In late March, the UCLA Division of Cardiology made a strong impact at the American College of Cardiology Scientific Sessions 2026. Their groundbreaking research presentations highlighted UCLA’s leadership in cardiovascular medicine. Learn more: https://t.co/uyxZ0Ehafn
Congratulations to Dr. Edward Ha on receiving the UCLA Distinguished Teaching Award! A dedicated hospitalist and educator, Dr. Ha’s passion for teaching and commitment to future physicians exemplify excellence in medical education. Learn more here: https://t.co/YvokiqTKQ1
#FlashbackFriday to our fellows covering our @UCLA IM residents on CCU, so they could enjoy their retreat!
#Bruinhearts always showing up for each other and our house staff 💙💛💙
And many thanks to those similarly covering Memorial Day weekend 🫡🫀
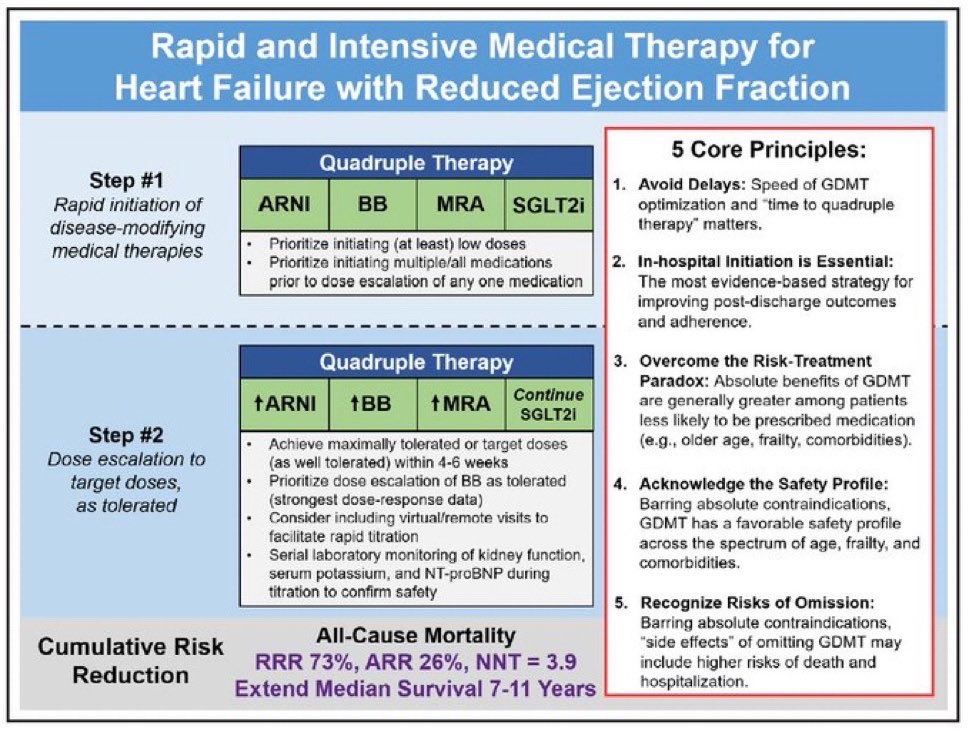
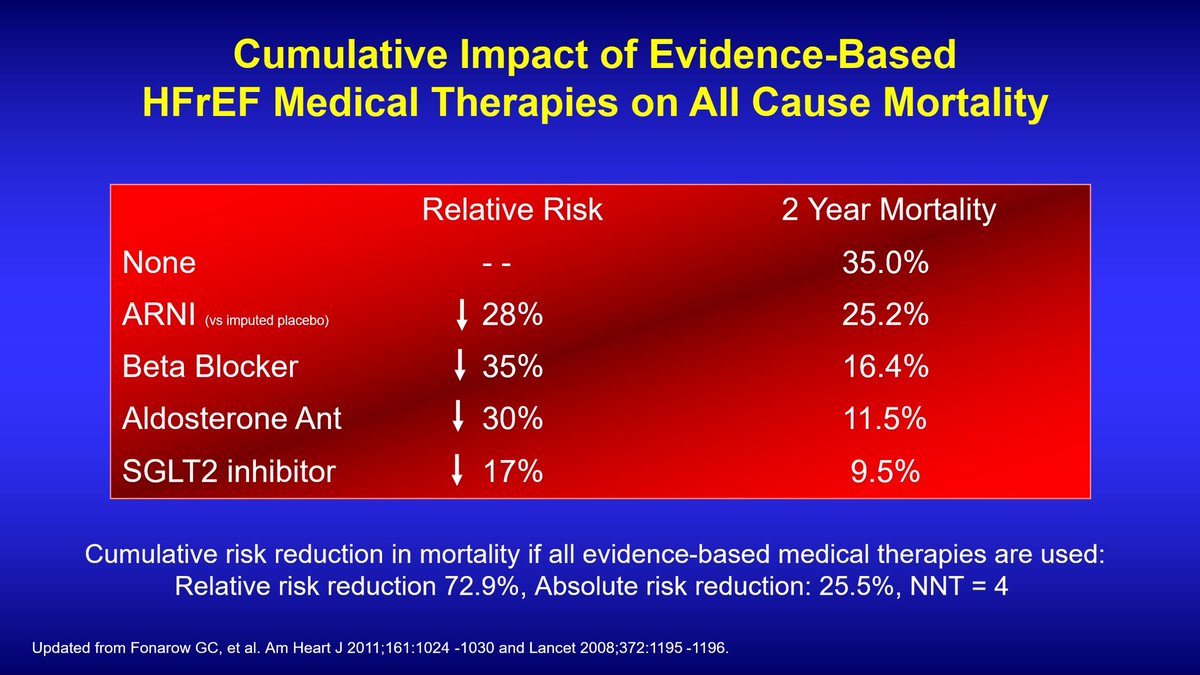
Quadruple GDMT for HFrEF
ARNI+BB+MRA+SGLT2i
At drug pricing in 2023 in US with annual costs of $9869, Q-GDMT was found to be cost effective (vs 2 or 3 drug regimens)
