Incredibly humbled to hear from @JosephSakran for the 2nd Annual #HealthEquity Grand Rounds. He met with trainees and discussed further the ways surgeons can engage in their work meaningfully by building their clinical content expertise and adding advocacy and passion work.
Top lung cancer developments in 2025?
My take:
2025 wasn’t about a single disruptive moment. It was about consolidation, maturation, and a few long-awaited signals finally turning solid.
1) MARIPOSA delivers OS
Amivantamab + lazertinib demonstrates an overall survival benefit over osimertinib in first-line EGFR-mutant NSCLC. Toxicity, logistics, and sequencing still matter—but this is now a real OS-based conversation, not just a PFS debate.
2) FLAURA2 confirms upfront intensification can matter
Osimertinib + chemotherapy shows improved OS vs osimertinib alone. Reinforces that combination strategies can deepen benefit, at the cost of complexity and tolerability. “Best first-line EGFR strategy” is now legitimately plural.
3) HER2 finally matters clinically
Accelerated approvals for zongertinib and sevabertinib in HER2-mutant NSCLC. Oral TKIs, meaningful response rates, and a credible path beyond antibody-drug conjugates alone.
4) EGFR exon 20 keeps inching forward
Sunvozertinib approved post-platinum. Incremental progress, but still meaningful in a historically difficult molecular subset.
5) c-MET ADC enters routine practice
Telisotuzumab vedotin approved for MET-high NSCLC. Expression-based biomarkers and ADCs are now firmly embedded in lung cancer decision-making.
6) A genuine advance in SCLC
Tarlatamab converts to full approval in platinum-refractory ES-SCLC with a survival benefit. Rare, and important.
7) Companion diagnostics become unavoidable
HER2 TKD, EGFR exon 20, MET expression—therapy is increasingly inseparable from the assay used to define eligibility. Testing strategy is now a core clinical decision.
8) Combination immunotherapy reality check
ATR inhibition + durvalumab misses OS (LATIFY). A reminder that biological plausibility still has to survive Phase 3.
9) AI moves from novelty to infrastructure
Improved CT nodule detection, risk stratification, and workflow support. Still assistive, not autonomous—but no longer theoretical.
10) Direction of travel is clear
More rare targets, more ADCs, OS gains in EGFR-mutant disease, slow but meaningful progress in SCLC—and increasing pressure on systems to deliver precision care at scale.
Bottom line: 2025 didn’t reinvent lung cancer. It made several long-promised ideas finally defensible at the OS level. That’s quieter progress—but it’s the kind that lasts.
#LCSM @SylvesterCancer@IASLC@myESMO@lungoncdoc@Latinamd@COlazagasti@Jani_Chinmay@NarjustFlorezMD@DrJNaidoo@StephenVLiu@EddieSantosMD@RManochakian@LuisRaezMD@uicc
When my mother was choosing between lobectomy and SBRT for a small lung cancer, the real question wasn’t which treatment was “better,” it was which one would preserve the life she worked so hard to maintain.
Her decision hinged on the quality of her life after treatment.
When two well-validated options offer similar chances of cancer control, the conversation naturally shifts to what matters most: independence, mobility, and the ability to keep living the life a patient values.
For her, the choice became unmistakably clear.
🔗 https://t.co/jKWytFCNSw
The hardest lessons after training aren’t always in the OR or clinic.
🙏 I wrote this essay for anyone navigating their first year as an attending.
“Unseen Scars” in @JAMA_current
🔗https://t.co/0e09Zx1nb6
So excited for the 6th Annual William H. Pearce, MD Research Symposium tomorrow, showcasing the research done by our amazing trainees this year, a talk by Edelstone-Bendix Visiting Professor @laparoscopes, and the graduating chiefs residents!
Join us Thursday, June 12 at 9am for the @NMSurgery Research Conference INSIGHT Presentations. We'll hear from Daniel Liesman, MD, Nicole Ontiveros, MD and @John_B_Rode. All moderated by @LaraLopesMD.
