💥Happy to announce our new study: Time to platelet recovery was the same when transfused with platelet rich concentrate alone vs FFP and platelet rich concentrate in patients with #dengue requiring product support. Link 👇🏻
#medicine#MedX@Audrinlenin
https://t.co/PB2a0m9H5N
#ASCO26
Personalized cancer vaccines are the next frontier.
Intismeran autogene + pembrolizumab vs pembrolizumab in high-risk resected melanoma: 5-year KEYNOTE-942 update
What we are really talking about here is individualized neoantigen therapy: sequence the tumor, identify patient-specific neoantigens, manufacture an mRNA therapy, and train the immune system to recognize the cancer more effectively.
KEYNOTE-942 tested this plus pembrolizumab vs pembrolizumab alone in completely resected high-risk stage IIIB-IV melanoma.
Quick hits:
📌 Randomized phase 2b
157 patients
Intismeran + pembrolizumab: n=107
Pembrolizumab alone: n=50
💉 Treatment
9 doses of intismeran Q3W
18 doses of pembrolizumab Q3W
📈 Recurrence-free survival
HR 0.510 (holy smokes)
49% reduction in recurrence or death
⏳ Overall survival
Favorable trend
HR 0.471
🔍 Biology matters
Greater expansion of novel clones was seen in patients without recurrence in the combination arm
⚠️ Safety
Manageable
No new safety signals at 5 years
This is melanoma, not GI.
But the concept matters across oncology.
We have spent decades giving systemic therapy in broad categories: chemotherapy, immunotherapy, targeted therapy.
This is finally something new.
The practical challenges are real: manufacturing, timing, cost, access, tissue quality, sequencing, and whether this works outside highly immunogenic tumors.
But a sustained 5-year signal on top of pembrolizumab is impossible to ignore.
When can we get these products in GI? I know there are studies running now in Pancreatic Cancer, but we’re waiting in Colorectal.
Also, if we could please come up with a different name than “vaccine”? Might help with funding and rollout in the future…
https://t.co/8pnKTt9UtF
@TheGutonclab@UGrewalMD@TimothyJBrownMD@OncoAlert@Onco_Nexus@ASCO@NazliDizman@LauraAlderMD@DVAraujoMD@DrBarbiOnc@LauraEsfeller@FunchainMD@YGaritaonaindia@DrSAHaddad@jgong15@iandresmeraz@SakditadMD@RamilaShilpakar@RohitBanwar@lungoncdoc
Amazing! I’m impressed both with the results for a disease we have struggled against forever: pancreatic cancer; and the fact that we can target what we thought we could not ever: RAS.
#ASCO26@NEJM https://t.co/Hu0mRlmA9D
LBA5 #ASCO2026
Pancreatic cancer finally gets a major targeted therapy win.
RASolute 302 showed daraxonrasib (RAS(ON) inhibitor) significantly improved outcomes vs chemotherapy in 2L metastatic PDAC:
• OS: 13.2 vs 6.7 months • HR 0.40 • PFS: 7.2 vs 3.6 months • HR 0.49 • ORR: 31.6% vs 11.2%
For a disease where most targeted therapies have failed, an OS improvement of nearly 6.5 months is fantastic
Beginning of new Era ?
#ASCO26 @ASCO@dr_yakupergun@NiuSanford@GIMedOnc@GIcancerDoc@OncoAlert
Dr. @TonyMok9 at #ASCO26 presents update on CROWN in ALK+ NSCLC. After 7y, median PFS with lorlatinib still not reached. Between years 5 and 7, only 4 progression events occurred. Unusual but fantastic to see such a tail with targeted therapy - this is truly raising the bar.
After FSSAI order, Kenvue rebranded ORSL to eRZL and marketed it as new version of ORSL in violation of FSSAI order and Delhi High Court order, I have filed a Trade Mark objection to this rebranding(minor tweaking with everything else remaining the same). I have raised awareness that eRZL was not ORS, and that Sucralose containing drinks should not be given on a daily basis to children as per WHO conditional recommendation of 2023 and also as per various academies of Paediatrics . I have reached out to IAP president Dr Neelam Mohan that eRZL can still mislead ignorant parents, to ask Kenvue to rebrand eRZL not to look like ORSL which misled millions, and to ask Kenvue to not promote them as daily hydration drinks for children. Kenvue issued a public statement that their 'scientific drinks' were validated at PEDICON. KENVUE AND JOHNSON&JOHNSON PTE LTD sent me a notice accusing me of spreading unscientific information for commercial interests and views, threatening to put a defamation case against me.
I have once again asked the IAP leadership to
1. Ask Kenvue to rebrand eRZL to not look like ORSL
2. To ask Kenvue to not promote electrolyte drinks as daily hydration drinks for children
3. To condemn the notice issued to me by Kenvue and Johnson&Johnson Pte Ltd
4. To condemn the public notice issued by Kenvue that its scientific products were validated at PEDICON.
A phase started where most paediatricians were supporting the cause, but the committee formed by Dr Neelam Mohan issued a position statement on ORS and electrolyte drinks in which extra emphasis was put on the safety of Sucralose without talking about the other artificial sweeteners and without alerting the parents about the dangers of the long term effects of Sucralose like the risk of diabetes and related complications, clearly showing a conflict of interest(most IAP programmes are sponsored by Kenvue).