At 2026 pricing with annual costs of $420, now highly cost effective (ICER <$5000 per QALY saved)
Implement!
Why are 100% of eligible patients with HFrEF w/o CI or intolerance not receiving quadruple GDMT?
ARNI+BB+MRA+SGLT2i ➡️
75% ⬇️ all-cause ☠️ (26% ARR, NNT=4, 24 months)
85% ⬇️ HF 🏨 (33% ARR, NNT=3, 24 months)
Extend median survival by 7-11 years
💊 Cost $35/month
History made ✅ Congrats to the @uclawbb team on winning their first NCAA National Championship! 🏆 We’re honored to be your care team on and off the court. 💙💛 Shoutout to our orthopedic and sports medicine physicians for keeping these Bruins at their best.
A cholesterol AND #cardioonc curveball…& newly described IRAE?
#STAR future #bruinhearts chief @repettigiuliana Stumps the Profs w/ a ⁉️case of rapidly ⬆️ lipids after ICI myocarditis/hepatitis w/cholestatic injury ➡️ lipoprotein X!🤯 How 2 🔎?
🙏 to #ACCFIT chairs! #ACC26
Alt-X (@downloadaltx) builds AI agents that turn real estate deal documents into fully built underwriting models in Excel automatically, with every number cited back to the source.
Congrats on the launch, @SamadiRyan and Michael!
