🚨New GLOBOCAN 2024 data show that the global cancer burden is not only increasing, but also widening inequalities. Incidence is higher in developed countries, whereas mortality is disproportionately greater in LMICs. By 2050, new cancer cases may reach 34.4 million!
New drugs alone will not be enough; prevention, early detection, and equitable access are essential🌍🌎🌏
https://t.co/aqbxpoQOet
Monday Morning Mention!
🩺 Study Protocol of OLIGOPELVIS 2–GETUG P12: A Randomized Phase 3 Study Comparing Intermittent Androgen-deprivation Therapy with or Without Salvage High-dose Intensity-modulated Radiotherapy to Oligorecurrent Pelvic and Para-aortic Lymph Nodes in Patients with Biochemically Relapsing Prostate Cancer by Quentin Josset...Stéphane Supiot et al
https://t.co/REp52mRUi2
💡 Patient summary
The OLIGOPELVIS 2–GETUG P12 clinical trial assesses short-term (6 mo) androgen-deprivation therapy in association with external beam radiation therapy in men with prostate cancer relapsing to pelvic and para-aortic lymph nodes of prostate cancer. The trial investigates whether radiotherapy targeting pelvic and para-aortic lymph nodes can improve the biological response while maintaining a favorable tolerability profile.
✨ We thank the authors for trusting EUO to publish your work.
@uroweb@mroupret@GPloussard@jteoh_hk@Ric_Campi@CaPsurvivorship@LauraMarandino@RenuEapen@Ecastromarcos@OncoAlert@Sciencedirect
🚨 New publication in Urolithiasis 🚨
Most surgeons look at a urine dipstick and ask:
"Is this patient infected?"
Our data suggest a different question:
"Can this dipstick tell me whether the pre-laser renal pelvic culture will be negative?"
During ureteroscopy:
✅ NPV 96.7% for pre-laser renal pelvic urine culture
✅ Immediate result
✅ Available 24–48 hours before culture results
Why is that important?
Pre-laser culture positivity was associated with:
🔺 6× higher odds of postoperative infection
🔺 9× higher odds of sepsis
A negative pre-laser dipstick may provide real-time reassurance while awaiting the culture result that matters most.
The dipstick is a rule-out test for culture positivity.
It is not a rule-in test for infection.
@Pietro9609@FZorzi@OTRAXER
#Urology #Endourology #URS #KidneyStones #Urolithiasis
Link to article below:
https://t.co/C0CLL8C1Px
65% of MIST studies on BPH are at high risk of industry sponsorship. Only 18% are low-risk across all Conflict of Interest criteria. A systematic review by Akgul, Herrmann, Netsch, Rassweiler, Guven, Romero Otero, et al. — unsponsored — asks how this should change guidelines.
https://t.co/MxrkoDI4vm
#BPH #MIST #EvidenceBasedMedicine
Prostate volume doesn't reliably predict obstruction — and we've known it for decades. A new open-access review in PCAN introduces a new concept: periurethral and transition-zone fibrosis is an under-recognised, untreated driver of LUTS/BPH.
The case for antifibrotics: pirfenidone, losartan, PDE5-i, even halofuginone. https://t.co/vIw1BF5CJs
People have been DM and asking me: with an HR of 0.68 for durvalumab + BCG in POTOMAC, why isn’t this for every high-risk NMIBC patient?
Here’s how hazard ratios work – and why they can mislead you if you stop there. 🧵 #ASCO26@tompowles1@WesKassouf@shilpaonc@DrFelixGuerrero
Managing LUTS after prostate radiation requires extreme caution before offering surgery.
Many post-radiation urinary symptoms improve over time or with conservative management alone. Once you operate on irradiated tissue, complication rates can be significant: incontinence, strictures, calcifications, necrosis, fistula, and need for repeat procedures.
Some series report post-TURP incontinence rates approaching 20–30%, and even higher complication rates with implants in previously radiated patients.
The key is honest counseling and balancing quality of life vs complications. Just because we can operate doesn’t always mean we should.
And perhaps the most important lesson: treat symptomatic BPH before radiation whenever possible.