A phase started where paediatricians close to the leadership started spreading messages to malign my name. The biggest lie was that I had never reached out to the IAP before and that I am begging them for legal support now. I AM ABSOLUTELY NOT EXPECTING ANY LEGAL SUPPORT FROM THEM. I WAS MISQUOTED IN SOME NEWS THAT I RESIGNED BECAUSE I DIDN'T GET SUPPORT. I DID ASK THEM TO CONDEMN THE NOTICE SENT TO ME, BUT I RESIGNED BECAUSE COMPANY'S INTERESTS WERE BEING PRIORITIZED OVER CHILD SAFETY. I have each and every message and mail to all the leadership of state IAP, and to Dr Basvaraj(president 2024), Dr Vasant(president 2025), and Dr Neelam Mohan.
BASICALLY ANYTHING TO PULL ME DOWN AND TO LET THE CHILDREN SUFFER BECAUSE OF THE MISLEADING BRANDING AND MARKETING OF eRZL AS ORSL. IAP LEADERSHIP CAN'T LET GO OF THE FUNDS FROM KENVUE AND THE EB MEETINGS AT HOTELS AND ON CRUISES!
I will share with you the notice sent to me, the public notice issued by Kenvue, the IAP's position statement, and what Dr Neelam Mohan says whenever she is asked to ask Kenvue to rebrand eRZL so as not to look like ORSL, and whenever IAP leadership is requested to reach out to the Govt. to address the misbranding and misleading marketing.
Please read it and tell me if I can survive this and make it work, with 1.Kenvue still wanting to continue with the misleading branding and marketing
2. With the FSSAI giving permission to eRZL without a blink and not taking action inspite of the misleading marketing (violating the FSSAI order and the Delhi High Court 's order).
3. With the IAP leadership's position statement to suit Kenvue (inspite of the conflict of interest).
Will you continue to stand by me if KENVUE AND JOHNSON&JOHNSON PTE LTD PUT A CASE AGAINST ME? I STOOD UP FOR YOUR CHILDREN INSPITE OF THE CHARACTER ASSASSINATION, THREATS AND TROLLS! WILL YOU STAND UP FOR ME?
WILL YOU ATLEAST SHARE HOW YOUR CHILDREN WERE AFFECTED BECAUSE OF ORSL, AND HOW eRZL HAS THE POTENTIAL TO WREAK THE SAME HAVOC, AND TAG @narendramodi@MoHFW_INDIA@JPNadda
https://t.co/JUvchQ0UI5
https://t.co/chddU4WOxQ
Proton beam therapy vs IMRT for oropharyngeal cancer: Results from the phase 3 TORPEdO trial are now out in @TheLancet
☢️ No significant difference in co-primary endpoints.
☢️ Important randomised evidence on this resource-intensive technology.
@OncoAlert@NHS@ASTRO_org@ESTRO_RT
Is it sexy? No.
Is it incredibly important for how we treat patients? Absolutely 🧠🧬
For over 20 years, 6 months of oxaliplatin plus a fluoropyrimidine has been the default for stage III colon cancer, and often high-risk stage II and rectal cancer. The cost has always been cumulative neuropathy that can follow patients for life ⚡️🖐️
The SCOT trial, the largest study in the IDEA collaboration, gives us long-term clarity with nearly 6,100 patients and more than 6 years of follow-up:
📊 5-yr DFS identical with 3 vs 6 months: 72.9% vs 72.9%
📈 5-yr OS identical: 82.4% vs 82.4%
✅ Noninferiority for OS formally met for 3 months
Where this really matters clinically:
🟢 CAPOX clearly supports 3 months
🟢 Low-risk stage III shows no OS penalty
🟡 Even high-risk disease sees only tiny absolute OS differences
⚠️ Meanwhile, neuropathy nearly doubles when oxaliplatin is extended to 6 months. Many patients pay a lifelong price for minimal benefit.
SCOT also uniquely included rectal cancer patients treated with upfront surgery, and here too, 3 months held up. This fits perfectly with modern TNT strategies 🧩
Takeaway:
This isn’t flashy, but it’s foundational. For most patients with localized colon or rectal cancer, 3 months of adjuvant CAPOX is enough. Six months should be the exception, not the rule, and always a shared decision 🤝
Sometimes the most important advance is knowing when to stop.
@OncoAlert@TheGutOncLab
#GI26
https://t.co/geX09H4ltq
Proud moment for the Thoracic Oncology Multidisciplinary Team @OffCMCVellore
Our real-world study on induction chemotherapy ± low-dose nivolumab in stage III NSCLC featured among the Top Articles of 2025 in @JCOGO_ASCO
DOI: https://t.co/6cMfz2o2Cq
https://t.co/oWHxwBhGVz
#LCSM
Good morning!
