Employers don’t know the price of medical care from big hospitals.
Employers don’t know how much their insurance company pays those hospitals or providers for that same care
If you don’t know the price, and you don’t know what your insurance company paid for that care.
How do you know if what your employer should be paying the insurance company for that care ?
You don’t.
Spread pricing from insurance conglomerates is an enormous tax on employers.
Direct Contracting is the answer. It most cases, it costs so much less, the employer can eliminate the employee out of pocket cost !
And
The hospital/provider will make more money with the insurance conglomerate out of the middle.
https://t.co/IjW3BsvfN1 for direct contracts you can use.
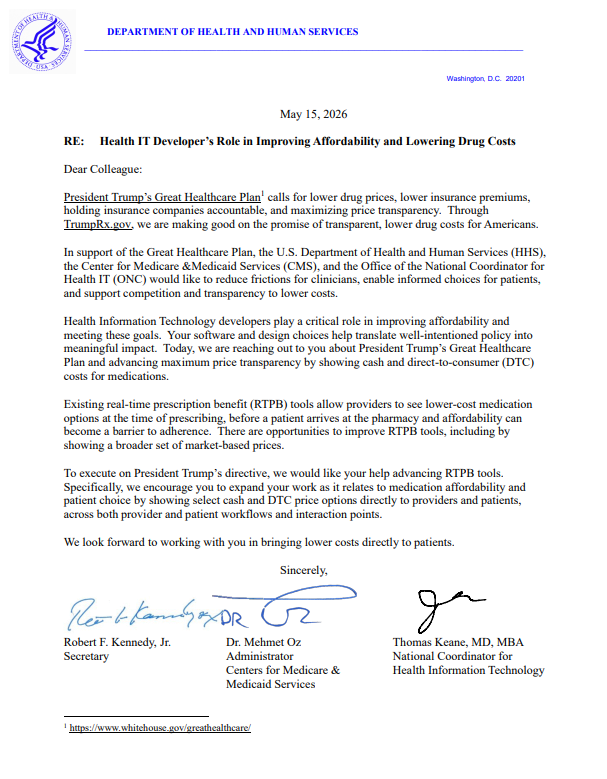
Patients deserve to know what their medications cost before they leave the doctor’s office.
@DrOzCMS, National Coordinator for Health IT @ONC_HealthIT Tom Keane, and I are calling on electronic health record vendors to accelerate the integration of drug price transparency into clinical care — well before the 2028 regulatory deadline.
We are also asking them to include cash-pay and direct-to-consumer drug prices on their platforms, which can be lower than the prices patients would pay through insurance.
Our priority is simple: give patients the drug price transparency they need to find the most effective medications at the lowest cost.
.@mcuban, co-founder of @costplusdrugs: "As our volumes go up, our costs go down, which means we'll be ending up charging less to people over a period of time... This is a special partnership. 559 of those drugs are ours, so we're really excited to be part of this."
He is right. By direct contracting with employers, the providers make more money (they get to keep what the ins companies were taking )
Cut their overhead AND MOST IMPORTANTLY, even when making more, they are charging employers FAR LESS
The best part is that the providers already know which employers they are dealing with All they have to do is call them up and explain the value !
Whether it’s existing consulting firms, new ones that emerge, FDEs from agent vendors, or new internal agent engineering roles, the amount of work that is going to be created to implement agents in enterprises will exceed anything we imagine today.
The complexity of implementing agents in any existing organizations is very real. When I talk to large enterprises, as you move from a chat paradigm to agents that participate in meaningful workflows, there are a number of things they need to do.
First, you have to get agents to be able to talk to your data securely across your systems. In many cases, enterprises have decades of legacy infrastructure that contain the valuable context for AI agents. That’s going to take a ton of work to go modernize and move to systems that work well with agents.
Then, you need to ensure that you’ve implemented agents with the right access controls and entitlements, the right scopes to be safely used, and have ways of monitoring, logging, and securing the work that they do.
Next, you need to actually document the processes in the organization in a way that agents can utilize for doing the work. You also need to figure out what the new workflow looks like when agents and people are working together on a process, and who steps in where. Just replicating the old workflow will mute the gains. Oh and you likely need to create evals for your top new end-state processes.
Finally, you have to keep up with a rapidly changing set of best practices and architectural shifts happening in the agent space. While it’s fun for people to change their personal productivity tools on a dime, it’s 100X harder to do this in a business process. The speed of change is a blessing and a curse right now for anyone trying to keep a stable system design.
All of this means that individuals and companies that develop expertise on the above set of components (and more) are going to be needed to help organizations actually implement agents at scale. This is also the rationale for vertical AI agents right now that can go in deep on a business domain and help bring automation to it.
This is a huge opportunity right now whether you’re doing this internally or as an external business provider.
@dp_oneill@BradSpellberg@mcuban@kevin_schulman It is already happening. Many of the patients with one of those insurers are on a self-funded plan. Every self-funded plan can have different coverage, benefits, eligibility rules, etc. In many cases the practice has someone calling the carriers all day to ask "What's the copay?"
@dp_oneill@mcuban@BradSpellberg To a large extent hospitals and practices are dealing with this already. @kevin_schulman's work has shown there are over 300k health plans in the US when you include ERISA plans. These plans get funneled through TPAs/ASOs but it still requires the provider to confirm coverage.
I don’t think people realize how much healthcare costs are driving big companies to fire and not hire.
It costs them $30k per family, per year for premiums and care. Most of that goes to the massive, vertically integrated insurance companies that send weekly bills that no one reviews in details. And it doesn’t include the company overhead to deal with it all. It’s usually the 2nd largest expense after payroll. Which is insane
It’s far easier to blame AI than it is to blame Healthcare costs.
