Proud to share that our team’s hard work, alongside our incredible collaborators, has led to the publication of groundbreaking data on colorectal cancer (CRC) from the GALAXY arm of the ongoing CIRCULATE-Japan trial, in both Nature Portfolio @NatureMedicine and @Annals_Oncology . The OS data presented could be practice-changing, particularly highlighting the crucial role of MRD (Minimal Residual Disease) testing in CRC treatment.
This is a significant advancement, especially for patients, offering new hope in improving outcomes and personalizing care.
Read our publications below:
https://t.co/gdW17Njc3s
https://t.co/7Ur27j1tCI
Read more in our press release below.
https://t.co/LkWVmCqhuB
@NateraOncology
New data published in @JAMAOnc adds to the growing body of evidence supporting the actionability of Signatera™ in colorectal cancer (CRC). This important study analyzed patients with resected CRC whose cancer had metastasized to the liver. For the first time in a large cohort, we saw that Signatera was predictive of an overall survival benefit from adjuvant chemotherapy (ACT) for patients with resected CRC liver metastases. The findings also showed that MRD-negative patients in this population derived no significant benefit from ACT. Our colleagues and collaborators discussed this data in an oral presentation this past weekend at the ESMO GI Congress.
Please read our press release for additional details and to learn more. https://t.co/qVQbQ9zmVb
🔥off the press🔥
Durvalumab with gemcitabine-based CTx in advanced BTC: primary results from the phase IIIb TOURMALINE study
https://t.co/GGqyAGNB2s
@JHepatology
👉Consistent efficacy & safety across 7 different chemo regimes
@myESMO@EASLnews@ILCAnews@curecc
🚀 Rapid oral innovation#ESMOGI26
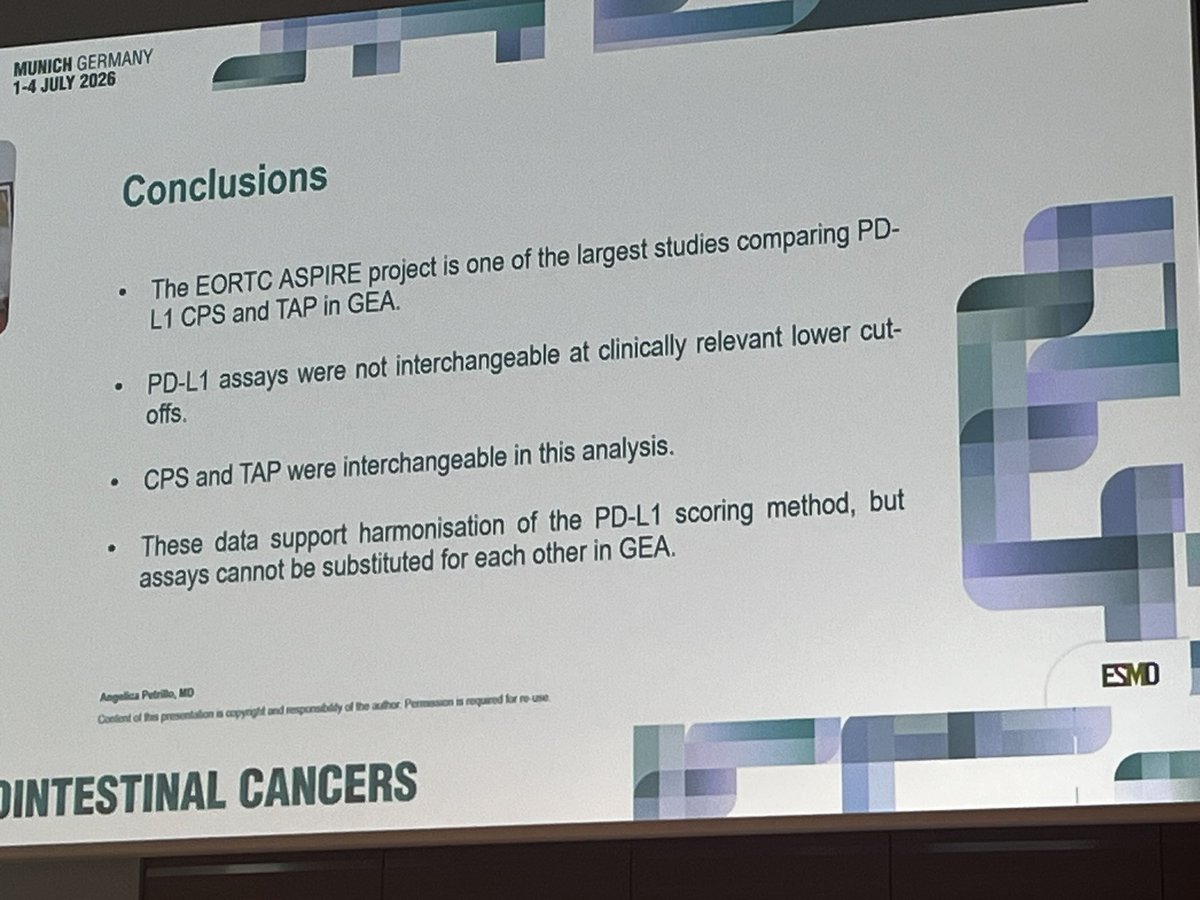
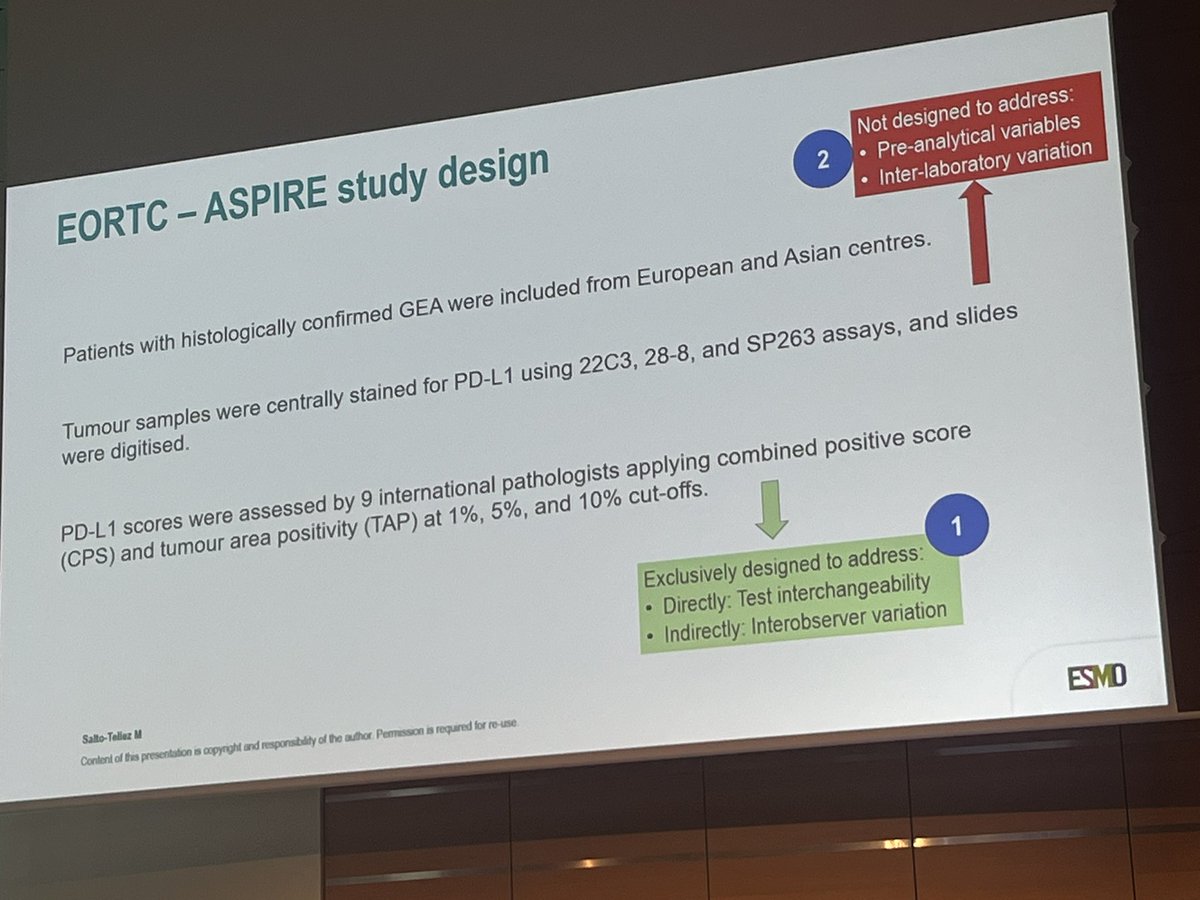
✅Interchangibiliry of PDL-1 assays gastric GEJ adenoca @EORTC
🚨Assays are NOT interchangable
✅CPS TAP interchangable
#cancer#Oncology#MedX@OncoAlert
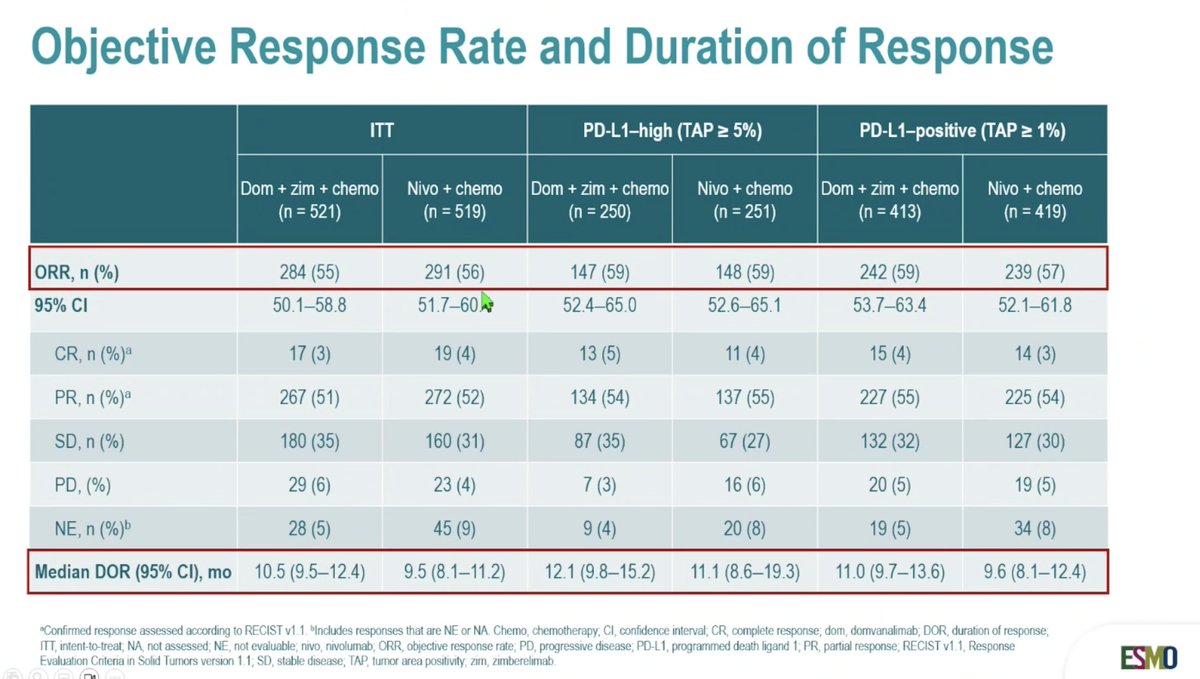
