Looking for a colleague! We have a vacancy for a gastroenterology consultant to join our vibrant team in one of the most beautiful parts of England.
Cornwall is great for family life but is no walk in the park. We need a “jack of all trades” gastroenterologist to manage a diverse and intellectually stimulating caseload, but with opportunities to sub-specialise.
Please spread the word and get in touch if interested.
https://t.co/W4D8gE6L6N
Musculoskeletal injury was common among surgeons: 22% reported changing operating responsibilities because of injury, and 59% reported that ergonomic pain affected their ability to work as a surgeon. https://t.co/pwEqwgQIz3
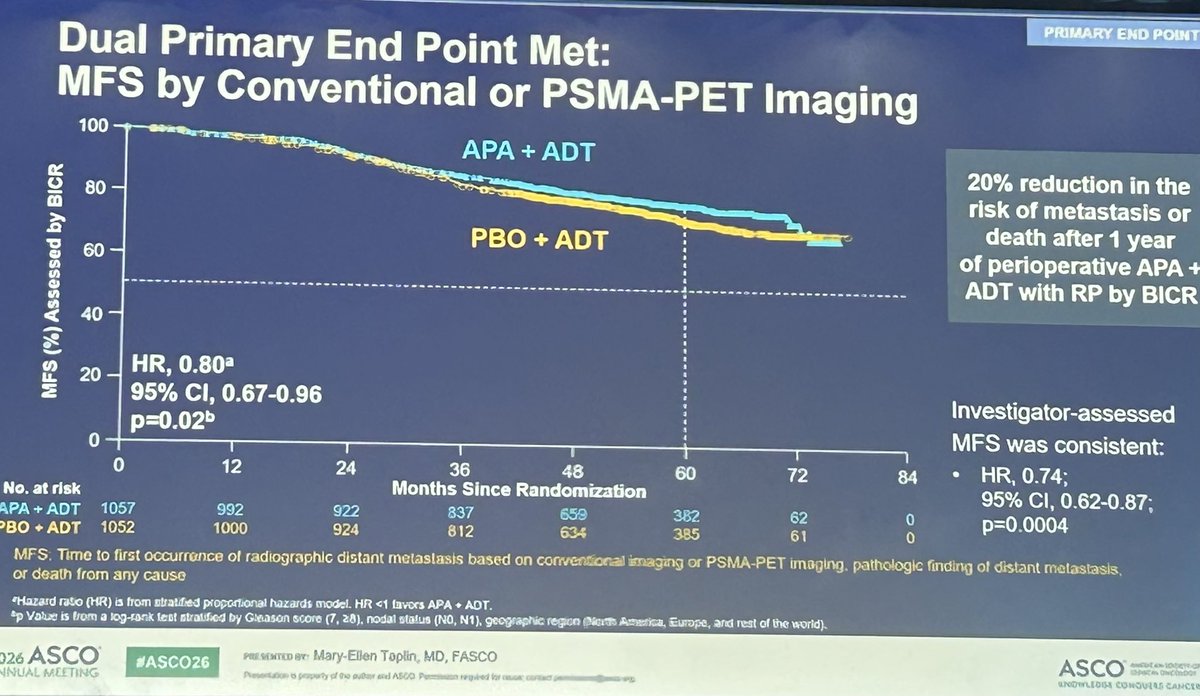
Finally #PROTEUS (#MyBaby) presents results. Significantly improved outcomes reported by Mary-Ellen Taplin for #neoadjuvant/perioperative treatment with #Apalutamide prior to #RadicalProstatectomy
PCR/MFS (+based on #PSMAPET), Time to subsequent treatment, to distant mets significantly improved
#ProstateCancer #ASCO2026
Let's watch this complete #MiniPCNL of a 2.4 PUJ stone that migrates into the kidney.
Complete surgery with no edition of the 0-90 simplified technique perc tract and complete lithotripsy from start to end.
#MiniPCNL is a great way to treat stones with no risk of bacteremia.
I hope to improve my english little by little
@RomanCarvajal@urobraulio@Endo_Society #UroSoMe
Dr @UroDocAsh has explained what does this mean :HR 0.68 = a 32% relative risk reduction in recurrence at any given moment during follow-up, please read this thread
People have been DM and asking me: with an HR of 0.68 for durvalumab + BCG in POTOMAC, why isn’t this for every high-risk NMIBC patient?
