1/Big week for Renaissance: LDRT-MIND just cleared IRB review and approval.
So I can finally talk about what we're doing, which is treating Alzheimer's disease with a new style of low dose radiotherapy.
🧵
🥇 And the award goes to a surgeon willing to lead a randomized trial of radiotherapy versus surgery (prostate cancer) that showed no difference in efficacy, and yet better quality of life with radiotherapy.
📌 Impact of Radionecrosis and Local Recurrence on Overall Survival After Stereotactic Radiosurgery for Brain Metastases 🧠
🔗 https://t.co/zLFWzoaKKY
@ASTRO_org@EJVaios@PeterFecci@MuzamilArshad18
🔹1383 pts
🔸 large, multi-institutional cohort
🔹 Patients diagnosed with LR were diagnosed sooner after SRS than RN (5.8 vs 8.3 months)
🔸 Local recurrence was associated with significantly worse OS than radionecrosis (15.2 vs 40.4 months)
🔹 Patients symptomatic from either LR or RN presented earlier after SRS than asymptomatic patients and had worse OS
🔸 On binomial logistic regression, RN was associated with single fraction SRS (odds ratio [OR] = 0.38, P = 0.012), receipt of immunotherapy after SRS (OR = 0.32, P < 0.014), and a longer interval from SRS (OR = 0.94, P = 0.028).
ASCO2026: Asymptomatic brain met EGFR/ALK NSCLC any benefit upfront cranial RT on this Randomized trial?
- Upfront RT ↑↑ brain control, no benefit PFS, OS
- Selection criteria high risk (e.g. larger size) for upfront RT is key
https://t.co/1CM31nbxeL
MIRACLE-2: RT to primary/mets -> chemo + tislelizumab in MSS unresectable met rectal ca (N=50): 68% ORR & median OS 23 mo.
Early, single-arm data, but ~1 in 5 pts reached NED.
Suggests RT + systemic + PD1 blockade could overcome immune resistance in MSS mCRC. #ASCO26@OncoAlert
Education - Metastatic #BreastCancer
Stereotactic Body #Radiotherapy for Oligometastatic and Oligoprogressive Hormone Receptor-Positive Breast Cancer: When and Why?
Steven J. Chmura #ASCO26
The story is not over @OncoAlert#OncoAlert
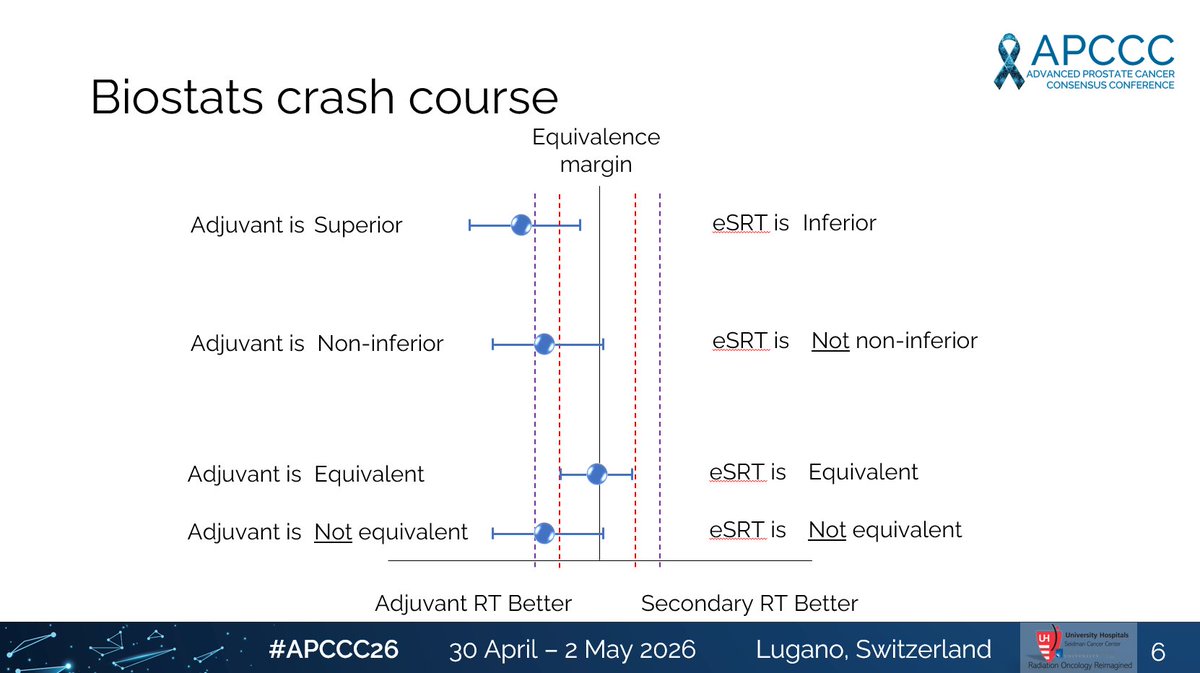
#APCCC26@APCCC_Lugano No one better to debate than @piet_ost
Is early SRT "equivalent" to adjuvant RT in high risk/locally advanced disease? Statistically, absolutely not if you believe the RADICALS-RT data.
