PTEN loss is associated with worse outcomes in prostate cancer. Now there's a way to act on it in the hormone-sensitive setting.
🎯 CAPItello-281: capivasertib + abiraterone improved rPFS in PTEN-deficient mHSPC, 33.2 vs 25.7 mo, HR 0.81. FDA approved this month, PTEN by IHC.
⚠️ The AKT inhibitor adds hyperglycemia, diarrhea, and rash, including grade 3 rash.
🏥 Plan for it: check glucose at baseline and on treatment with metformin ready, antihistamine prophylaxis for rash, loperamide early for diarrhea (onset around day 9).
Why this matters for your practice: 💡 The supportive care and counseling need to be set up early before the first dose.
What are you recommendations for handling glucose and skin monitoring for these patients? 🩺
👉CAPItello-281 full results: https://t.co/FRpQO9hmJO
#ProstateCancer #GUOnc
🎗️ 27 Days Until #BrachytherapyAwarenessDay
🔰 Image-Guided #Brachytherapy
🖥️ MRI
📡 CT
🔍 Ultrasound
👁️ See the tumor.
🎯 Treat the tumor.
➡️ Maximum dose to the tumor
➡️ Minimum dose to healthy tissues
🛡️ Organ preservation
😊 Better quality of life
📈 Excellent tumor control
🌍 Precision is not the future.
🚀 It is already here.
#Interventional_Radiotherapy #ThisIsBrachytherapy #ImageGuidedRadiotherapy #PrecisionMedicine #RadiationOncology #ThisIsBrachytherapy
📢 New publication in European Urology
