mmsm
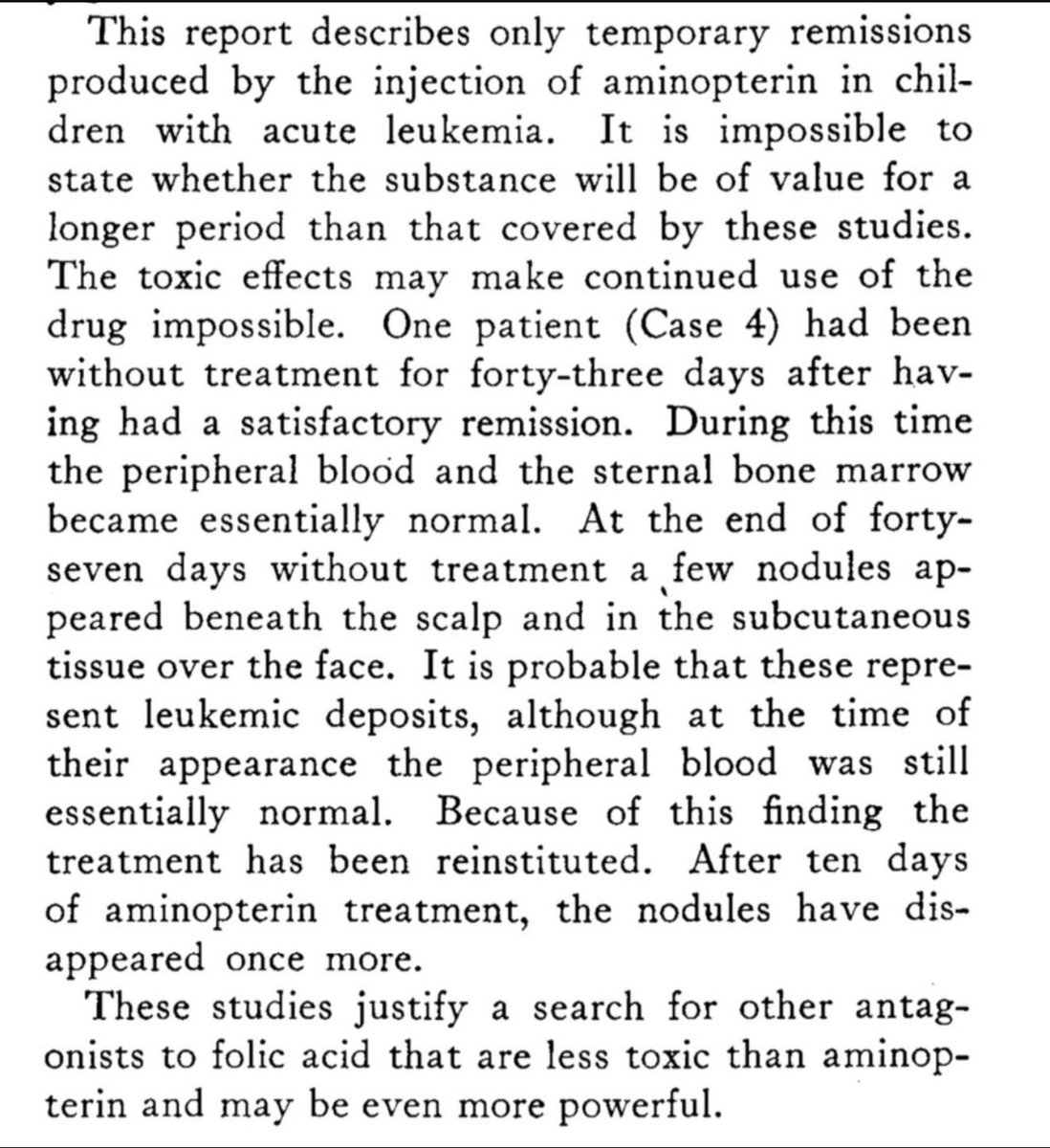
In 1948, Sidney Farber and colleagues published his work in @NEJM that helped open the door to modern chemotherapy.
Seeing that history from the same institution — especially after a remarkable #ASCO26 with major plenary contributions and @NEJM papers from @DanaFarber — is humbling.
A powerful reminder that progress in oncology is built across generations: by patients, scientists, clinicians, and teams who keep asking what might be possible.
Very exciting and promising. Once undruggable and invincible, KRAS has finally fallen after some remarkable researcher refused to back down. Science is the ultimate winner and basic scientific research is the main tool for real breakthrough.
In 1982, scientists named KRAS the first human oncogene. For the next four decades, some of the sharpest minds in cancer biology called it "undruggable."
Today, that word officially expired.
At the ASCO plenary this weekend, the phase 3 RASolute 302 trial showed a once-daily oral pill nearly doubling overall survival in second-line metastatic pancreatic cancer — published simultaneously in the New England Journal of Medicine.
For context on why this is hard: pancreatic cancer is the most RAS-addicted cancer we have, with KRAS mutations in more than 90% of patients. Five-year survival sits around 3%. Second-line chemotherapy has offered modest benefit for years.