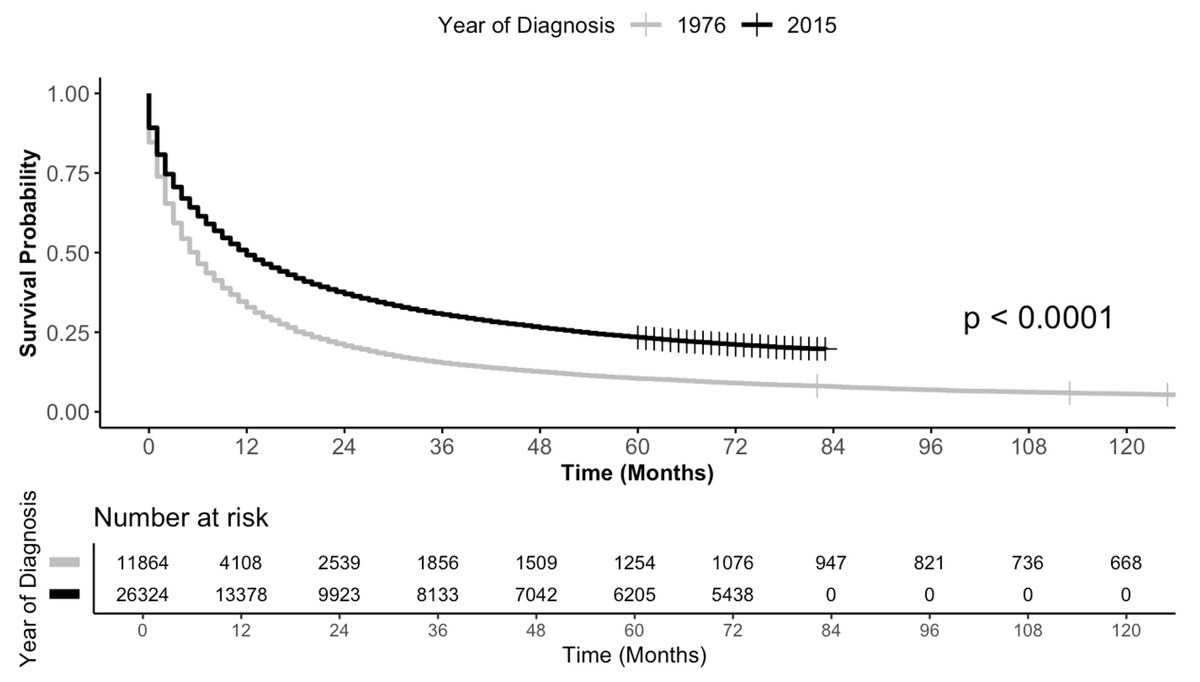
Long-term survival for patients with newly-diagnosed metastatic cancer has more than doubled ⏫in the past 40 years.