Want to increase jobs, wages and improve affordability for every American ?
Break up the biggest insurance companies. Make divest non insurance companies. They don’t need thousands of subsidiaries. That’s how they game and abuse the system and increase costs for all of us.
Call your senator and tell them to support the BreakUp Big Medicine Bill by @HawleyMO and @SenWarren.
Want to know the craziest part about insurance company Pre Authorization Denials ?
The insurance company defines the network of providers the patient can use
When they deny care, they are effectively saying "we don't trust the judgement of the doctors we require you to use" 🤯🤯🤯
One more idea on how we can increase hospital competition - standardized contracts
IMO one of the most underrated obstacles for new hospitals is the sheer complexity of payer contracting. It’s so complex and f***ed up, you have entire departments that need to handle this. If you know what “managed care contracting” is you need to find god.
I think it could be interesting if you had way more simplified and modular contracts, especially if everyone could see them. There are some interesting experiments happening here:
- Turquoise Health has Clear Contracts and Standard Service Packages to spin up simpler contracts powered by the price transparency data.
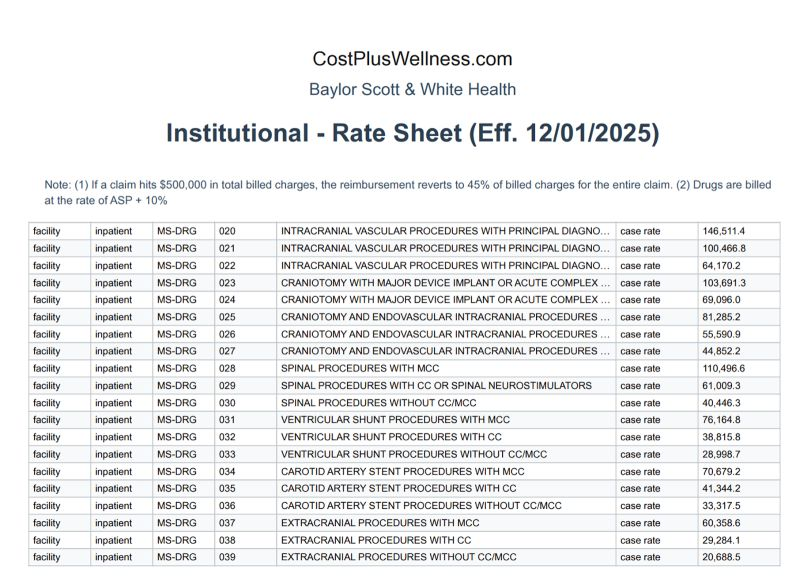
- Cost Plus Wellness has been publishing transparent contracts that they have with hospitals. There’s a big disclaimer at the top that says these are only meant to be used as a reference but…still interesting to see.
- CMS has something in the new LEAD model called CARA, an acronym matryoshka doll (CMS Administered Risk Arrangements). These are supposed to provide ACOs with shared data infrastructure, standard contract templates, and payment processing for specialist arrangements. What if CMS offered CARA-like infrastructure to new hospitals in concentrated markets? Provide standard contract frameworks, episode data, and payment rails that new entrants can plug into
❄️Reminder❄️:
City of Dallas Temporary Inclement Weather Shelters are open at Fair Park in the Automobile Building. If you or someone you know needs a warm, safe place, please come by. 🙏
In case you missed it this week, the incredible @BeckyQuick and @CNBC launched CNBC Cures — an initiative to raise awareness for the 30M Americans living with rare diseases. Hats off to Becky and Matt (my first CNBC boss!) for sharing their personal journey and fighting for a cure 💙
What is needed is a national network of providers that will offer cash pay pricing around a single standardized contract to employers and a simple to understand price list for patients. Each can charge what they choose, as they do now.
Employers will save money. Providers reduce admin costs significantly. Insurance companies will have to meet market prices for services. The game changes.
Who puts this network together ? If the hospitals are smart , they will work together to create it. Otherwise they will be looking down the barrel of fighting single payer or universal healthcare, sooner rather than later.
And if you wanna replace the ACA ? That’s also the first step.
It answers the “how much does it cost “ question.
The only 2 remaining questions are “how do you pay for the care “, and who takes the risk when patients can’t afford the cash prices.
That’s a conversation for another post
All suggestions welcome!
I know we are on the same side when it comes to PBMs. The big brands are more afraid of PBMs than what your father will do to them. They have been told if they work with @costplusdrugs, which would get low prices to patients, thePBMs will remove them from formularies, costing them 10s of billions of $.
The big PBMs control 95 pct of commercial rebates. It's insane and not an open market.
We are ready to hit those MFN prices
DEAR MOOLAH FAM: Our sales are up over 700% in the last two weeks (vs. 2024) since the NYT article and All-Star Weekend. All we can say is, thank you. We are overwhelmed with gratitude. 📈📈📈🎉🎉🙏🙏
Shoutout to @CourtMWilliams for lighting it up on court in Moolah! @mcuban
If you take Entresto, we now have the generic and it starts at $33.75 !
It's probably lower than your deductible or Coinsurance. So check it out with your doctor !
I had 4 patients that I saw in follow up that needed a joint injection.
This past week my billing dept comes to me and says “you can’t do this anymore”
I can’t do it anymore? This is fundamental care as a sports and pain doctor.
Well, we have to figure something else, because in one case they down coded the injection, denied the follow up and paid you $22. In two cases they denied you both and paid you nothing and in the 4th they denied the injection and paid you $76.
Well, we can’t afford to keep the place open if we get paid less than $100 for 4 patients and injections which by themselves almost cost that much. Maybe we can figure out which insurance does what so we can decide what they will and won’t pay?
They were all the same insurance