We are pleased to highlight a new study published in European Urology, titled “Circulating Tumour DNA Positivity Predicts Shorter Survival for Patients with High-grade pT1 Urothelial Bladder Carcinoma”.
👏 Congratulations to Faisal Bin Humaid, Goel A., and Bryan R. on this excellent contribution, together with all co-authors.
🔗 Read the full article here:
👉 https://t.co/bPA7QAjpNu
#EuropeanUrology #Urology #UroOncology #Research #MedicalResearch #AcademicUrology
Discussion #EAU26 about the future of cystectomy neoadjuvant treatment and radiotherapy in muscle invasive bladder cancer. Things are changing rapidly. With pCR rates >50% for EVP many patients will want to keep their bladders. An era of ‘EVP 1st and ask questions later’ maybe a reality soon. Generation of EVP bladder sparing data is a priority. @Uroweb@EUplatinum
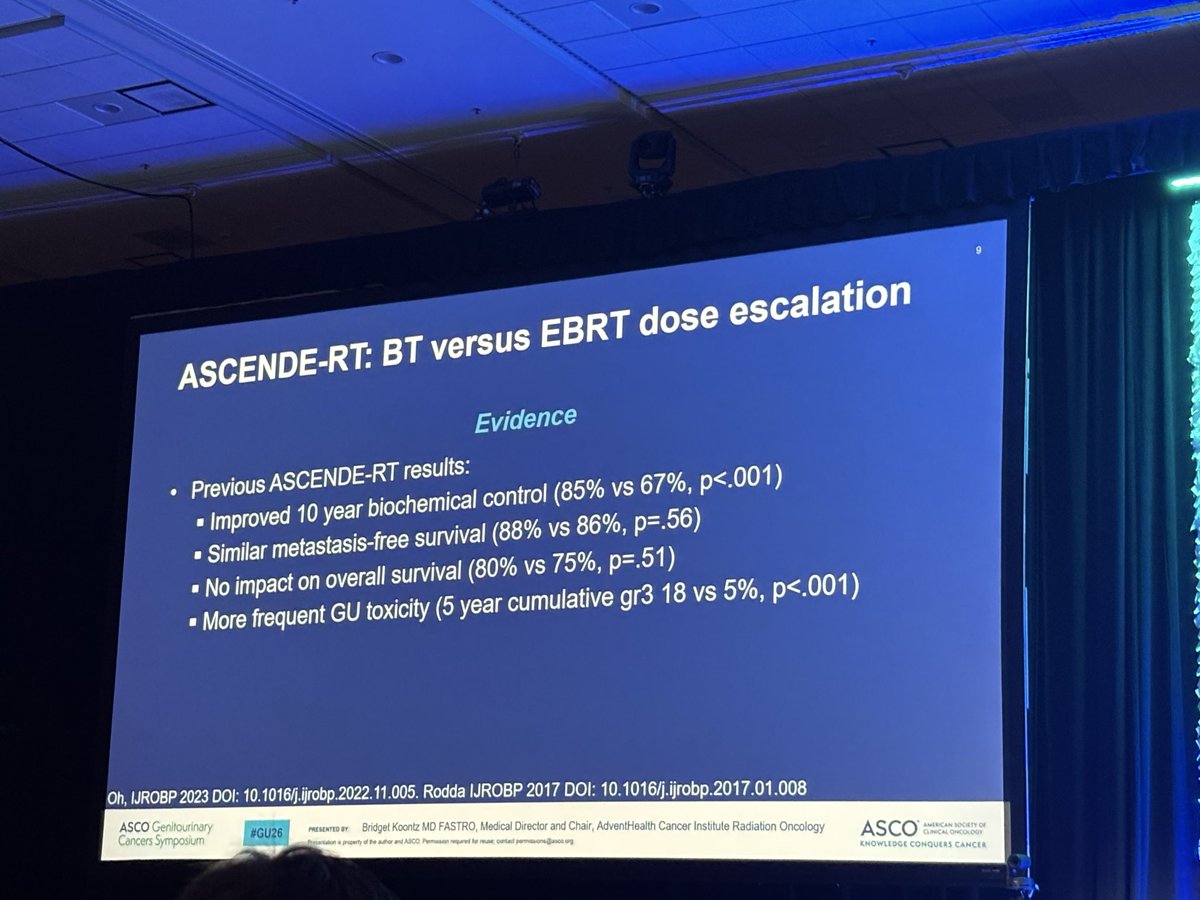
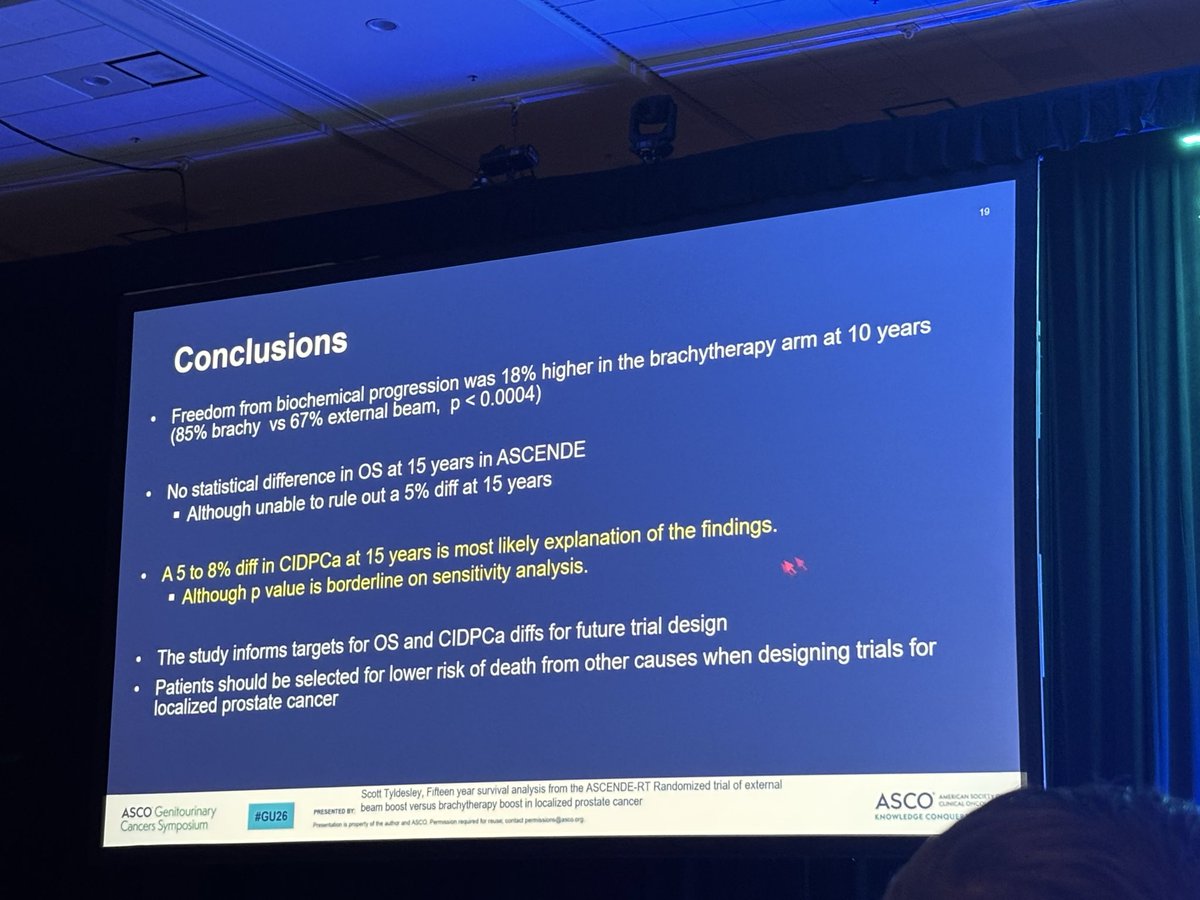
Calling all Brachytherapists, 15 year results from ascende RT presented by #scotttyldesley showing continued biochemical PFS, no OS benefit but benefit in prostate cancer specific deaths. @AmericanBrachy@ASTRO_org
💥 “Screen or not to screen?”
After 23 years, ERSPC finally answers.
📊 ERSPC (n = 162,236 men, 55–69 yrs)
🔹 Screening: repeated PSA testing
🔹 Control: no screening