#AUA26
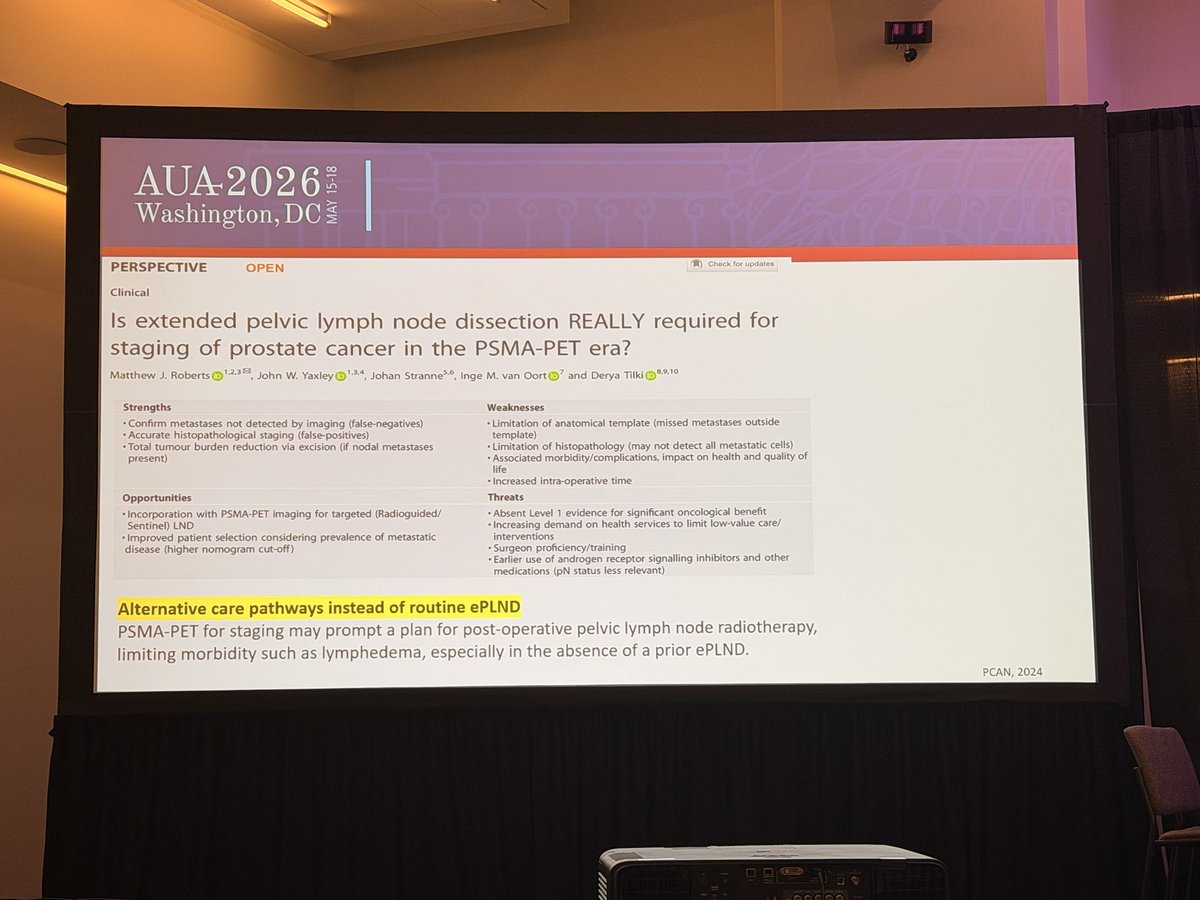
At #AUA2026, the message was clear: 📌 ePLND provides staging information, but its therapeutic benefit remains uncertain. 📌 RCTs have not shown consistent improvements in BCR outcomes. 📌 PSMA PET/CT has a high NPV (~96%) and may safely avoid unnecessary PLND in intermediate-risk patients with negative scans. 📌 Morbidity is not negligible: lymphedema, DVT/PE, and potential overtreatment. 📌 Up to 47% of nodal metastases may even lie outside the standard ePLND template.
