MajesTEC-9 trial: Teclistamab vs. VPd or Kd in RRMM, 1-3 prior lines. N=593, median F/U: 17.3 months. 18-month PFS 70% vs. 27%, HR: 0.29. 41% grade 3-4 infections, 6.5% deaths in Teclistamab arm #mmsm#ASCO26@NEJM https://t.co/I4kSOdeoL3
ERASMM Study: Elra In High Risk Smoldering MM
n= 76
Safety: Gr 3 CRS in 2 pts & No ICANS. 70% recd toci, , Infxn: 14% w/ Gr 3
Efficacy:
ORR: 90%, CR 30%;
Median F/U of 14 m: 72% CR rate; MRD rate 90% in evaluable pts
Responses deepened over time.
#mmsm#ASCO2026
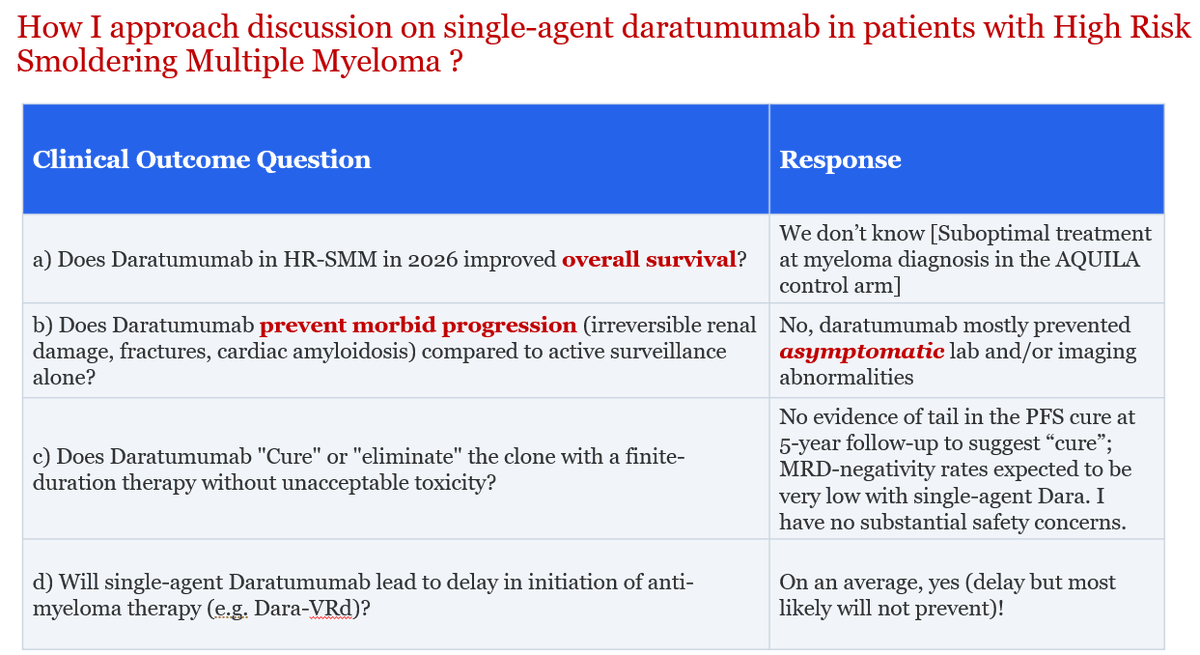
Since management of High Risk-Smoldering Multiple #Myeloma often comes up in clinic these days (and leads to spirited discussions with trainees and colleagues), sharing my approach here on how I counsel patients on the use of single-agent daratumumab.
I am genuinely excited though about fixed-duration BCMA BsAbs in selected patients, and looking forward to more data in coming years!
1/ 🧵 ANDROMEDA final analysis is practice-changing for newly diagnosed AL amyloidosis.
IMPORTANT tweets: 3/4 and 6 for clinicians who treats Amyloidosis
D-VCd = daratumumab + bortezomib/cyclophosphamide/dexamethasone.