⏱️ Median follow-up: 23 yrs
🎯 Results
🧬 ↓ Prostate cancer mortality: 1.4% vs 1.6% (RR 0.87 [0.80–0.95])
➡️ 13% relative & 0.22% absolute risk reduction
📈 NNI = 456 | NND = 12 → better harm–benefit ratio
⚠️ Overdiagnosis: +27 extra cases / 1000 men (mostly low-risk)
🧩 Who should be screened?
✅ Men 50–69 y with ≥15 y life expectancy
✅ Earlier (40–45 y) if BRCA2+, family history, or African ancestry
🚫 Stop if >70 y, frail, or PSA < 1 ng/mL at 60 y
💡 Takeaway:
PSA screening saves lives - just not everyone’s.
Target the right men, at the right age, using risk-based + MRI-guided screening.
📖 Roobol MJ et al. NEJM 2025
🔗https://t.co/msFgNpODRI
#OncoTwitter #MedTwitter #ProstateCancer #Screening #ESMO25
@OncoAlert@myesmo@esmo_open@ASCO@NEJM@Uroweb@AmerUrological@UrologyTimes@EUplatinum
BART Trial Presented at #ASTRO25: Adjuvant RT after cystectomy + chemo in MIBC #bladdercancer improves survival with no excess grade ≥3 toxicity
One of the first large randomized trials to show meaningful pelvic relapse reductions, says @VedangMurthy
🔗 https://t.co/bvQtwoXBpu
✍️ Editorial in European Urology:
In the PROBASE trial, 26% of significant prostate cancers in men 45–50 would have been missed with MRI-targeted biopsy alone.
👉 Stabile & Nordström argue systematic biopsy remains essential for young men.