The question is no longer “PLND yes or no?” 👉 It’s about smarter selection using PSMA PET, nomograms, and individualized risk assessment.
#ProstateCancer #PSMAPET
Ejaculatory sparing TURP
✅minimally invasive ( 4 hours =0.167 days discharge )
✅ No 3 months for improvement (immediate )
✅Cost effective (1/3 price of MIT)
✌️Easy principle ( preserve bladder neck & 1 cm pre Vero )
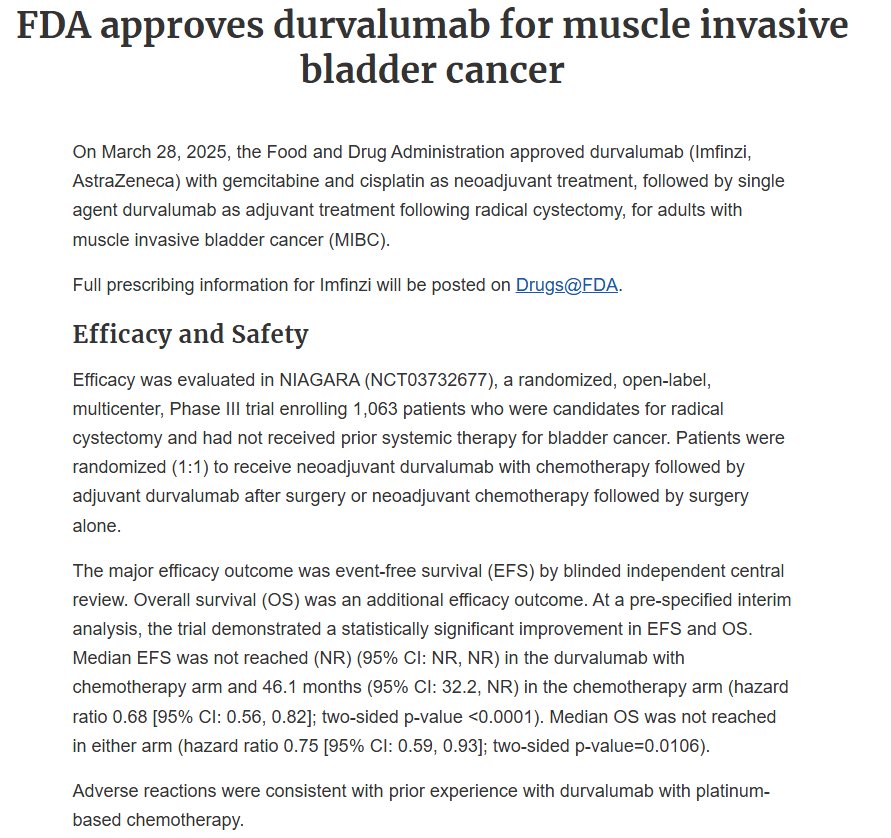
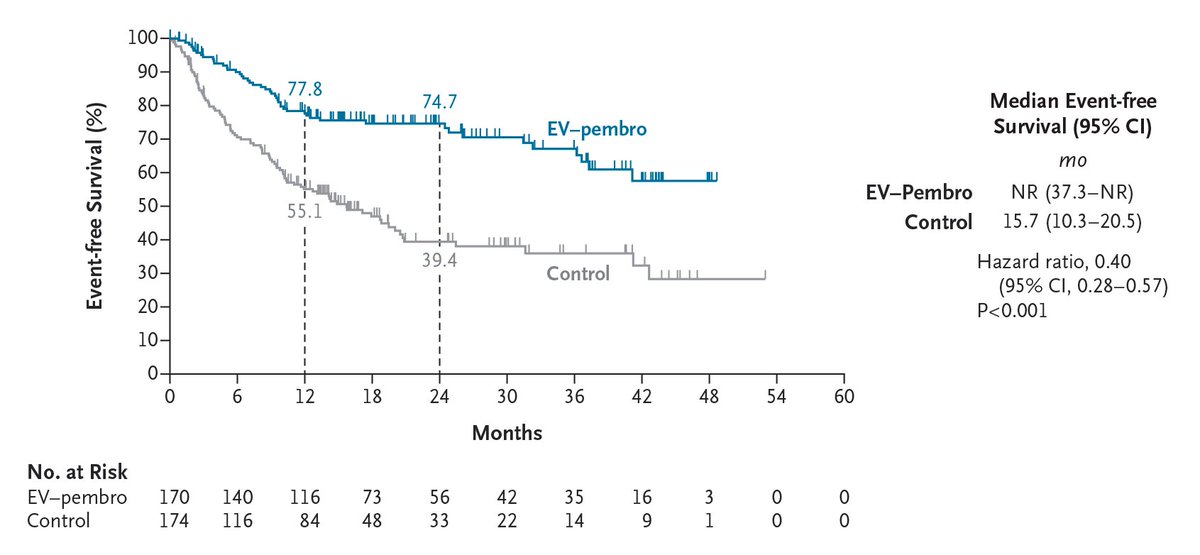
Original Article: Perioperative Enfortumab Vedotin and Pembrolizumab in Bladder Cancer (phase 3 KEYNOTE-905 trial) https://t.co/liPEVlPfHV
Editorial: Enfortumab Vedotin plus Pembrolizumab as Perioperative Therapy https://t.co/wIH8w21yJg
#Oncology
🩻Contrast-induced AKI:
one of the biggest myths still shaping clinical decisions
For decades we were taught:
👉 “Contrast damages the kidneys”
👉 “Avoid CT with contrast in CKD”
👉 “Hydrate, protect, delay imaging if needed”
But what if… most of this is wrong?🤔
->The uncomfortable reality
Modern evidence shows:
👉 Low-osmolar contrast rarely causes true nephrotoxicity
👉 Even in CKD, AKI, and ICU patients
👉 The risk is often overestimated—or nonexistent
So where did the fear come from?
📍 1950s high-osmolar contrast (actually toxic)
📍 Poorly controlled observational studies
📍 “Creatinine rise = contrast injury” assumption
👉 Correlation became causation
👉 And the dogma stayed
⚠️What recent data tells us
✔ No difference in AKI rates with vs without contrast
✔ No benefit from bicarbonate, NAC, or aggressive hydration