With 61.4 months median follow-up, D-VCd improved depth of response, organ recovery, MOD-PFS, and OS. 🔥
#USMIRC #MedEd #medtwitter #mmsm #myeloma @USMIRCNEWS@US_HMC@MedwatchKate@Larvol@OncoAlert
Intriguing paper in
@ASHbloodjournal suggesting the delayed development of MRD negativity in transplant-eligible newly diagnosed myeloma patients with t(11:14) does not prevent the translocation's good prognosis.
https://t.co/ie6H5zOBYc
Glad this negative study was published by the @iStopMM group! No association of any dietary pattern with MGUS overall in this large population-based screening study. Before putting the burden of dietary intervention on our patients (beyond common sense), we must have randomized trials with clinically relevant endpoints.
Grateful to @ASHClinicalNews for highlighting our article on sFLC>100 criterion for #Myeloma diagnosis!
This creates two problems: Potential over-treatment of a majority of patients in a heterogeneous group & driving PFS benefit in high-risk smoldering myeloma trials by events that are not clinically meaningful!
As BsAbs move into earlier lines, infection risk is the elephant in the room!
Kim et al. @BloodAdvances: 75% cumulative infection rate at 24 mo.
Neutropenia and low IgG drove risk, early steroids did not.
IgG monitoring and timely IVIG remain key!
https://t.co/nT0q9VQZmv
Just in: Good news for the myeloma field.
FDA approves teclistamab plus daratumumab (Tec-Dara) combination for myeloma for patients who have had at least one prior line of therapy.
Note: Always use Tec-Dara with monthly IVIG. It’s not optional.
That was fast! And this is unprecedented curve is why.
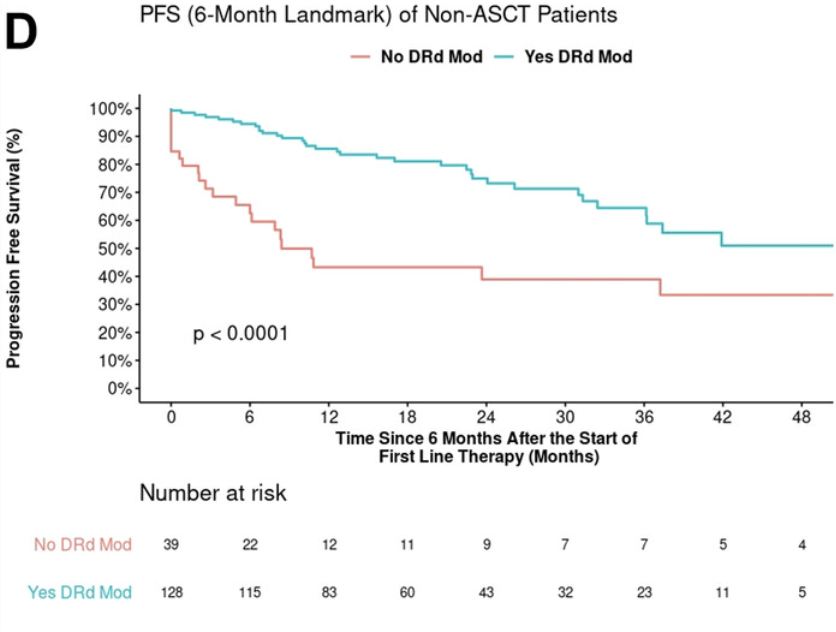
Picture worth a thousand words!
@AjHematology by Mayo myeloma: RW Dara-Rd in #MMsm
1️⃣ 2/3 pts required dose ⬇️, typically #downwithdex or #downwithlen
2️⃣ Landmarked PFS unequivocally better if so
My takeaway: Duration of Dara-Rd --> Dara(±R) more important than exact dose!
@mancunianmedic He was a patient of mine for a few years. He had a great self-deprecating sense of humour, particularly if he didn't think much of the play/programme he was involved with when I saw him.