https://t.co/YSdwIyZevN
#2026 Withdrawing GDMT in patients with improved EF? Lifelong GDMT is standard, long after EF improvement. This trial however showed no outcomes difference with GDMT withdrawal in prior tachycardia mediated cardiomyopathy — once afib was controlled. WITHDRAW-AF Trial, EHJ 2026 ♥️
#2026 Withdrawing GDMT in patients with improved EF? Lifelong GDMT is standard, long after EF improvement. This trial however showed no outcomes difference with GDMT withdrawal in prior tachycardia mediated cardiomyopathy — once afib was controlled. WITHDRAW-AF Trial, EHJ 2026 ♥️
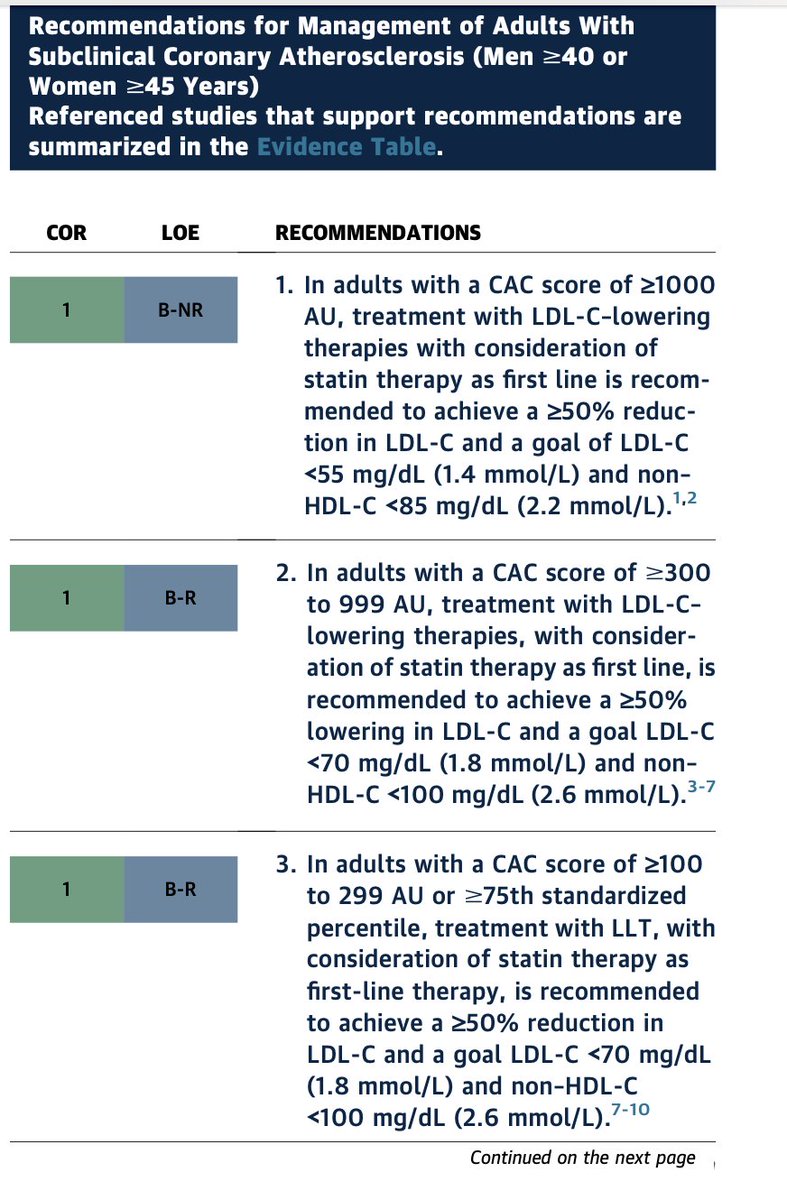
One of the most meaningful evolutions in the 2026 ACC/AHA dyslipidemia guideline is the continued elevation of CAC as a central tool in preventive decision-making.
We have come a long way.
1. In the 2013 guidelines, CAC was effectively sidelined.
2. By 2019, it re-emerged as a decision aid.
3. In 2026, it is now clearly embedded in the framework of risk assessment, treatment initiation, and treatment intensity.
Two messages stand out.
1. First, CAC has become the preferred decision aid when treatment decisions are uncertain. This is not an uncommon situation. In real-world practice, uncertainty is the rule rather than the exception, especially in borderline or intermediate-risk individuals. #PowerOfZero provides a clear distinction who is and not at risk that for the decision whether lipid-lowering therapy should be initiated.