✔ Even ICU and AKI patients show no worsening outcomes
->Translation to real life
👉 The patient was going to develop AKI anyway...Not because of contrast!!
->The real problem: “Renalism”
👉 Avoiding necessary imaging
👉 Delaying diagnosis
👉 Choosing inferior tests
And that leads to:
❌ Missed PE
❌ Delayed sepsis source control
❌ Worse outcomes
->Clinical mindset shift
Instead of asking:
👉 “Will contrast harm the kidneys?”
We should ask:
👉 “Will NOT doing the scan harm the patient?”
->Who still deserves caution?
✔ eGFR <30
✔ Severe hemodynamic instability
✔ Multiple nephrotoxins
Even then:
👉 Optimize volume
👉 Minimize dose
👉 Don’t delay critical imaging
🤓Bottom line
✔ Contrast nephrotoxicity exists… but is rare
✔ The fear is bigger than the risk
✔ The harm of NOT imaging is often greater
In critical care
👉 We don’t treat creatinine
👉 We treat patients
And sometimes…
👉 The most dangerous thing is NOT the contrast
👉 It’s hesitation.
📃Reference
Florens N, Demiselle J.
Kidney360 7: 445–449, 2026. doi: https://t.co/CWzi7WC9Wx
Bir aşı, bir kanseri neredeyse sildi…
🇺🇸ABD’de 15-29 yaş kadınlarda serviks kanseri insidansı 2010-2022 arasında her yıl %24.2 düştü.
2006’da HPV aşısı yaygınlaştı. Sonra grafik düşmeye başladı. Şimdi neredeyse sıfırda.
Bu tesadüf değil. Bu bilim.
Serviks kanseri önlenebilir bir kanser. Tek şart: aşıya erişim ve aşıya güven.
🇹🇷Türkiye’de de bu tablo mümkün. Ama bunun için HPV aşılama oranlarını artırmak şart.
Çocuklarımız için. Geleceği olan her insan için.