🔗 https://t.co/FS02DWTQQz
We chose the theme of One Voice for our inaugural year of World Radiotherapy Awareness Day because we want everyone working in the field to join together and speak up for the millions around the world who do not have access to safe, high-quality radiotherapy.
🎯 Early detection saves lives. This #ProstateCancerAwareness Month, we’re proud to spotlight ABS member, #radonc & #navyvet Dr. Bear, who’s bringing high-dose #brachytherapy to @PalomarHealth offering faster recovery & precision care close to home. https://t.co/T4M4SNzvNB
📢 New in European Urology:
SABR is not just for brain mets. A systematic review shows excellent results in RCC—alone or with IO.
🧠 Local control in primary RCC
🛡️ Delay of systemic therapy in oligomets
⚡ IO + SABR: promising combos
🔗 https://t.co/pQ0xuUEOwY
#RCC#SABR #Immunotherapy #UroOncology
One day, oncology guidelines will start with: ‘First, listen to your patient.’ Then the algorithms, biomarkers, and p-values will follow.
It will be beautiful.
🚀 Why Radiation Oncology Needs to Stop Playing Defense and Start Playing Offense
I recently wrote a post on entrepreneurship across medical specialties, and the findings were eye-opening. While dermatology, radiology, and cardiology have robust entrepreneurial ecosystems driving innovation, radiation oncology remains surprisingly conservative despite being one of the most technologically sophisticated fields in medicine.
Here's the uncomfortable truth: We've been playing defense for too long.
While we've focused on protecting our traditional scope of practice, other specialties have been playing offense. Dermatology has expanded into oncology with superficial treatments. Urology has embraced advanced technologies and minimally invasive approaches that sometimes compete with our traditional treatments. Meanwhile, we've watched from the sidelines. We have even cannibalized ourselves with competition between protons and photons.
Sometimes the best defense is offense.
It's time for organizations like ASTRO and ACRO to actively champion entrepreneurship within our specialty. We need:
✅ Business education integrated into residency training
✅ Innovation incubators within academic centers
✅ Regulatory guidance for bringing new technologies to market
✅ Mentorship programs connecting clinicians with entrepreneurs
✅ Support radiation oncologists that are bringing innovation to the field
✅ Risk-sharing models that make innovation accessible.
The opportunity is immense: We sit at the intersection of AI, precision medicine, advanced imaging, and robotic systems. Our field has the potential to lead healthcare innovation, not follow it.
📢🗣️ New trial analysis from #FASTRACKII: in kidney cancer, SABR ⬆️ efficacy and ⬇️ cost than radiofrequency or cryoablation #kcsm#radonc
🔹 QALYs: SABR 4.00 vs RFA/CA 3.07
🔹 Cost: SABR A$31,053 vs RFA A$35,001 vs CA A$36,356
🔹 Net savings ~$4K/patient
https://t.co/2NoT7g94EP
Brachytherapy is an excellent treatment for prostate cancer which is organ preserving and highly effective. If you have been diagnosed with prostate cancer make sure you have all your options discussed including #brachytherapy for your own personal best outcome. #prostatecancer
#americanbrachytherapysociety
X-torial: Cleaning up the misinformation about @JoeBiden and #ProstateCancer that I am reading everywhere.
The purpose of this is to provide education from someone who treats and studies PCa for a living, lead the USA @NCCN PCa guidelines, hold leadership in @NRGonc@theNCI@US_FDA and dedicated my career to help men and their families suffering from PCa
@nytimes@WSJ@FoxNews@CNN@NBCNews@Reuters@ASCO@PCFnews @DeptofDefense
KEYNOTE-641 & KEYNOTE-991 in Prostate Cancer
What happens when you combine immunotherapy (pembrolizumab) with androgen receptor inhibitors (enzalutamide) in mCRPC & mHSPC?