Here’s how hazard ratios work – and why they can mislead you if you stop there. 🧵 #ASCO26@tompowles1@WesKassouf@shilpaonc@DrFelixGuerrero
The approval answers one question, but leaves another unanswered: which patients truly derive enough benefit to justify escalation beyond optimized BCG?
The FDA approval of durvalumab plus BCG in high-risk NMIBC was driven by a meaningful improvement in disease-free survival (HR 0.68), mainly recurrence free survival. Checkpoint inhibitors are not benign therapies, carrying ~ 15% risk of serious treatment-related adverse events.
At the same time, this trial also demonstrated that patients with BCG-naïve high-risk NMIBC have low rates of progression and bladder cancer mortality, when treated with BCG appropriately.
For many patients, the balance between reducing recurrence and exposing them to potentially significant toxicity is not straightforward.
That raises a practical question: who should actually receive treatment intensification?
Durvalumab + BCG is FDA approved in high risk NMIBC , by hitting its DFS - HR 0.68 (plus a ~⬇️ cystectomy rate). OS & M1 data show these patients have low cancer mortality & IO has about a 10% chance of serious side effects. Therefore, this is not a treatment for all HR NMIBC IMO. It’s hard to know who to select. Inconsistency with other data for Sasanlimab + atezo means there is no subset that consistently benefits. It will be interesting to see whom urologists recommend for treatment. #ASCO26 https://t.co/12cmVfA6Rl
Some of the best ideas - including in science and medicine - do not emerge in a conference room.
They happen while walking hallways, moving between clinical duties, or talking side-by-side with colleagues.
Not every critical meeting belongs around a table.
Renal cancer highlights #ASCO26 1) RAMPART - adjuvant durva/tremi vs durva vs surveillance. How much does CTLA4 help? 2) Is ctDNA useful post surgery in RCC (KN565 data)? 3) Does radium-223 help in bone mets patients? (a RII study) 4) Data on 2 VEGF+PD1 combination single arm studies in papillary RCC.
Time to revisit something I’ve been saying for years: TaHG bladder cancer is not intermediate risk. The clinical outcomes, molecular biology ... all point in the same direction.
Yet some frameworks allow < 3cm TaHG tumors to be downgraded into “intermediate risk” alongside low-grade disease.
That classification has real consequences for patients:
• undertreatment
• less rigorous surveillance
• in some studies, these patients are even placed on observation as a supposedly appropriate “control arm.”
TaHG is high risk. 🧵 @BladderCancerUS@WorldBladderCan@IBCG_BladderCA
I’ve created a dedicated Surgical Video Library at https://t.co/i1ZpZkmjXj
Patients and colleagues frequently ask for specific videos from my procedures. Rather than searching through YouTube, this AI-powered site allows easy keyword search across my entire collection. I can also edit and update content directly.
Feedback welcome. @AmerUrological@SocietyGURS@SocietySURS
One-Handed Needle Control
👉One-handed push-and-pull motion guides the needle smoothly.
👉Gentle rotation and precise needle-driver control allow subtle adjustment of the needle direction.
👉A simple drill for refining needle advancement without forceps support.
