Important paper for all PFA users!🚩
PFA-PVI may look successful—but tiny signals matter.
Residual tiny PV potentials ≥0.03mV ⚡️on high-res mapping predicted 1-yr AF/AT recurrence + late PV reconnection (81% spatial concordance).
Do not miss tiny signals.🔍
https://t.co/MbT8cqZ5ZK
@masudamasaha@hrs_journal
#EPeeps #PFA #AFib
Open access books can be downloaded using this QR code. Content also appears weekly in @JACCJournals Thank you to @HRSonline for making this a special annual component of HRS for all EP’s.
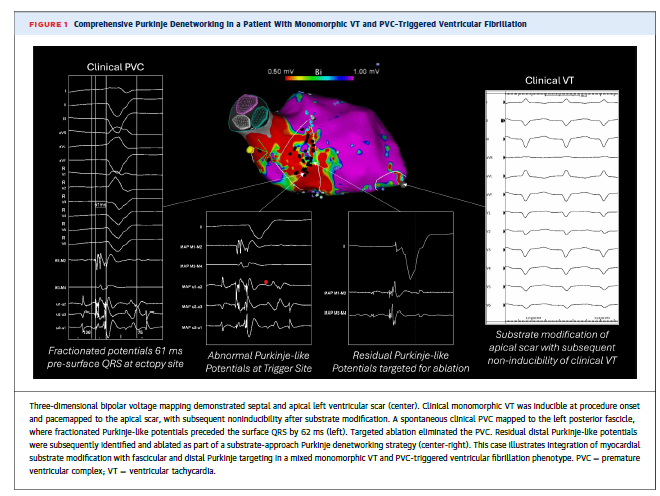
Adjunctive Purkinje Denetworking at the time of ablation led to improved VT/VF-free survival in VT patients with a history of shocks for PMVT/VF. Pardigm shifting approach.
Free read through this author share link:
https://t.co/lCN5O1JRPK
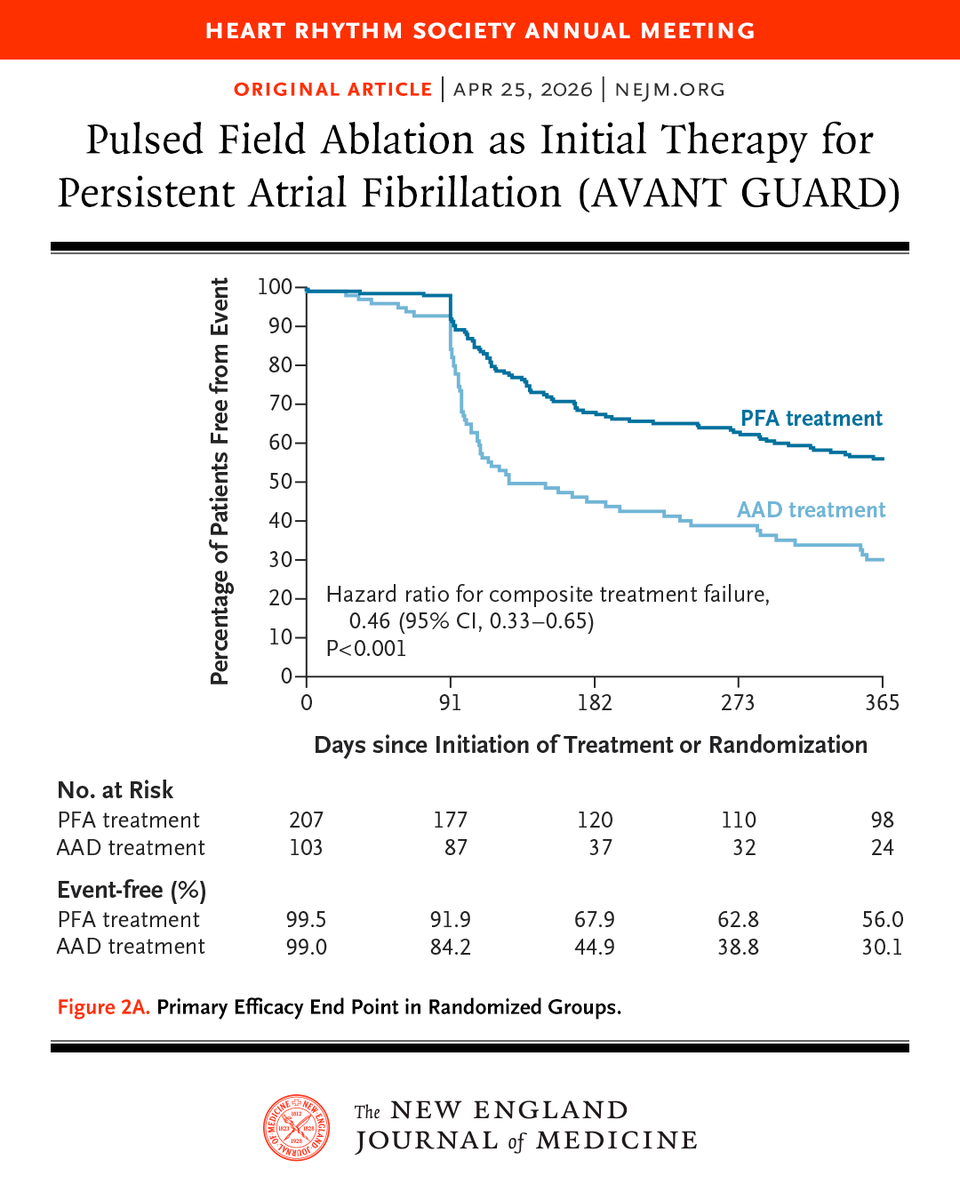
Presented at #HRS2026:
In patients with persistent atrial fibrillation, first-line treatment with pulsed field ablation reduced the recurrence of atrial arrhythmias at 12 months as compared with antiarrhythmic drugs. Full AVANT GUARD trial results: https://t.co/milHy26ojJ
@HRSonline
6/6
Risk factors for adverse psychological reactions from wearables:
🔴 25–45% of AF patients have anxiety/depression
🔴 430+ commercial wearables with inconsistent accuracy
🔴 Jan 2026 FDA change: BP, glucose, SpO2, HRV devices can skip premarket review if marketed as “general wellness”
🔴 No clinical guidelines for managing wearable data in cardiology clinics
The greatest problem in healthcare ? Hospitals, even market dominant hospitals, won’t walk away from the big ins companies that underpay, late pay, clawback, deny claims, waste their time in denial appeals, and require them to pay up to 8 pct of revenue to RCM consultants so they think they are getting what they are owed.
Here is the crazy part. The ins companies ARE NOT THE ONES ACTUALLY PAYING THEM on commercial plans. Employers are.
60 pct of employees get their insurance from their self insured employers. The ins carrier is just a middleman that pretends to add value.
All the clinical “value” they add, the hospital could do better, for both medical and pharmacy.
Most hospitals have no idea whether they make or lose money with their big ins contracts. They are just afraid to lose patient flow.
But. They actually know which companies their patients are coming from. They actually know or can find out, how much more the employers are paying the ins company, than what the ins company pays them (the spread, just like in pharmacy )