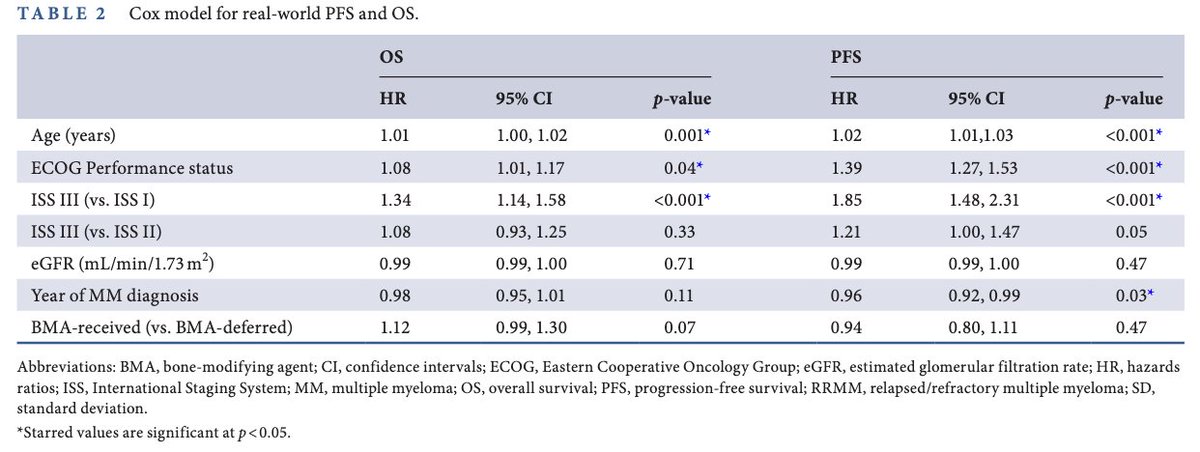
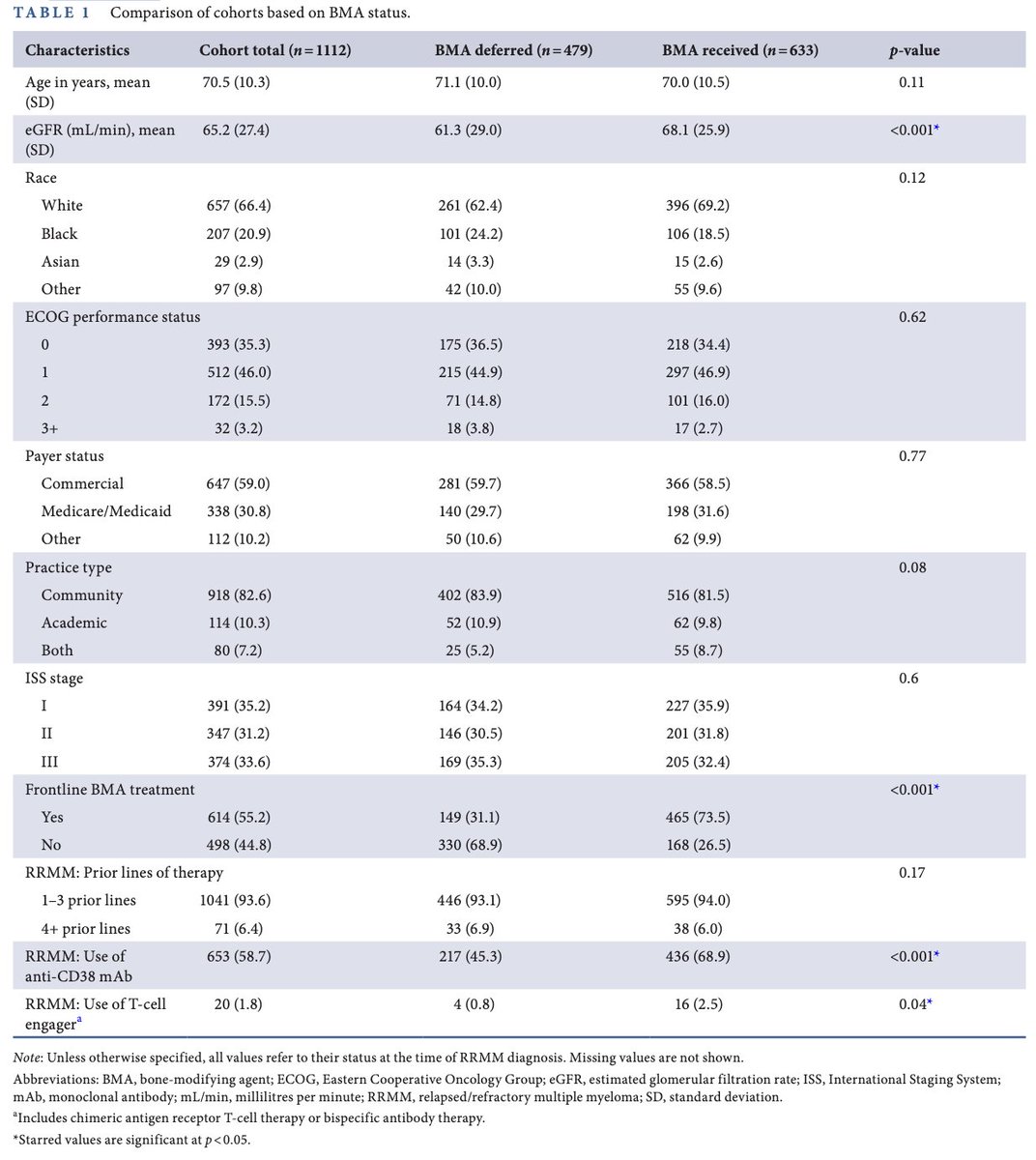
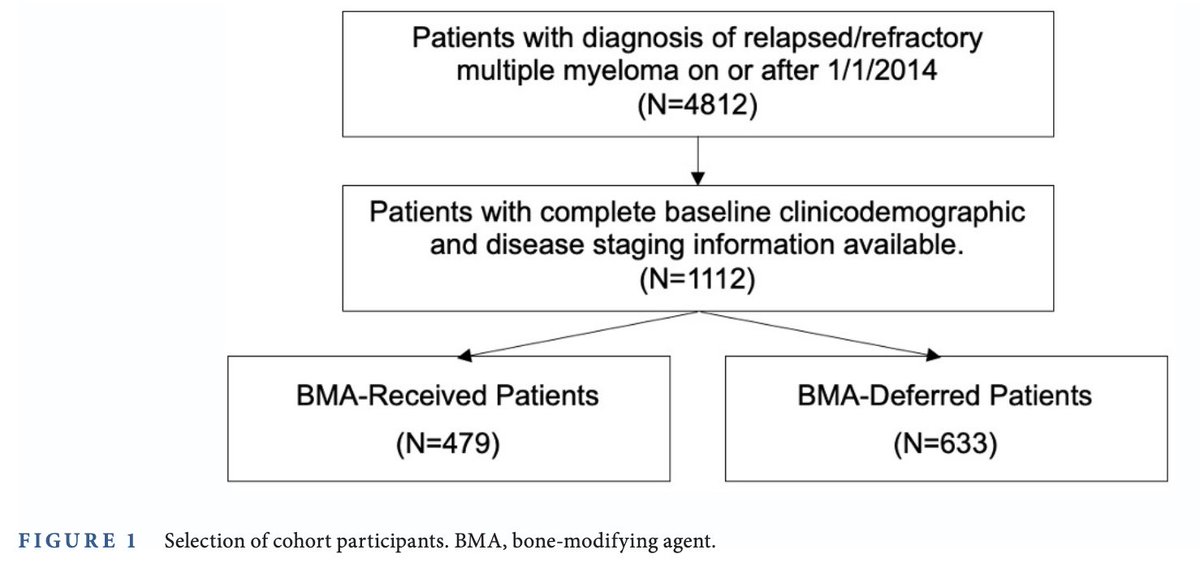
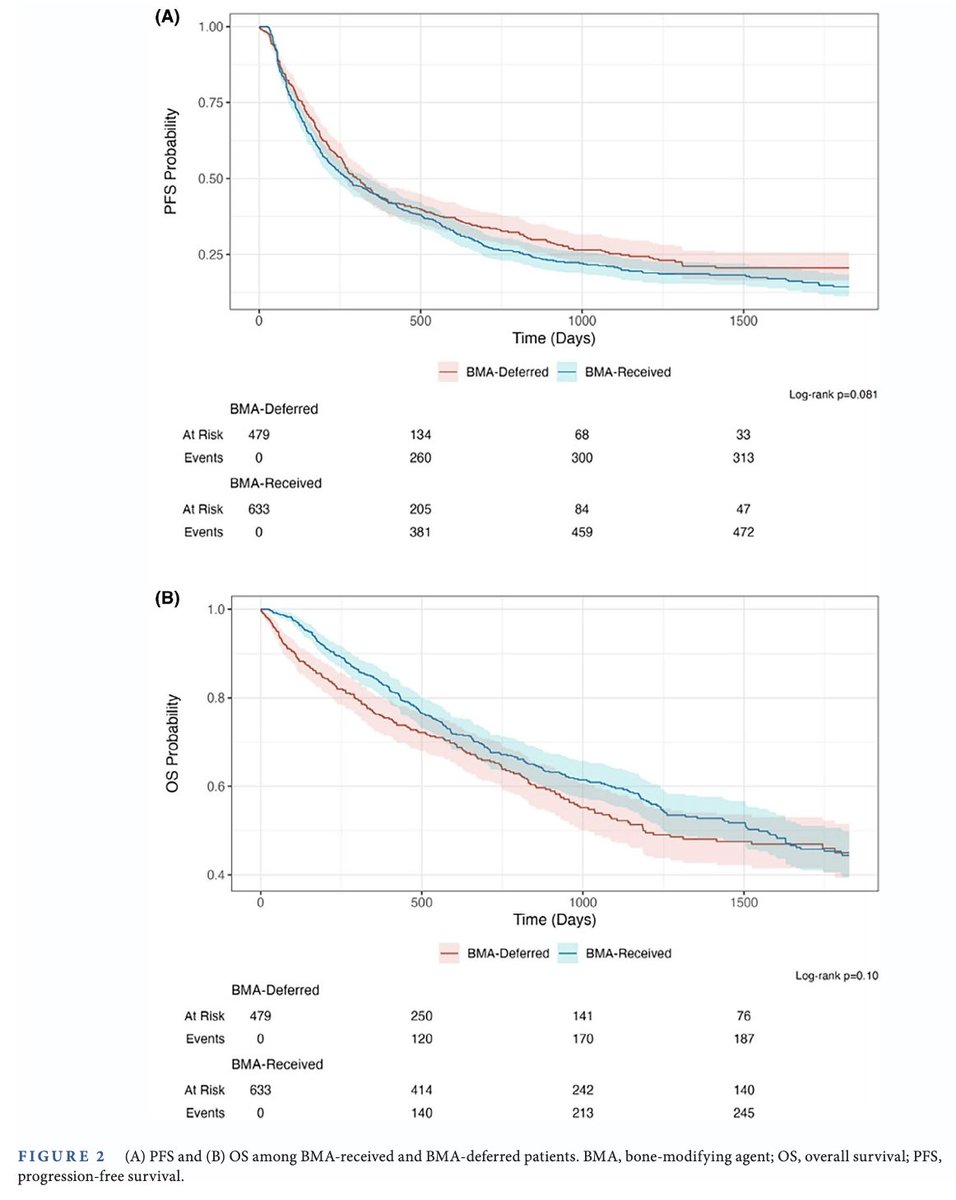
#Myeloma Paper of the Day: Real-world analysis of resuming bone-modifying agents in relapsed myeloma does not show improvement in long-term survival outcomes (median PFS 10.1 vs 9.2 months; OS 39.6 vs 51.5 months for deferred vs. BMA-received pts): https://t.co/uu8WW8HxFm. #mmsm
Excellent editorial by @DrRakeshPopat, re-evaluating the place of bispecific antibody therapy in the light of the groundbreaking MajesTEC-3 trial. #mmsm
Biting the Tail of CAR-T for Relapsed Multiple Myeloma | New England Journal of Medicine https://t.co/ILMMGme8o6