When well-intended policies create unintended harm — a lesson in system dynamics.
Rating systems are designed to help patients choose better care, increase transparency, and incentivize hospitals to improve. But when you change one part of a complex system, the ripple effects can be profound — especially when reputation and reimbursement are on the line.
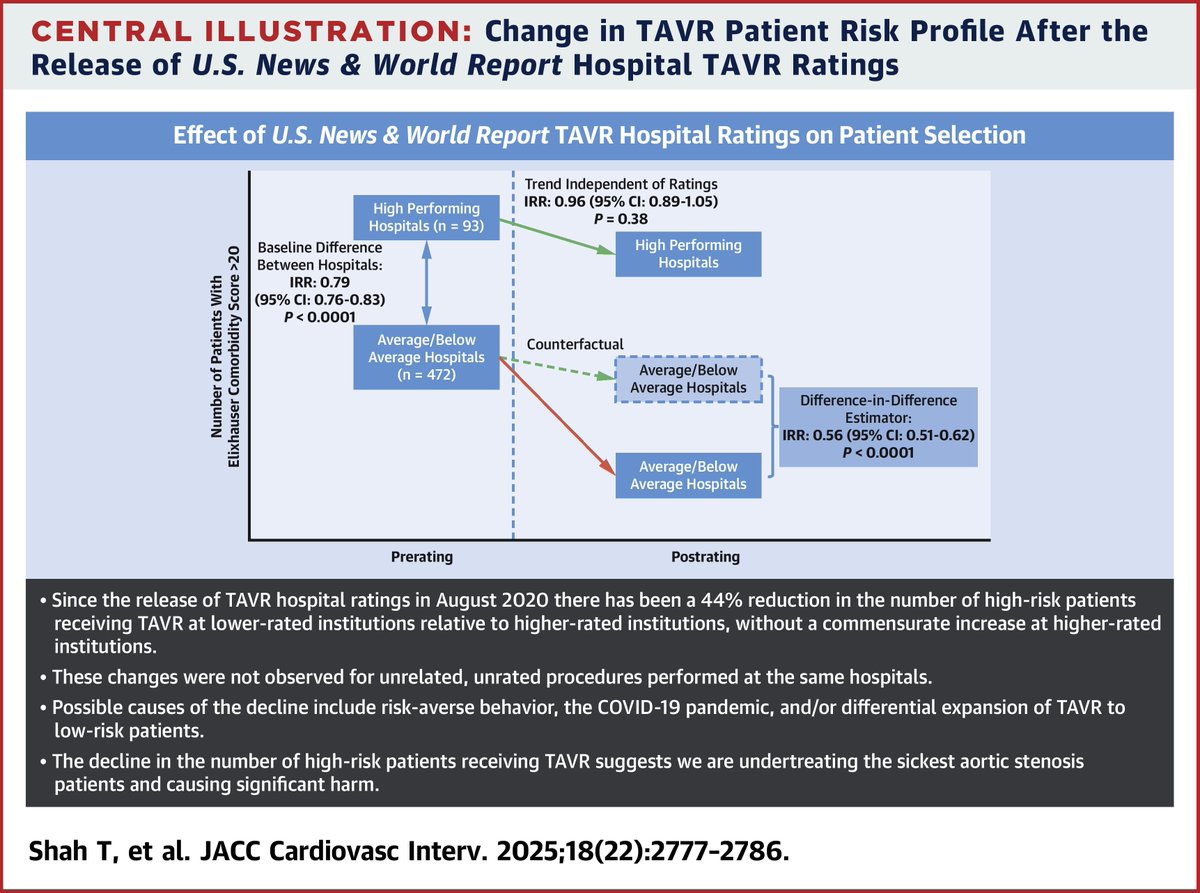
A new analysis in @JACCJournals reveals that after U.S. News & World Report began rating TAVR programs in 2020, lower-rated hospitals became significantly more risk-averse — performing 44% fewer high-risk TAVR procedures, with no compensatory increase at higher-rated centers.
This is the paradox of public ratings: a tool meant to improve care may instead discourage hospitals from treating the sickest patients, simply to protect a score.
It is a reminder that:
1. Metrics shape behavior.
2. Imperfect risk adjustment means patients — not systems — absorb the cost.
3. Those “too sick” for surgery must not become invisible casualties of policy design.
This is an opportunity to rethink and redesign — rather than to blame.
Perhaps the question should be: How do we build systems that reward treating the hardest cases — instead of penalizing them?
https://t.co/KEXJEkAZAO
(1/x) Authors have sued the six largest academic publishers for running an illegal cartel that violates US antitrust law.
Here are the key points from the biggest lawsuit in academia 🧵
Please retweet to help promote FAIR publication.