Pleased to announce the launch of the Mentorship Programme @Uroweb,your next step starts here: register either as a mentor or a mentee and expand your Network that can help shape your clinical, academic, and leadership journey 🤓 @eau_yuo@JLVasquez82 https://t.co/8GiEvf6dYv
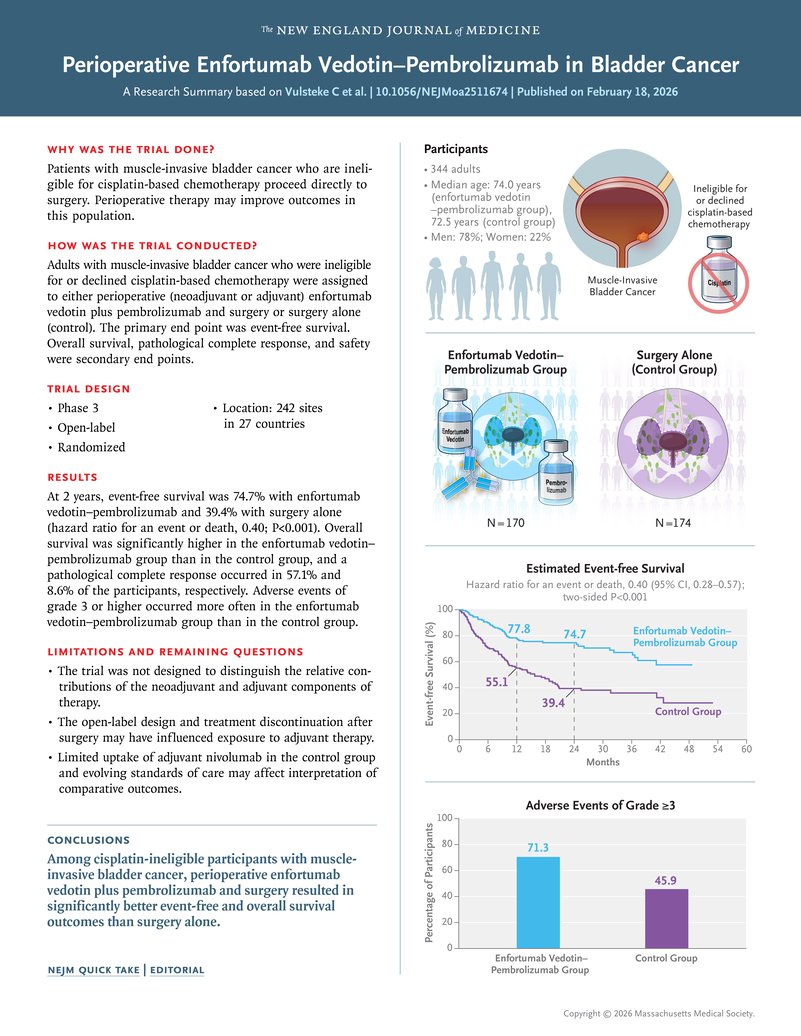
⚡️ KEYNOTE-905 published in @NEJM: perioperative enfortumab vedotin + pembrolizumab vs surgery alone in cisplatin-ineligible MIBC (n=344).
2-year EFS: 74.7% vs 39.4% (HR 0.40)
2-year OS: 79.7% vs 63.1% (HR 0.50)
pCR: 57.1% vs 8.6%
The trial that supported FDA approval in November 2025 — now with full data.
https://t.co/3FsYt3ZuEJ
#BladderCancer
Exciting news for the #Endourology community! 🩺✨ We are pleased to share the first summative work focusing on the importance of Fluid Management in ureteroscopy when using suction. #FansofFANS
In just a few years, we’ve seen incredible milestones: 🔹 2024: #FANS revolutionized fragment removal and #ZRFSFR, impacting over a million surgeries globally in its first year.
🔹 2025: The focus turned to measuring and monitoring Intrarenal Pressure (#IRP) in daily practice. 🔹 2026: We are entering the era of Automated Fluid Management.
This new reference paper is a comprehensive guide on why automated fluid management matters and how it fundamentally changes: ✅ Lasing Strategy (pedal time & duration) ✅ Intrarenal Thermal & Pressure controls ✅ Aspiration Efficiency (improving scope withdrawal & the pull-back effect) ✅ Patient QOL & Sepsis Prevention
We also introduce game-changing new concepts like the Suction-Irrigation-Ratio (SIR), SIPS (Suction Irrigation Pressure Autoregulating Systems), and Dynamic Stone Extraction (multiple fragments per extraction!).
👇 Check out the breakthrough research here: DOI: 10.1097/MOU.0000000000001411
@steffiyuen@jl_kwok@endouro@Uroweb@CAU_URO@asiaendouro@filialendouro@Endo_Society@UroAcademic@young_endosoc@Endo_Sec_Eua@usioffice@EAU_YAUroTech@Uro_News@UrologyTimes@AmerUrological
#Urology #MedicalResearch #fURS #Surgery #PatientCare