The science took four decades and several relay handoffs to get here:
1982 — KRAS identified as the first human oncogene
2013 — Shokat's lab at UCSF finds the hidden switch-II pocket, reopening the field
2021–22 — sotorasib and adagrasib become the first KRAS inhibitors, but only for G12C, which is rare in pancreatic cancer
2026 — daraxonrasib, a multiselective RAS(ON) inhibitor, finally hits the G12 variants that actually drive PDAC — and wild-type RAS too
RASolute 302 randomized roughly 500 previously treated patients to oral daraxonrasib or investigator's-choice chemotherapy. In the intent-to-treat population: median OS 13.2 vs 6.7 months (HR 0.40, p<0.0001), median PFS 7.2 vs 3.6 months, and a response rate of 31.6% vs 11.2% — with benefit across RAS mutation status.
I want to hold two things at once here.
This is a genuine inflection point AND it comes with a real management burden. Daraxonrasib showed no new safety signals, but the rash, stomatitis, and diarrhea are not trivial — they need proactive, dermatology-informed supportive care. That's straightforward at an academic center. It's harder in the community settings where most patients with pancreatic cancer are actually treated. If "undruggable to doubled survival" is going to mean something for every patient, the supportive-care playbook has to travel with the drug.
That's the part of these stories I keep coming back to: the breakthrough and the delivery system have to arrive together.
For the scientists who refused to give up on a target everyone else abandoned — and the patients and families who enrolled when there was no guarantee — this is their result.
As we move RAS(ON) inhibitors toward first-line and into lung and colorectal disease, we have to make sure the supportive-care infrastructure reaches broader oncology community at the same pace as the drug discovery.
#Oncology #PancreaticCancer #KRAS #PrecisionMedicine #ASCO2026 #DrugDevelopment #ClinicalTrials #CommunityOncology #HealthEquity
In 1982, scientists named KRAS the first human oncogene. For the next four decades, some of the sharpest minds in cancer biology called it "undruggable."
Today, that word officially expired.
At the ASCO plenary this weekend, the phase 3 RASolute 302 trial showed a once-daily oral pill nearly doubling overall survival in second-line metastatic pancreatic cancer — published simultaneously in the New England Journal of Medicine.
For context on why this is hard: pancreatic cancer is the most RAS-addicted cancer we have, with KRAS mutations in more than 90% of patients. Five-year survival sits around 3%. Second-line chemotherapy has offered modest benefit for years.
The science took four decades and several relay handoffs to get here:
1982 — KRAS identified as the first human oncogene
2013 — Shokat's lab at UCSF finds the hidden switch-II pocket, reopening the field
2021–22 — sotorasib and adagrasib become the first KRAS inhibitors, but only for G12C, which is rare in pancreatic cancer
2026 — daraxonrasib, a multiselective RAS(ON) inhibitor, finally hits the G12 variants that actually drive PDAC — and wild-type RAS too
RASolute 302 randomized roughly 500 previously treated patients to oral daraxonrasib or investigator's-choice chemotherapy. In the intent-to-treat population: median OS 13.2 vs 6.7 months (HR 0.40, p<0.0001), median PFS 7.2 vs 3.6 months, and a response rate of 31.6% vs 11.2% — with benefit across RAS mutation status.
I want to hold two things at once here.
This is a genuine inflection point AND it comes with a real management burden. Daraxonrasib showed no new safety signals, but the rash, stomatitis, and diarrhea are not trivial — they need proactive, dermatology-informed supportive care. That's straightforward at an academic center. It's harder in the community settings where most patients with pancreatic cancer are actually treated. If "undruggable to doubled survival" is going to mean something for every patient, the supportive-care playbook has to travel with the drug.
That's the part of these stories I keep coming back to: the breakthrough and the delivery system have to arrive together.
For the scientists who refused to give up on a target everyone else abandoned — and the patients and families who enrolled when there was no guarantee — this is their result.
As we move RAS(ON) inhibitors toward first-line and into lung and colorectal disease, we have to make sure the supportive-care infrastructure reaches broader oncology community at the same pace as the drug discovery.
#Oncology #PancreaticCancer #KRAS #PrecisionMedicine #ASCO2026 #DrugDevelopment #ClinicalTrials #CommunityOncology #HealthEquity
Excellent observation. You can’t replace human intellect by its own creation. Fundamental science research is the foundation of scientific breakthrough. If you cut funding basic clinical research, you would certainly destroy further amazing discoveries extremely benificial to ours .
Human scientific ingenuity and hardwork, not AI. Human clinical trialists and patients, not AI
The standing ovation at #ASCO26 for the unprecedented results in metastatic pancreatic cancer with daraxonrasib an oral RAS inhibitor is the result of research excellence and perseverance, and a witness to this.
AI won’t do the work or run the trials to make these advances. It can make the process easier in the future. But you still need human ingenuity and hard works to take a chemical and make it an effective approved medicine.
Institutions and companies must nurture the human talent. Academic medicine is bleeding talent. Leaders are appointed for pliability over excellence. With NIH funding of new investigators at an all time low, coupled with institutions and organizations extolling the efficiencies and prioritizing the virtues of AI, we are at risk slowing down our ability in drug development.
https://t.co/2YRwESyIuu
This curve brought me to tears.
I treated a patient on this trial, and it took his terrible pain away completely within days, which is simply not common.
This represents decades of scientific perseverance and millions of patients who will now live longer and with less pain. 👏🏻
This is that watershed moment in oncology. The previous ones I recall is the story of checkpoint inhibitors and CAR-T cell therapy. Science is incredible. Translational research is even more incredible. @ASCO