However, not all patients live longer.
https://t.co/zNg546hKcc
https://t.co/X6wTFytYPL
Work via @JCOOP_ASCO from team at @UHhospitals@CWRUSOM@MayoClinic
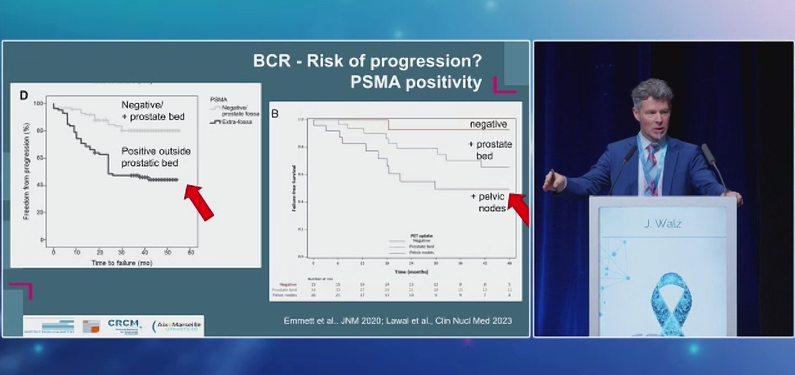
#APCCC26 Jochin Walz crushes his talk and makes the strong case why waiting until imaging is positive after RP is inappropriate and non-evidence based. Early is better!
I am thrilled to announce that Renaissance Institute completed the initial phase of its first course of LDRT for an #Alzheimers patient today.
The patient began the treatment course with a MOCA of 15, complete anosmia & ageusia, and A&Ox1.
By the end of Renaissance-modified treatment fractionation, the patient had recovered their sense of taste, was A&Ox4, able to remember my staff’s names, and MOCA improved to 19.
We look forward to opening this new & innovative fractionation scheme in the upcoming LDRT-MIND trial.
#radonc #neurology #dementia
Interesting that a review on TNT for LARC- w/ extensive discussion of RT toxicity & RT omission - has 0 rad onc authors, cites bowel tox data from 2005, and mischaracterizes PROSPECT data: no better QoL with chemo as they state, but different toxicity profile and no diff in HRQoL








![Advances_ASTRO's tweet photo. 📌 Impact of Radionecrosis and Local Recurrence on Overall Survival After Stereotactic Radiosurgery for Brain Metastases 🧠
🔗 https://t.co/zLFWzoaKKY
@ASTRO_org @EJVaios @PeterFecci
@MuzamilArshad18
🔹1383 pts
🔸 large, multi-institutional cohort
🔹 Patients diagnosed with LR were diagnosed sooner after SRS than RN (5.8 vs 8.3 months)
🔸 Local recurrence was associated with significantly worse OS than radionecrosis (15.2 vs 40.4 months)
🔹 Patients symptomatic from either LR or RN presented earlier after SRS than asymptomatic patients and had worse OS
🔸 On binomial logistic regression, RN was associated with single fraction SRS (odds ratio [OR] = 0.38, P = 0.012), receipt of immunotherapy after SRS (OR = 0.32, P < 0.014), and a longer interval from SRS (OR = 0.94, P = 0.028).](https://pbs.twimg.com/media/HJ5kvwbWUAA8cil.jpg)























![Advances_ASTRO's tweet photo. 📌 Impact of Radionecrosis and Local Recurrence on Overall Survival After Stereotactic Radiosurgery for Brain Metastases 🧠
🔗 https://t.co/zLFWzoaKKY
@ASTRO_org @EJVaios @PeterFecci
@MuzamilArshad18
🔹1383 pts
🔸 large, multi-institutional cohort
🔹 Patients diagnosed with LR were diagnosed sooner after SRS than RN (5.8 vs 8.3 months)
🔸 Local recurrence was associated with significantly worse OS than radionecrosis (15.2 vs 40.4 months)
🔹 Patients symptomatic from either LR or RN presented earlier after SRS than asymptomatic patients and had worse OS
🔸 On binomial logistic regression, RN was associated with single fraction SRS (odds ratio [OR] = 0.38, P = 0.012), receipt of immunotherapy after SRS (OR = 0.32, P < 0.014), and a longer interval from SRS (OR = 0.94, P = 0.028).](https://pbs.twimg.com/media/HJ5kvwbWcAA23SU.jpg)