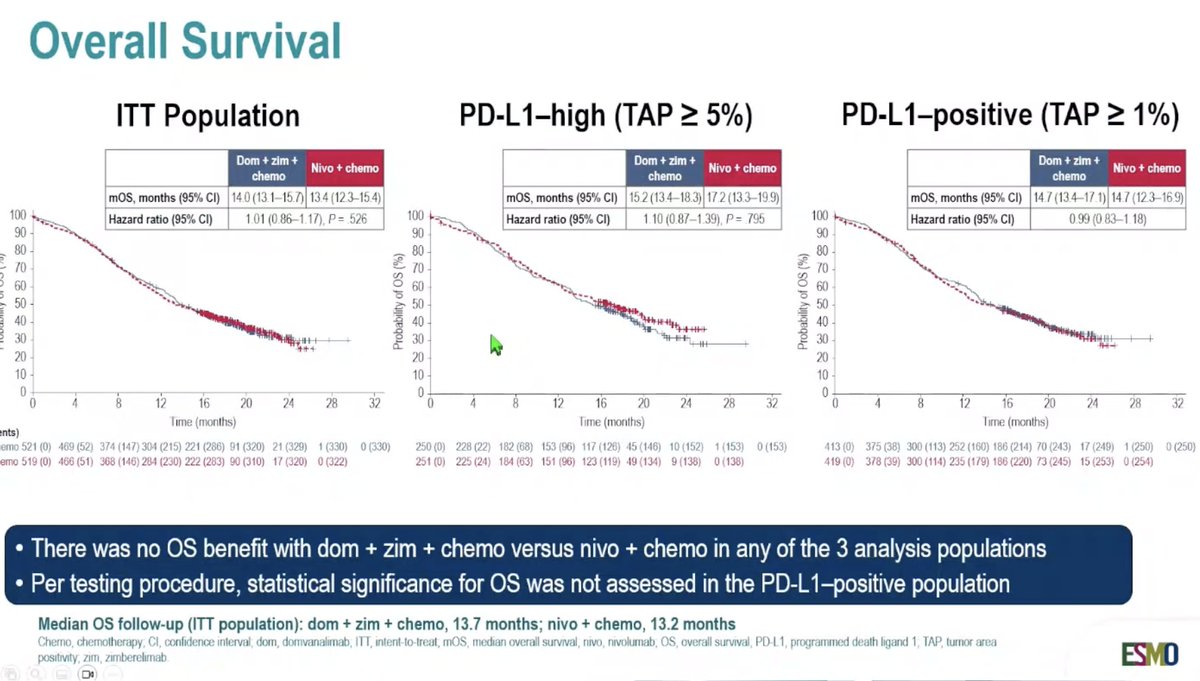
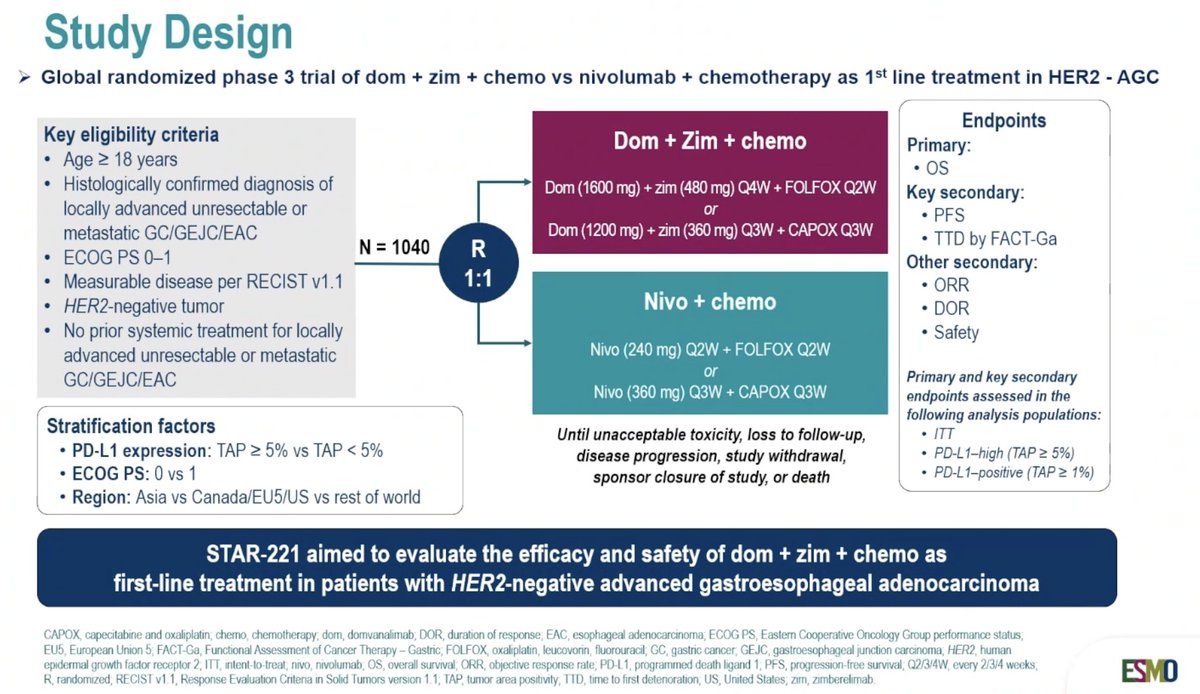
STAR-221: A phase III study of 1L domvanalimab, zimberelimab and Ctx vs nivolumab + CTx in advanced HER2-negative GC/GEJC/EAC
#ESMOGI26
👉no benefit for TIGIT&PD-L1 targeted therapy
🧐TIGIT remains a difficult target in oncology
@myESMO@ASCO
🚀Take home, summary #ESMOGI26@myESMO
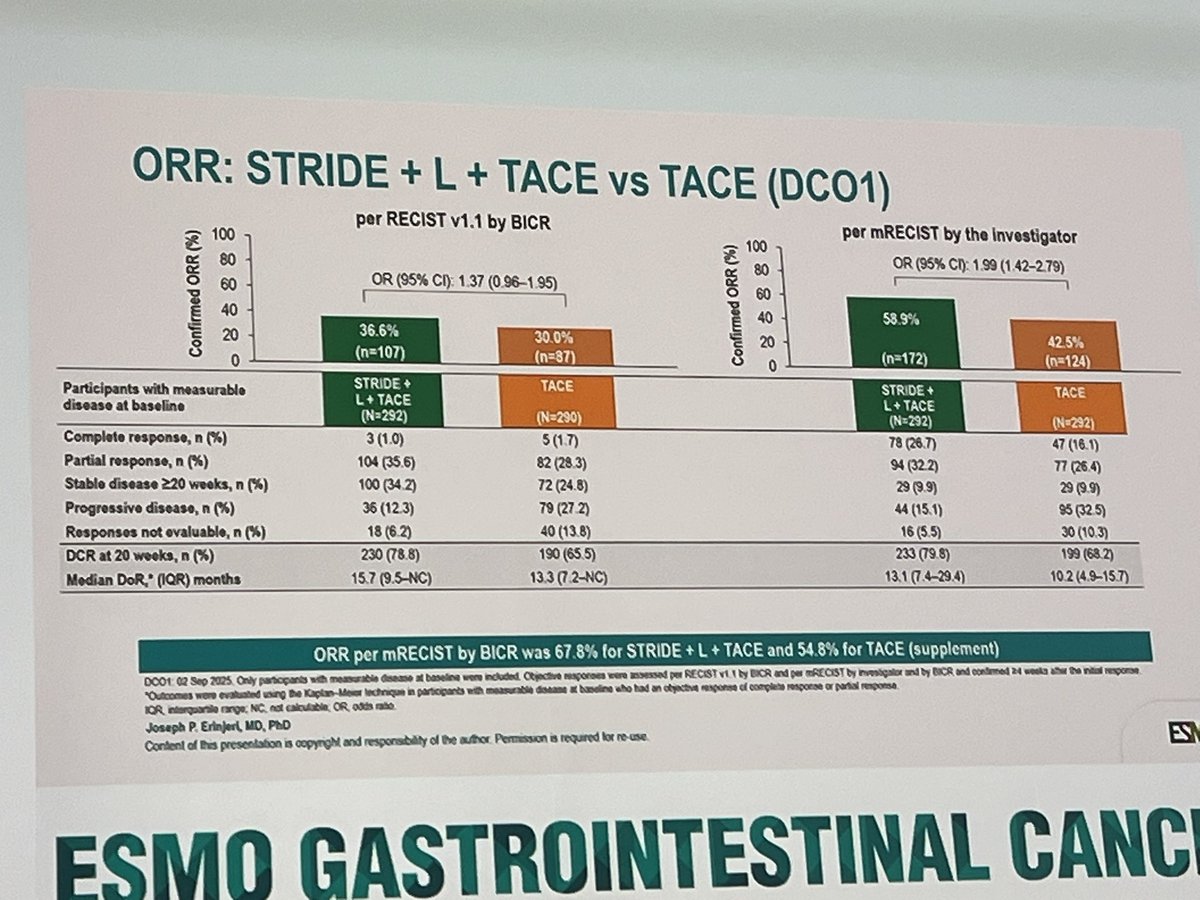
✅HCC: Cuse approach, TACE plus IO in intermediate HCC, TARE, downstaging with IO
✅NEN: molecular classification, young-onset NENs, small pancreatic NETs, radionuclide treatments
✅Gastroesophageal: HER2 treatments and zanidatamab, improving presicion, new IOs, doouble IOs and other drugs, FGFR2b, changing periop tx, oligometastatic disease
✅PDAC: KRAS inhibitors and zoldonrasib, daraxonrasib, local therapies (TTfileds, P-32 microparticles), Claudine18.2, new ADCs (ceacam5)
✅CRC: ctDNA/MRD in early-stage, improved survival in mCRC, IO for MSI-H, breakwater for braf, third and further line, anti-HER2, KRASG12C, bispecifics, ADCs, MET, IO in pMMR
#cancer #oncology #MedX @OncoAlert
Our latest research on ctDNA Status and ACT in Resected Colorectal Liver Metastases is now out in JAMA Oncology!
🔗https://t.co/RuRq2gkmSb
🔗doi:10.1001/jamaoncol.2026.2191
@JAMAOnc@OncoAlert
#ESMOGI26 Zani + ChT ± tisle improved outcomes & preserving QoL in 1L HER2+ mGEA.