And to make it worse, those ins companies negotiate their rates as a discount from the “charge master “, which is like WAC in pharmacy. Just a made up list price.
Because the hospitals are afraid or too uninformed to walk away from these deals, the hospitals use the inflated charge master prices as the basis to charge uninsured , or out of network , or insured but not covered for their care, at charge master rates. Which of course the patients can’t afford. And it crushes their finances or they go without care
I’ll summarize. Employers , and their members , are paying far more than they should to companies they don’t like working with , that effectively rip off both the employer and hospital , and they could eliminate the middlemen if they went directly to to the employer.
It’s so simple. Sell your services to the employers that use your services at a price that is less than what nine companies charge for your services and you will make MORE money and employers will save a ton
And if they did this, they could dump the chargemaster and reduce the price they bill patients when they are at their most vulnerable
But they don’t want to change. And don’t get me started on how much hospitals over pay for drugs and devices because of the GPO deals they do. It’s just stupid.
Which in turn leads to the hospital being a bad actor with 340b , facilities fees and afraid of their doctors who demand they pay more for things like glue and implants so they can get vacations.
If you are a politician and reading this. Now you know why this is so fucked up and it’s not about capping rates. The insurance companies are smarter than you. They will just move the money to other places. It’s not about giving money to patients. You can’t shop for care from hospitals that are too gutless to walk away from the ins companies that distort all of healthcare economics
Go to your local hospitals , particularly those at risk of closing and ask for their profitability by carrier. Fully burdened. Ask how much they spend on RCM and consultants. In many cases they could survive if they ran like a real business and hired execs that could do the work rather than just manage consultants. They could work out contracts in their communities rather than with ins companies and benefit everyone.