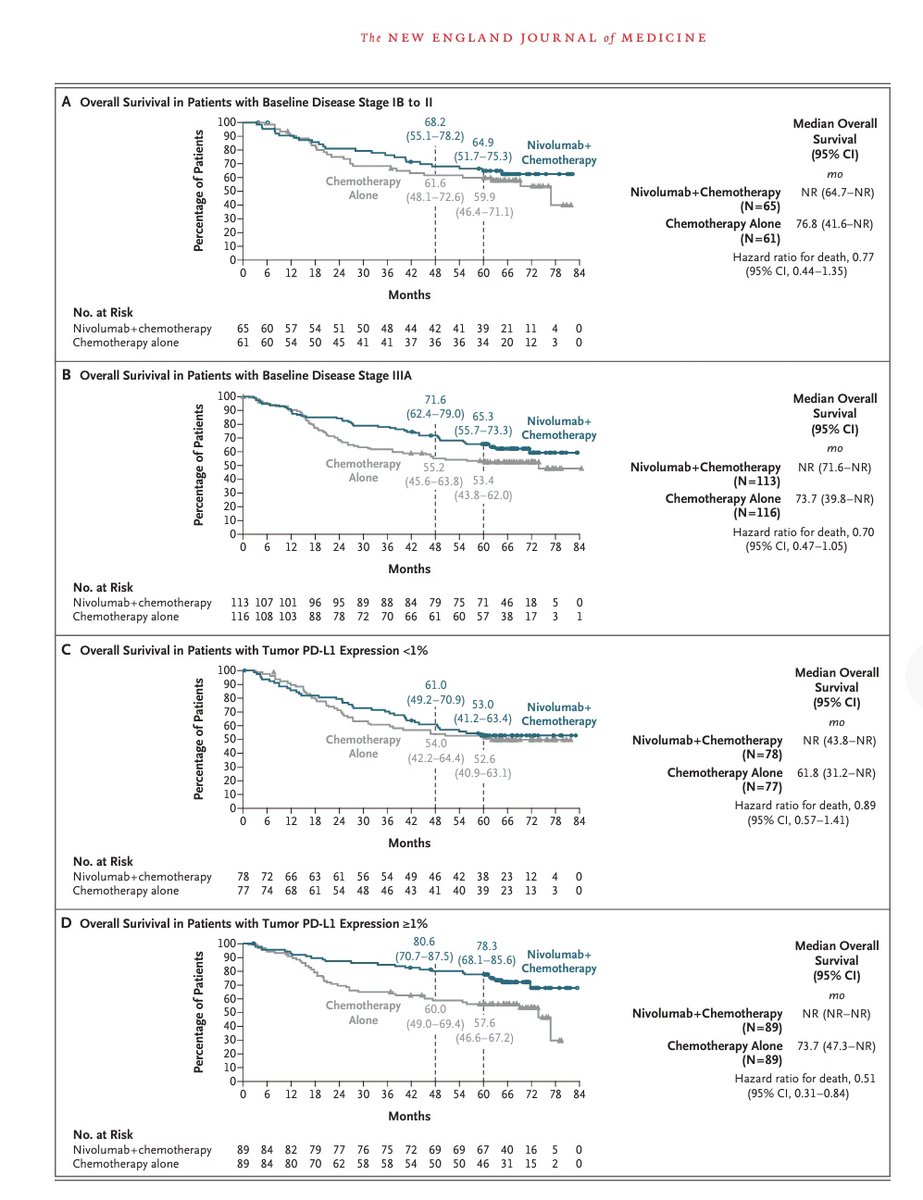
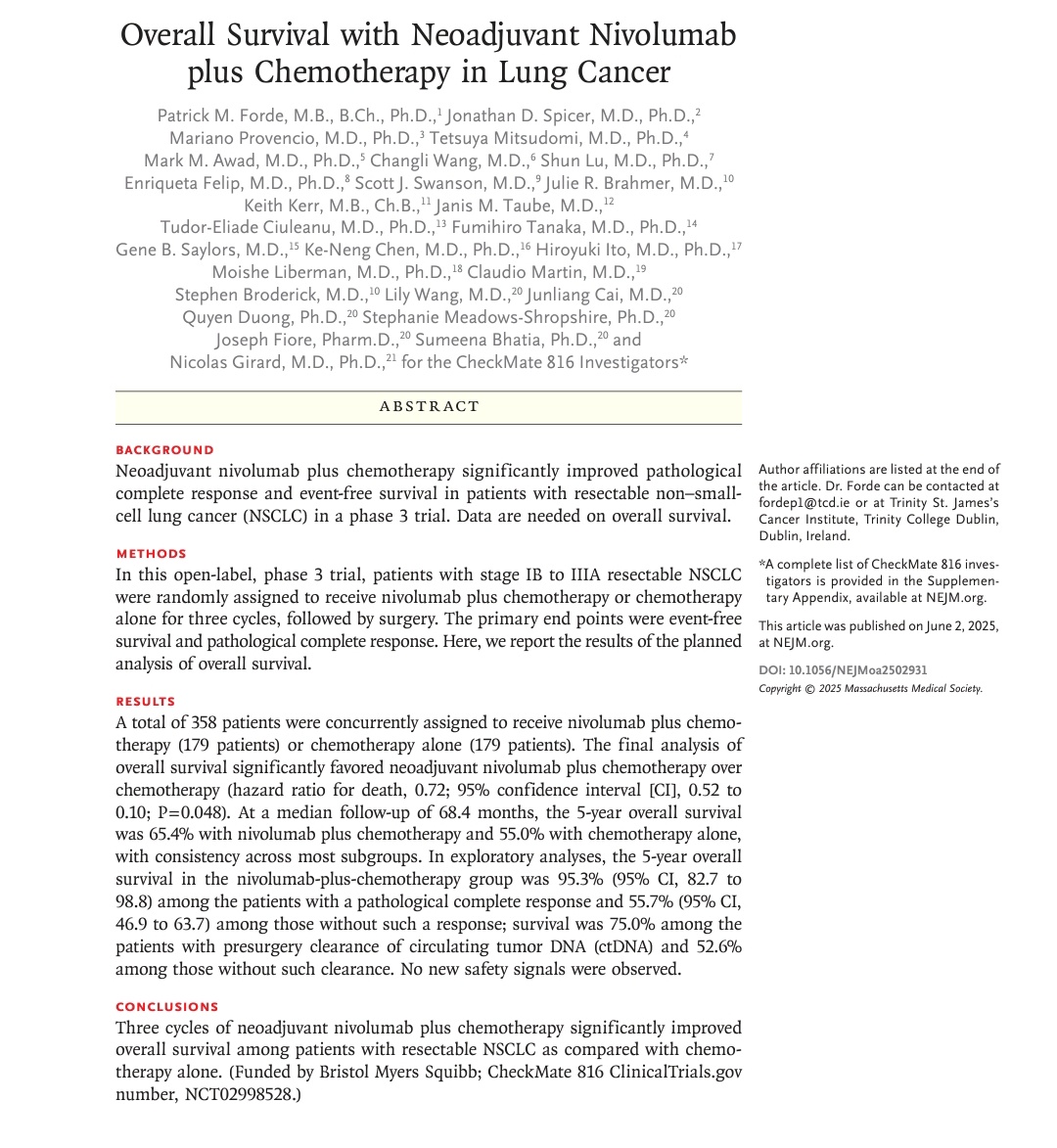
Landmark OS data from #CheckMate816 just dropped in @NEJM!
🫁 Neoadjuvant #Nivolumab + chemo in resectable #NSCLC delivers:
✅ 5-yr OS: 65.4% vs 55.0%
✅ HR: 0.72 (p=0.048)
✅ Lung cancer–specific survival HR: 0.65
✅ OS with pCR: 95.3%
✅ ctDNA clearers: 75%+ OS
📌 No lung cancer deaths in pCR patients
#LungCancer #Immunotherapy #ASCO25 #Oncology @FordePatrick@asco@OncoAlert
This is a major story from #ASCO25. Randomized phase 3 trial of time of day of immunotherapy infusion. Randomized to infusion before or after 3pm. Early infusion far superior: PFS 11.3 vs 5.7 HR 0.42, OS HR 0.45! Impactful, pragmatic, not costly. This should be a bigger story.
So you've heard the practice changing exercise CHALLENGE trial! But what did that groundbreaking exercise program actually look like day-to-day? Let's explore the "Structured Exercise Program" based on info from their paper supplement on NEJM #ASCO2025#ASCO25 1/10