Let’s break down 2 major negative trials that teach us important lessons.👇
⸻
🔬 KEYNOTE-641:
📍 Population: Chemotherapy-naive mCRPC
🧪 Arms:
•✅ Pembrolizumab + Enzalutamide
•🔲 Placebo + Enzalutamide
🎯 Endpoints: OS & rPFS
🧾 Results:
❌ No OS benefit (24.7 vs 27.3 mo; HR 1.04)
❌ No rPFS benefit (10.4 vs 9.0 mo; HR 0.98)
📉 Trial stopped early for futility
⚠️ More Grade ≥3 AEs (31.2% vs 10.8%)
🚨 Rash & immune toxicity higher
https://t.co/6nFINNiZjV
⸻
🔬 KEYNOTE-991:
📍 Population: Next-gen hormonal agent–naive mHSPC
🧪 Arms:
•✅ Pembrolizumab + Enzalutamide + ADT
•🔲 Placebo + Enzalutamide + ADT
🎯 Endpoints: rPFS & OS
🧾 Results:
❌ No rPFS improvement (HR 1.20; P = 0.95)
❌ No OS improvement (HR 1.16; not statistically tested)
⚠️ More Grade ≥3 AEs (61.9% vs 38.1%)
🚨 Rash (25% vs 9.3%) prominent
📉 Trial also stopped for futility
https://t.co/camcMYPn8T
⸻
🧠 What do these trials teach us?
1️⃣ Immunotherapy (PD-1 blockade) does not improve outcomes in unselected mCRPC or mHSPC
2️⃣ Combination with enzalutamide leads to increased toxicity, especially rash
3️⃣ Not all solid tumors benefit from immunotherapy — biomarker selection is key 🔍
⸻
💡 Bottom Line:
Checkpoint inhibitors should not be used routinely in unselected prostate cancer patients.
We must move towards biomarker-driven immunotherapy in prostate cancer 🧬
⸻
🧪 Both KEYNOTE-641 and 991 remind us:
🚫 More drugs ≠ better outcomes
✅ Precision > empiricism
@NeerajAIIMS@scottdehm@prostatecell@DrSpratticus@DrAndrewLoblaw@DrChoueiri@urotoday@DrRosenbergMSK@BradMcG04@DrKarineTawagi@DrRanaMcKay@MattGalsky@BhardwajLab@sonpavde@nataliagandur






























![DrRishabhOnco's tweet photo. 💥 “Screen or not to screen?”
After 23 years, ERSPC finally answers.
📊 ERSPC (n = 162,236 men, 55–69 yrs)
🔹 Screening: repeated PSA testing
🔹 Control: no screening
⏱️ Median follow-up: 23 yrs
🎯 Results
🧬 ↓ Prostate cancer mortality: 1.4% vs 1.6% (RR 0.87 [0.80–0.95])
➡️ 13% relative & 0.22% absolute risk reduction
📈 NNI = 456 | NND = 12 → better harm–benefit ratio
⚠️ Overdiagnosis: +27 extra cases / 1000 men (mostly low-risk)
🧩 Who should be screened?
✅ Men 50–69 y with ≥15 y life expectancy
✅ Earlier (40–45 y) if BRCA2+, family history, or African ancestry
🚫 Stop if >70 y, frail, or PSA < 1 ng/mL at 60 y
💡 Takeaway:
PSA screening saves lives - just not everyone’s.
Target the right men, at the right age, using risk-based + MRI-guided screening.
📖 Roobol MJ et al. NEJM 2025
🔗https://t.co/msFgNpODRI
#OncoTwitter #MedTwitter #ProstateCancer #Screening #ESMO25
@OncoAlert @myesmo @esmo_open @ASCO @NEJM @Uroweb @AmerUrological @UrologyTimes @EUplatinum](https://pbs.twimg.com/media/G4gejGFaQAEVasz.jpg)



