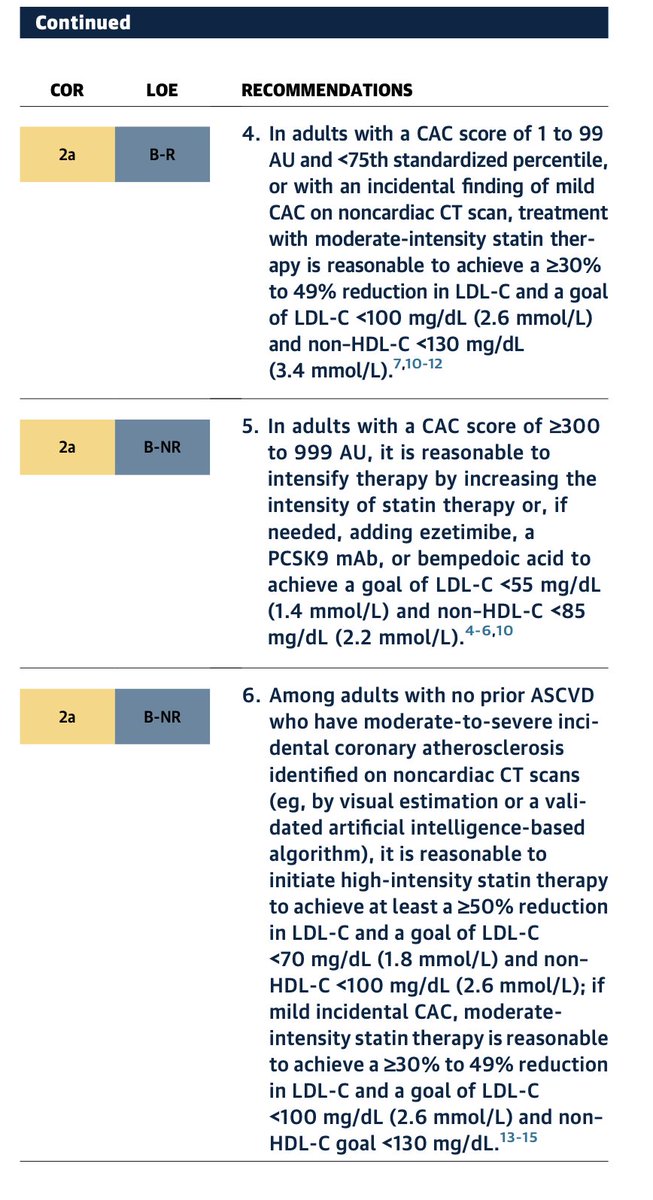
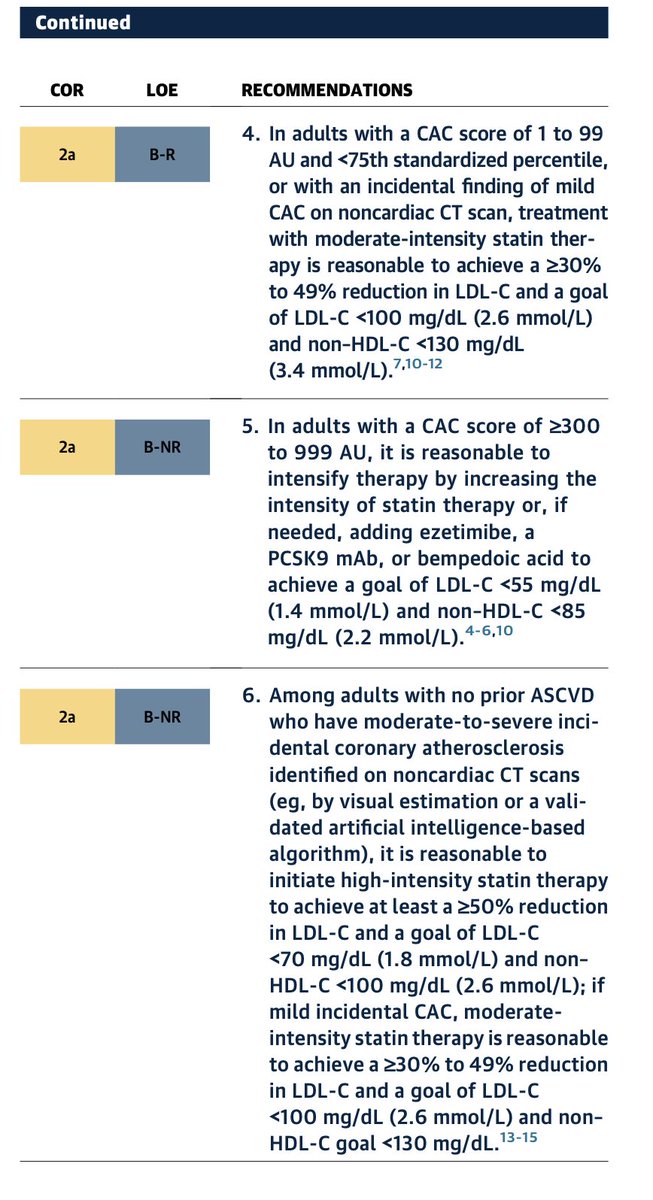
2. Second, the guideline goes beyond initiation. CAC is increasingly used to guide the intensity of therapy. Increasing plaque burden corresponds to progressively more aggressive LDL targets and therapeutic strategies. For example, individuals with CAC ≥300–1000 are recommended to pursue LDL reduction strategies approaching secondary prevention intensity, reflecting event rates comparable to treated ASCVD populations.