The middlemen are not needed. Get rid of them
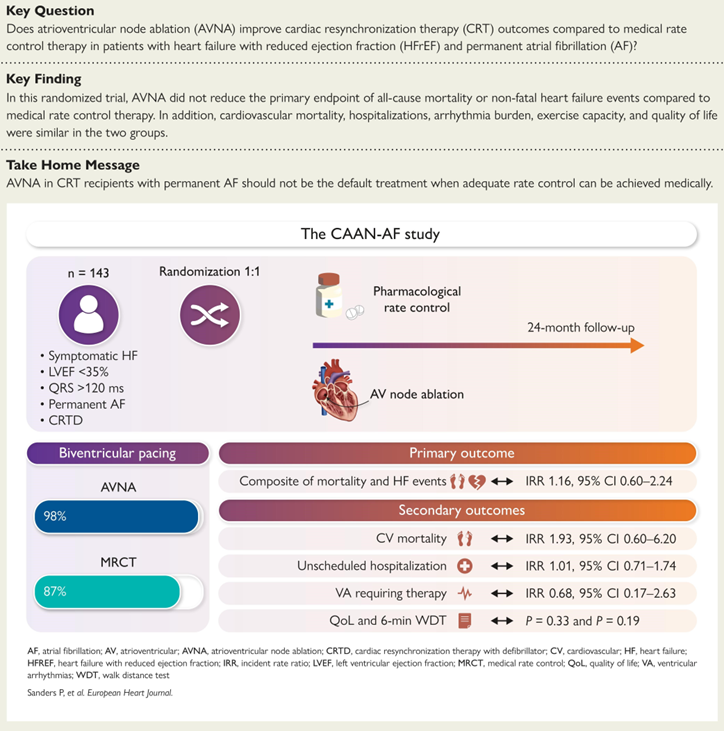
CAAN-AF Trial #CHRD@adelaide87018
Our previous meta-analysis of observational studies suggested CRT patients with AF had a significant 58% reduction in all-cause mortality with AV node ablation - https://t.co/rLbkUhqZLX
We designed the CAAN AF Trial supported by the @nhmrc and critical industry partners - in order of support @bostonsci@AbbottNews@Medtronic@MicroPort - Methodology paper - https://t.co/kZrLVV9G9q
CAAN AF Trial: https://t.co/bMIaH2CPHV
RCT showing no benefit in the routine use of AV node ablation
Important for everyone taking care of patients with Atrial Fibrillation. Our work in @CircAHA showing substantial cost savings for patients getting dofetilide through @costplusdrugs. This system needs to be fixed.
https://t.co/jtlFgi5xco
@mcuban@PennCVFellows@CardioNerds
Exercise Capacity and Quality of Life Improvements After Catheter Ablation in Patients with Clinically Asymptomatic Persistent Atrial Fibrillation #OpenAccess
https://t.co/n6A4ZQlTWQ
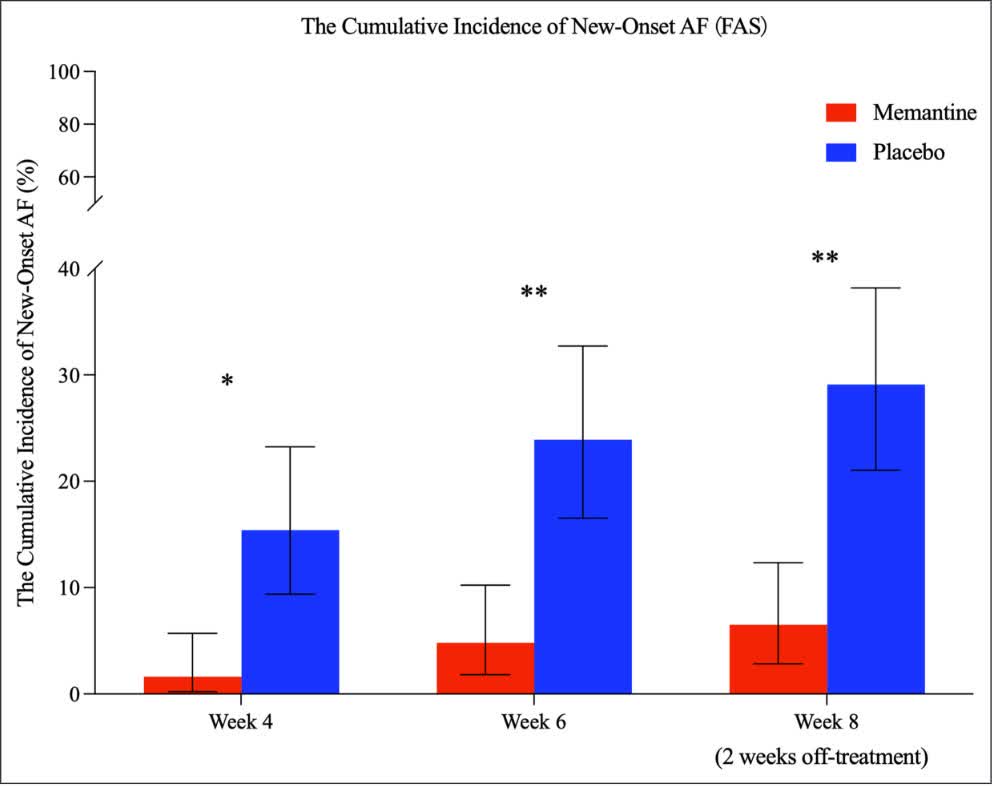
In a Phase 2 RCT, antagonism of NMDA receptors with memantine reduced premature atrial contractions, lowered non-sustained atrial tachycardia & cut new-onset AF risk, highlighting a novel glutamatergic pathway for atrial arrhythmia therapy. @zhoubingqing https://t.co/vYO4NVoWCQ
The CHAMPION trial does not forward the story of LAAO. No difference for major bleeding. No difference in all bleeding when procedural bleeding is included. Numerically worse for stroke. About 60% are CHADSVASC 2/3 WHO DON'T NEED OCCLUSION if ablation successful. #OCEAN