📊 Kaynak: JNCI, Mart 2026
@DrYukselUrun@JNCI_Now@saglikbakanligi@sagliklicozum@ankarabbld@ttborgtr
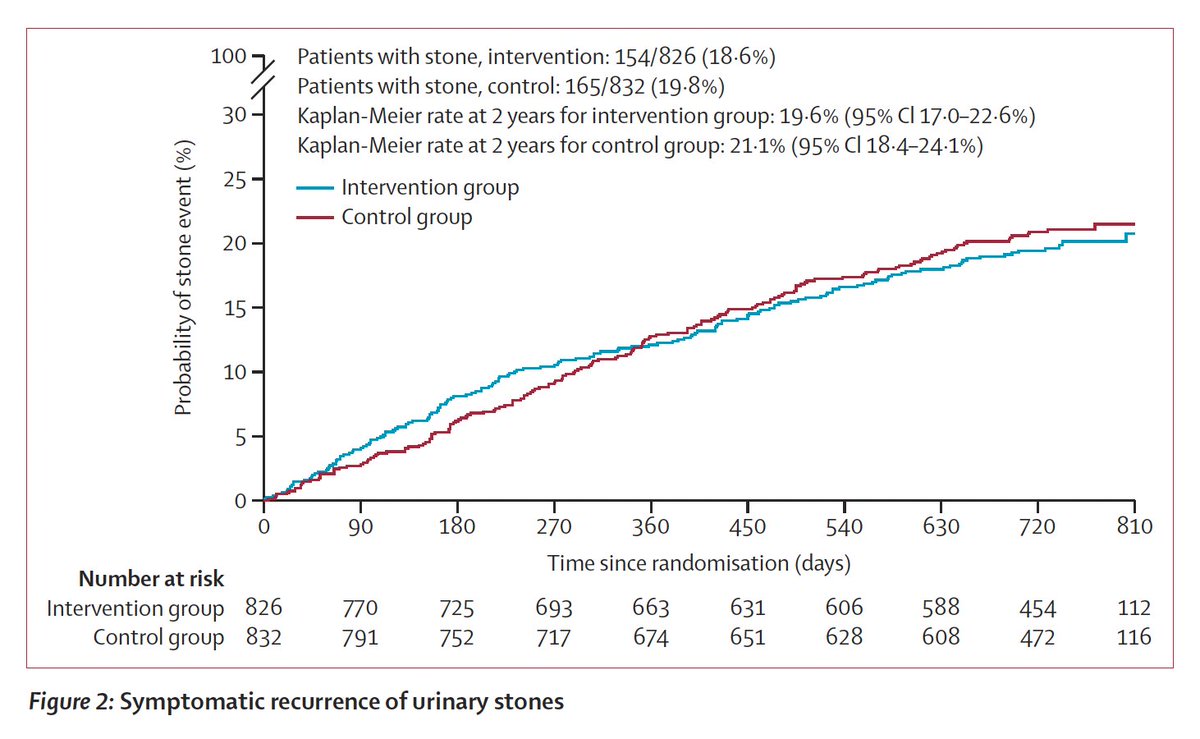
If you've had a kidney stone, you've been advised that the most important thing to prevent another bout is to increase hydration. Now a randomized trial of hydration in over 1600 participants showed no benefit, despite evidence of increase during volume. https://t.co/9ipUGlIsMz
#SESAUA26 State of the Art Lecture @sanojpunnen
PCa Screening Guidelines:
♦️Start: 45-50 yrs
♦️Screen q2-4 yrs if PSA < 1
♦️Screen q1-2 yrs if PSA >1
♦️Intervene: PSA 3-4
♦️Stop: 70-75 yrs or life expectancy < 10 yrs
@urotoday
Learn something new every day! Never knew testosterone so frequently dropped post-RP. May explain why sometimes first PSA is undetectable but recurrence happens months later when T recovers. Or it is meaningless and just a factoid great to ask med students and residents.
Thread: We obsess over operative time in BPH surgery. But what patients actually care about: will I need another procedure? New data from 420,611 real-world cases definitively answer this. (1/7)