This is a MAJOR shift.
CAC is no longer simply a tie-breaker for statin decisions. It is evolving into a disease-guided framework for preventive intensity.
From a practical standpoint, this matters.Risk equations estimate probability. CAC visualizes disease.
1. When uncertainty exists, seeing the burden of atherosclerosis often changes the conversation for both clinician and patient.
2. It also aligns therapy more closely with biology (GREATER DISEASE, MORE INTENSE THE TREATMENT) rather than risk-factor projections alone.
IN 2026. CAC has moved from the margins of guidelines to the center of preventive cardiology.
For clinicians, that represents one of the most practical advances in translating risk assessment into actionable care.
Congrats @rblument1@RonBlankstein@DrMichaelShapir & rest of the guideline authors
@AJPCardio@ASPCardio@MichaelJBlaha@Sadeer_AlKindi@HMethodistCV
The 2026 ACC/AHA Dyslipidemia Guidelines now officially promote coronary artery calcium as a Level 1 class of recommendation - not once, but 6 times. The final step in the 36 year journey since Agatston published the first paper in 1990. @khurramn1@RonBlankstein@rblument1
CAC plays a larger role with class I when treatment decisions are uncertain. Risk estimation + risk enhancers are a starting point, and CAC can help resolve. And now there is additional support for using CAC to guide treatment aggressiveness. For example, CAC ≥100: LDL-C <70 mg/dl, CAC 300-999: LDL-C <70 mg/dl (consider <55 mg/dl), and CAC ≥1000: LDL-C <55 mg/dl. This strongly leans into event prevention when subclinical disease is manifest.
[6/14]
Beware,relying solely on color Doppler jet area for quantification can lead to major inaccuracies.A pt referred as severe MR. clinical finding,ECG,X-ray doesn’t suggest it. In MVP always put M mode through MR,if only late systolic single frame measurements(VC,MR area) are useless











































![AHAScience's tweet photo. Key updates to this guideline include:
➡️ The use of the American Heart Association PREVENT-ASCVD equations to guide primary-prevention and lipid-lowering therapy decisions.
➡️ Testing Lp(a) at least once in a lifetime and selective apolipoprotein B measurement to improve risk assessment and guide treatment
➡️ The return of LDL-C and non-high-density lipoprotein cholesterol treatment goals (with lower targets for higher-risk groups)
➡️ Expanded use of coronary artery calcium scoring to reclassify risk[ME1.1]
✍🏼 @rblument1 @tygluckman @RonBlankstein @PamelaBMorris @pnatarajanmd @AnnMarieNavar @SethShayMartin @APRN_CNS @nyulangone @DrMichaelShapir @kgradneyrd @eugeniagianos @virani_md @KellieMcLain1 @ijeomaheartdoc @SamiaMoraMD @DrHeatherJohn @dmljmd](https://pbs.twimg.com/media/HDPXv0SXsAIEPMD.png)




