Presented at #ASCO25:
A 3-year structured exercise program after adjuvant chemotherapy for colon cancer improved disease-free and overall survival, physical functioning, and fitness, as compared with health education alone. Full CHALLENGE phase 3 trial results: https://t.co/j3kWJDjuVz
@ASCO
Remarkable results for neoadj chemo-immunotherapy in locally advanced, N2/N3, lung cancer. 75% curative resections w v high pCR. Notably >40% of pts treated had high PD-L1 (unselected would be ~25-30%) but the boundary for lung surgery continues to chase the horizon #LCSM
🔥 Final analysis: CheckMate 577
Adjuvant nivolumab in resected stage II/III EC/GEJC post-CRT & surgery
✅ DFS benefit maintained
21.8 vs 10.8 mo
HR 0.76 (95% CI 0.63–0.91)
🧠 DMFS improved
27.3 vs 14.6 mo
HR 0.75 (95% CI 0.62–0.90)
⚠️ OS not statistically significant
51.7 vs 35.3 mo
HR 0.85; P = 0.1064
Grade 3–4 TRAEs: 14% vs 7%
Discontinuation: 5% vs 3%
#Immunotherapy #GIcancer #CheckMate577 #ASCO25 #OncoTwitter @ASCO@NiuSanford@GIcancerDoc@OncoAlert