I am done letting private equity treat Pennsylvania hospitals like a piggybank they can empty out and smash on the floor.
As a Commonwealth, it’s time for us to reform the way private equity has infected our health care system.
Send a bill to my desk requiring pre-transaction notifications for all sales, mergers, acquisitions, and bankruptcy claims by empowering the Office of the Attorney General to review these intentions carefully, comprehensively, and with the community’s best interest at the forefront.
Question: why do you charge medical students with no income and no other options hundreds to thousands of dollars to use your service?
And do you realize this disproportionately affects students of lower socioeconomic means?
I don't know who has to hear this but feeling for a pulse is not necessary during CPR interruptions if several monitoring waveforms from well-functioning devices (art line/CVP/pulse ox/Swan/ETCO2) are compatible with cardiac arrest. The same holds true if waveforms suggest ROSC*
@Apple Please update iOS 17 so that people can change the default notification tone/volume. Suddenly notifications are useless if you are relying on the audible alert for something important—Nobody can hear the new tone unless it’s a quiet room.
Do You Know the Concept of Spaced Repetition for Remembering Things?
Check Out This Short Video on the Concept of Spaced Repetition
https://t.co/nws5QBZ8dQ
#RezaieStrong#SpacedRepetition#Memory
Know a rockstar medical student with an interest in point of care ultrasound??? Have them apply for the AEUS Student Ultrasound Scholarship! Details on flyer below!
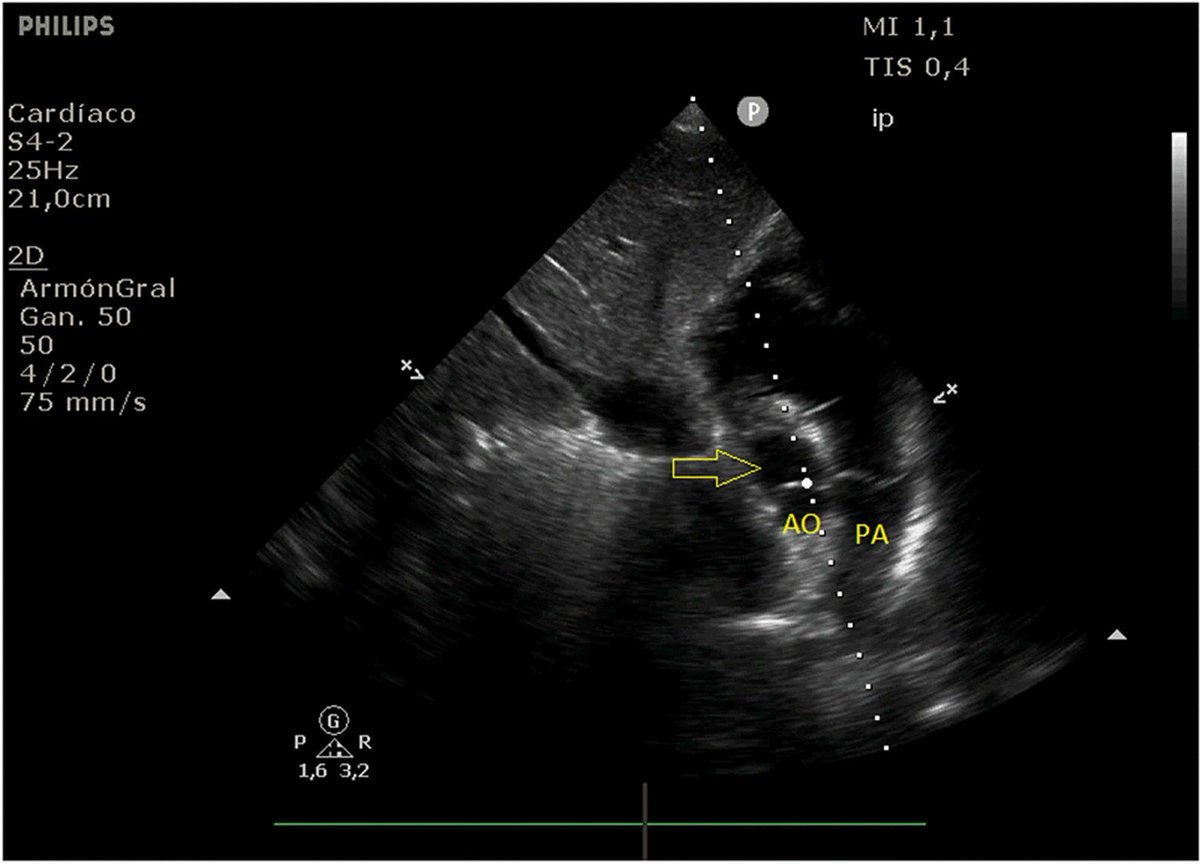
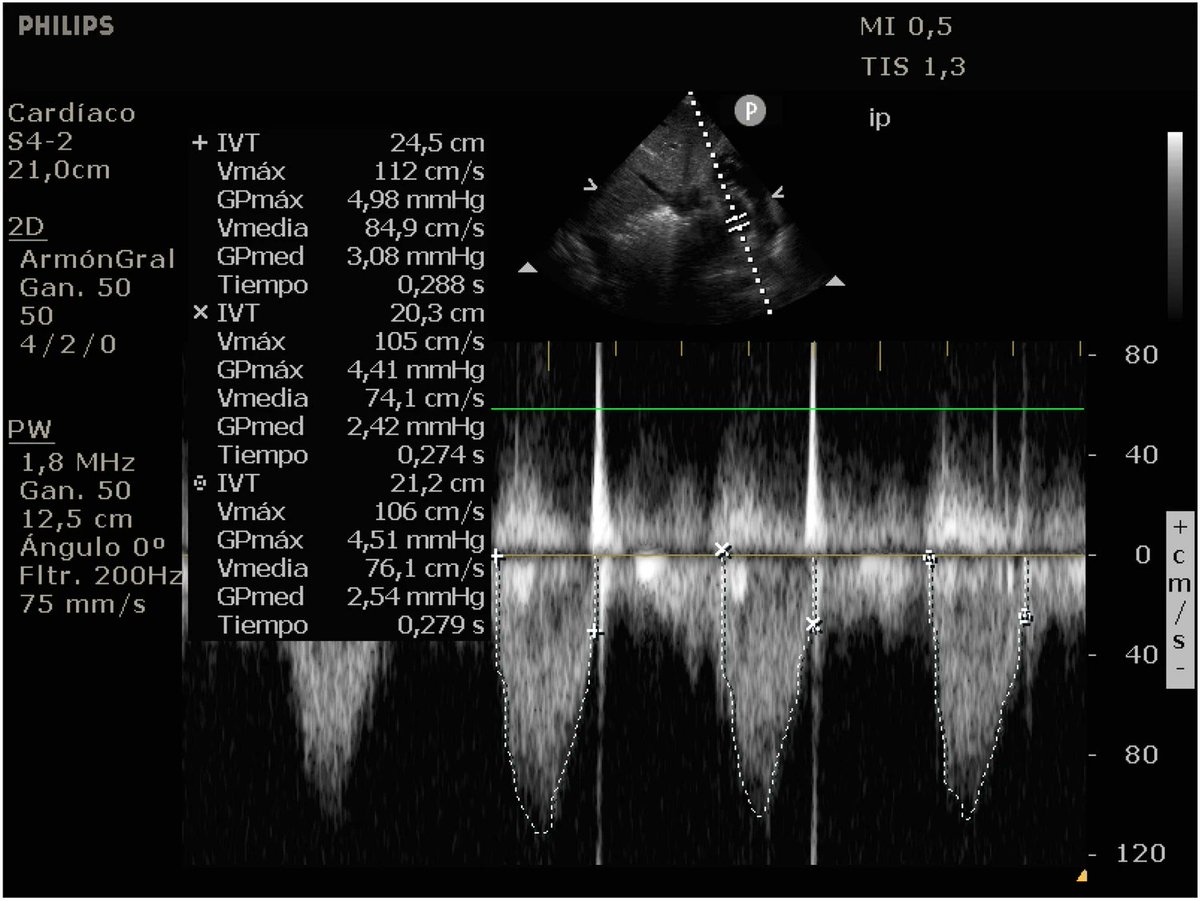
You may have heard of subcostal TAPSE, but have you heard of subcostal VTI?
#echofirst#echo#POCUS
Check it out: "A modified subcostal view: a novel method for measuring the LVOT VTI" in @JournalSiumb
https://t.co/BnlW3Tzhp7
Your patient is actively hemorrhaging and needs to go to the OR stat for a hemorrhage control intervention. They do not have a clear indication for intubation yet but are trending that direction. Do you...
(a) take control of their airway in the ED so they are all ready for surgery
(b) wait and let them get intubated in the OR 7.2 seconds before the surgeon starts cutting
This recent @JTraumAcuteSurg study from the NTDB of 9,667 patients suggests option B. Option A was associated with higher risk of death and cardiac arrest.
https://t.co/3JZGAgTtvk
#emergency #emergencymedicine #airway #surgery #surgeon #trauma #sick #blood #foamed #foamcc #science #data #research #armyemdoc #medtwitter