The government recommend that doctors prescribe generics because they are affordable.
We already know this.
But are they effective and safe?
There is literally ZERO transparent data on this.
This is why our citizen-led Citizens Generics vs. Branded Drugs Project is going to be the game changer.
Funding for this project is ongoing and people have been extremely helpful and supportive. We have now raised approximately INR 20,00,000 for this intense project.
You can contribute or ask your friends and family to help support this project that will give us a huge amount of information on quality of major branded and generic drugs in the Indian market.
To contribute any amount, please use this link: https://t.co/6YXy2Ko6hT
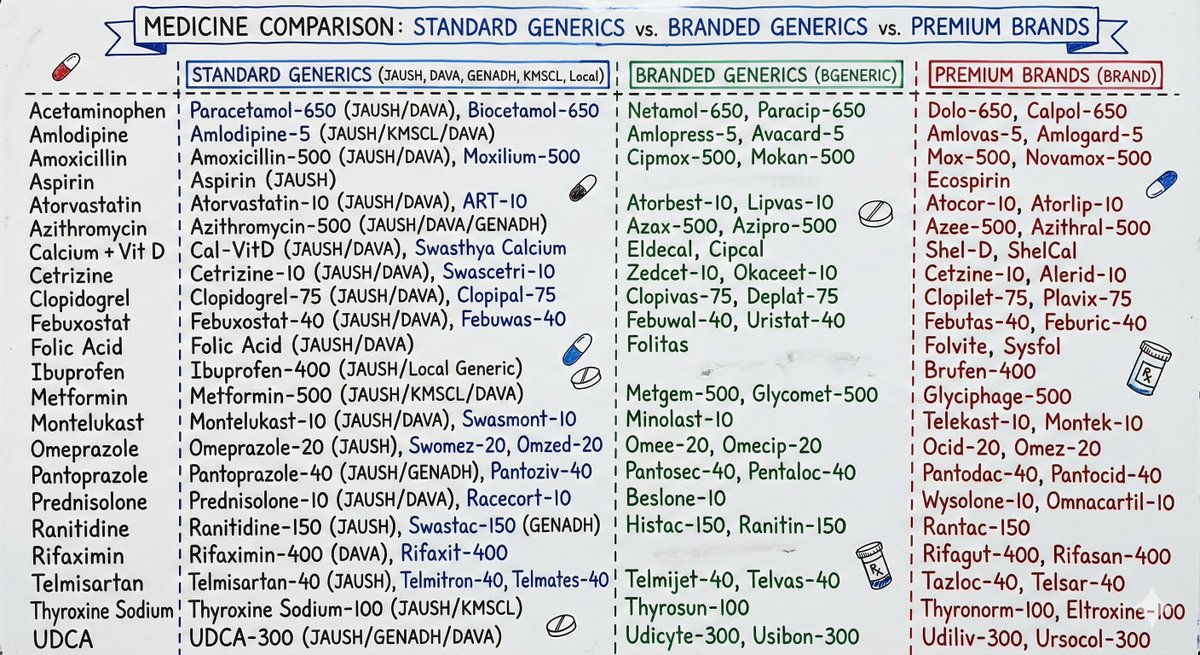
Here is a list of all the drugs we have purchased (40 numbers each) for the quality assessment! Thank you once again for keeping this fire alive and burning. Let us do it!
Key to abbreviations: JANAUSH = Jan Aushadi, DAVA = Dava India Generics, GENADH = Generics Aadhar, KMSCL = Kerala State Government Generic, BGENERIC = Branded Generics. Rest are local pharmacy available generics or proper (expensive) brands.
It has been 5 months since NEET SS 2024 Round-1 joining ended, yet MCC has not refunded the ₹2,00,000 security fee to thousands of doctors.
RTIs & emails have gone unanswered. Who gets the interest?
Requesting intervention.
@JPNadda@NMC_IND#RefundNEETSSSecurityFee
According to Globocan 2022, lip and oral cavity HNSCC is the second most prevalent cancer in India. Financial constraints limit treatment options. Affordable and effective cancer care become paramount in this setting.
#Cancer#MedTwitter#OncoDaily
🚨Out in @SciReports@NaturePortfolio our study from @OffCMCVellore@todrashish
Low-dose nivolumab + induction chemo in unresectable/loc advanced HNSCC led to 75 % ORR, 31 % conversion to resectability, ~90 % cost reduction. See below 🧵on our findings👇https://t.co/E8IfVeDjNI
Bloomberg @business (Global, NY) @RobertLangreth recently featured our work from @OffCMCVellore Medical Oncology & Haematology and @TataMemorial: low-dose immunotherapy and potential for equitable cancer care. What if 1/6th the dose works just as well?
https://t.co/CYAuvUz609
monarchE hits OS. In HR+/HER2−, node+ high-risk EBC, 2 yrs abemaciclib + ET improved overall survival vs ET alone; 7-yr landmark sustained iDFS/DRFS. Reinforces 2-yr abema+ET as adjuvant SoC. Awaiting full data, KM & hazard ratio. #monarchE#bcsm