📈 Significant PFS benefit (OS with zani + tisle)
💙 No clinically deterioration in QoL
⚠️ Diarrhoea was the main TRAE, no new safety signals
✅ Zani-based therapy, a new SoC 1L HER2+ mGEA.
@OncoAlert
#ESMOGI2026
Surprising news for mCRC out of ESMOGI.
KRYSTAL-10: Adagrasib + cetuximab misses its primary endpoint in 2L KRAS G12C mCRC.
After the accelerated approval and encouraging activity from KRYSTAL-1, many expected dual KRAS/EGFR inhibition to outperform chemotherapy in the second line. That didn't happen.
Quick hits:
• Primary endpoint (PFS): Negative
• mPFS 7.5 vs 8.1 months
• HR 0.89 (95% CI 0.71-1.13)
• Response rate dramatically improved
• ORR 47% vs 16%
• CR 7% vs <1%
• No improvement in OS at the final analysis despite the higher response rate.
So what happened?
This is a reminder that response rate ≠ durable disease control. Nearly half of patients responded, but those responses did not translate into longer PFS or OS compared with modern chemotherapy. Targeted therapy works, but mCRC can overcome via resistance mechanisms (such as via massive KRAS upregulation). Will be interesting to see how novel degraders come into the mix here... Remember, this is a first gen KRASi, the future is still bright here.
What does this mean for clinic tomorrow? Honestly, I still love a chemo-free option that is at least on par with chemotherapy.
This isn't the end of KRAS G12C in CRC. Far from it.
The focus now shifts to moving targeted therapy earlier, where combinations with chemotherapy may produce deeper, more durable responses before resistant clones emerge. Multiple frontline studies are already underway.
@TheGutOncLab@OncoAlert@Onco_Nexus@myESMO
#ESMOGI26
An interesting exploratory analysis from ATOMIC asks an important question:
How much chemotherapy do patients receiving adjuvant FOLFOX + atezolizumab actually need?
(Remember, this is our only adjuvant prospective study in MSI-H CRC and is with FOLFOX + Atezolizumab vs FOLFOX. If you can catch these patients before surgery, almost certainly better to treat neoadjuvantly).
Quick takeaways:
• Patients receiving >6 cycles of FOLFOX appeared to derive the greatest DFS benefit from the addition of atezolizumab (adjusted HR 0.45).
• That benefit was not apparent among patients receiving ≤6 cycles (HR 0.84), although this subgroup was relatively small.
• Receiving ≥12 cycles of atezolizumab was associated with numerically better DFS than shorter treatment, but this analysis is difficult to interpret given treatment discontinuation for toxicity and other confounders.
My interpretation:
This actually makes biological sense. Atezolizumab has consistently appeared less active than PD-1 inhibitors in MSI-H CRC. If that's true, then maintaining adequate chemotherapy intensity may be particularly important in this regimen.
I don't think these exploratory data answer whether 3 months of CAPOX is sufficient in dMMR disease. If anything, they reinforce that ATOMIC should probably be viewed as the regimen that was studied, than the exact regimen used in clinical practice.
Slides nabbed from @GillSharlene@TheGutOncLab@OncoAlert@Onco_Nexus@ESMO
🔥off the press🔥
Systemic therapy for HCC: Doublets, triplets and beyond
@JHepatology
👉comprehensive summary of systemic therapies in HCC
👇my author link
https://t.co/e9FfJdIIl2
@myESMO@EASLedu@ilca
🟠Adjuvant chemotherapy regimens in resected biliary tract cancers
TOG/GI-SAFRADJU-2501
@IntJCanc
➡️Our national registry study
➡️44 centers, 617 patients
❗️GemCis, GemCape or Gem are not superior to Cape
✅A positive signal for additional RT
🚨ECOG, T, N, R1 are prognostic
👉https://t.co/4IMhBB57kr
#cancer #oncology #MedX #biliary #cholangiocarcinoma #chemotherapy #adjuvant #gastrointestinal @OncoAlert@LorenzaRimassa
New episode of the @TheGutOncLab is out!
Had the pleasure of having a world leader in colorectal cancer on; Arvind Dasari! We talk about what is here now, and what will be in the future for colorectal cancer, including new technology and targeted therapy.
Available on Apple/Spotify below.
Great conversation.
Watch now on OncoNexus: https://t.co/xKcH5ApLc7
Spotify: https://t.co/Sft2mEriPf
Apple: https://t.co/Ij2FbbUQMX
@OncoAlert@Onco_Nexus