This is great news.
As you age, sugar binding to your proteins creates stiff, sticky chemical scars that affect skin, arteries, eyes and more. It was considered irreversible and now may be reversible, restoring to a healthy state.
Researches did this by using AlphaFold to search 45,000 oxidases, then screened more than 500 million engineered variants through directed evolution.
The work is still ex vivo in a lab setting. Delivering a large bacterial enzyme safely into living tissues, with sufficient penetration and bioavailability, remains a major challenge.
Right now, the sugar in your blood is sticking to your proteins. Not the sugar from food, but the glucose every cell runs on. Your HbA1c test measures this: sugar attached to a blood protein. Blood renews every few months, so that clears out. But your collagen, eye lenses, and artery walls last for decades, and there the sugar builds up into deposits called AGEs that stiffen the tissue. For 40 years, this was considered permanent, and no diet could reverse it.
Today, a paper reversed that view. Revel Pharmaceuticals, spun out of @DASpiegel256's Yale lab, engineered an enzyme that finds one of these tags, CML, and rebuilds the original protein. In tissue from elderly donors, it cleared over 70% from aged arteries and brought 75-year-old skin below a 31-year-old's level. The brown staining in the image is that damage. The pale panel is the same-aged tissue after the enzyme.
There are several caveats. It's in a dish, not a living body. It clears CML, not glucosepane, the crosslink that stiffens tissue most and is still beyond reach. Whether it works in a living person, nobody knows yet.
But "irreversible" just cracked. Revel is an @aubreydegrey spinout, the repair thesis he's pushed for 25 years, finally on the board.
Artificial light at night is a risk factor for age-related eye disease.
Evening light exposure above 1,000 lux was associated with a 31% greater risk of macular degeneration, an 18% greater risk of cataract, and a 47% greater risk of glaucoma.
1000 lux is very bright (e.g., a heavily lit television studio), but it illustrates the risks of nighttime light that may still be present at lower levels of exposure to screens or bright bedrooms.
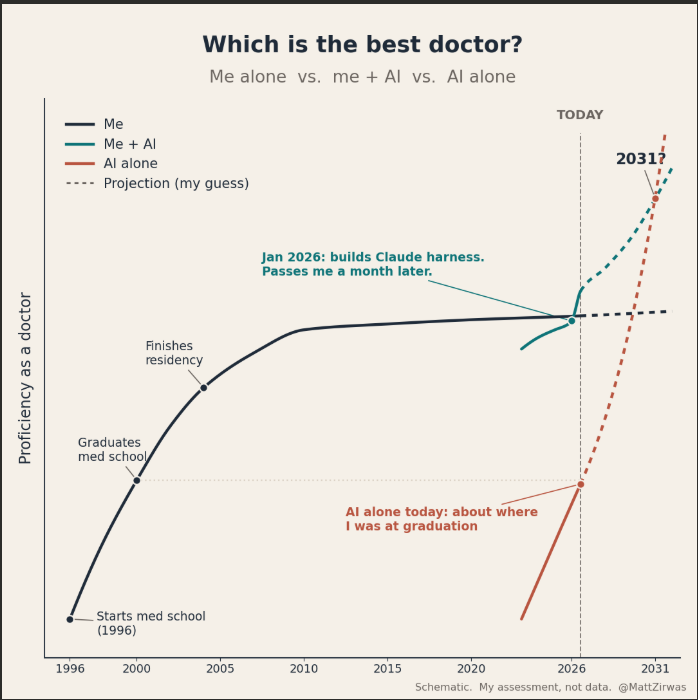
Whether AI is a better doctor than me is the wrong question.
The right question is this:
Which is best? Me alone, me + AI, or AI alone?
That sounds like a dumb question, but it's not and the answer isn't obvious or static.
A year and a half ago, the answer was me alone. AI made me worse. Slowed me down, gave me information that I had to verify and could have found faster on my own.
As of today, me + AI is WAY better than me alone. And that gap keeps getting bigger. Part of it is the AI getting better, part of it is me getting better at using the AI. The two compound.
My colleagues who don't get this are starting to get left behind. At an absolute minimum, start using OpenEvidence or ChatGPT for Clinicians. Both are free. Much better - build your own harness for Claude. It's better than either and not hard. One approach is in the first reply.
Some day AI alone will be better than me + AI. I'll just slow it down, send it in wrong directions, decide I know better than it when I don't.
But today isn't that day.
BOOM!
Humanoid Robots Just Performed Surgery for the First Time!
REAL VIDEO!
In a groundbreaking preclinical breakthrough, researchers at UC San Diego have achieved what many thought was years away: teleoperated humanoid robots successfully completing live surgeries.
Published in Nature, the study marks the world’s first use of humanoid robots for in-vivo laparoscopic procedures on large animals (pigs). Two separate surgeries were completed:
Key Details
•. Procedure: Laparoscopic gallbladder removal (cholecystectomy)
•. Team 1: Human surgeon + one humanoid robot (the robot performed core tasks while the human assisted)
•. Team 2: Two humanoid robots working together with no human at the operating table
•. Robots: Custom “Surgie” humanoids (~5 ft tall, ~60 lbs) using standard surgical tools
•. Control: Fully teleoperated by surgeons (remote human control, not autonomous)
•. Significance: First demonstration of humanoid robots handling real surgical workflows in a live setting, proving compatibility with existing OR tools and spaces
This proof shows humanoid robots could one day help address surgeon shortages, enable remote procedures in rural areas, battlefields, or even space all at a fraction of the cost and space of traditional surgical robots like da Vinci.
Read the full publication here: https://t.co/hSQ4sZb7Ma
Project page with video: https://t.co/xwIQk2tgb2
The future of surgery just got a whole lot more interesting. And medical cost for the first time in decades will be scheduled to go down, much further down.
Everyone assumed Ozempic helps fatty liver in the obvious way: lose the weight, and the liver fat follows. But a new mouse study from @DanielJDrucker’s lab, the man who helped discover these drugs, suggests weight loss is only half the story.
They mapped where the GLP-1 receptor sits in the liver. It’s on the thin cells lining the liver’s tiny blood vessels, plus some immune cells, not the main liver cells that store fat. Those vessel-lining cells are the ones that switch inflammation and scarring on and off.
Then came the clean experiment, run two ways in mice. Block weight loss but keep the receptor, and semaglutide still heals the liver. Keep the weight loss but delete the receptor from that vessel lining, and the liver stays sick even after the mice lose about 20% of their body weight.
So the weight loss was never doing all the work. The drug talks directly to the sick part of the liver. In mice, it’s a liver drug that also helps with weight loss.
Elon Musk’s latest predictions:
1: University degrees worthless within 36 months
2: AI takes over financial and legal work
3: Robots outperform the best surgeons by 2030
4: Saving for retirement “won’t matter”
Thoughts?
1/
10 years ago I published a paper predicting how machine learning would reshape plastic surgery.
Just reread it. Here’s what I got right, what I underestimated, and the one thing nobody in 2016 saw coming. 🧵
I’m a dermatologist. I’m supposed to say there is no amount of safe sun exposure.
But I won’t, because that’s a lie.
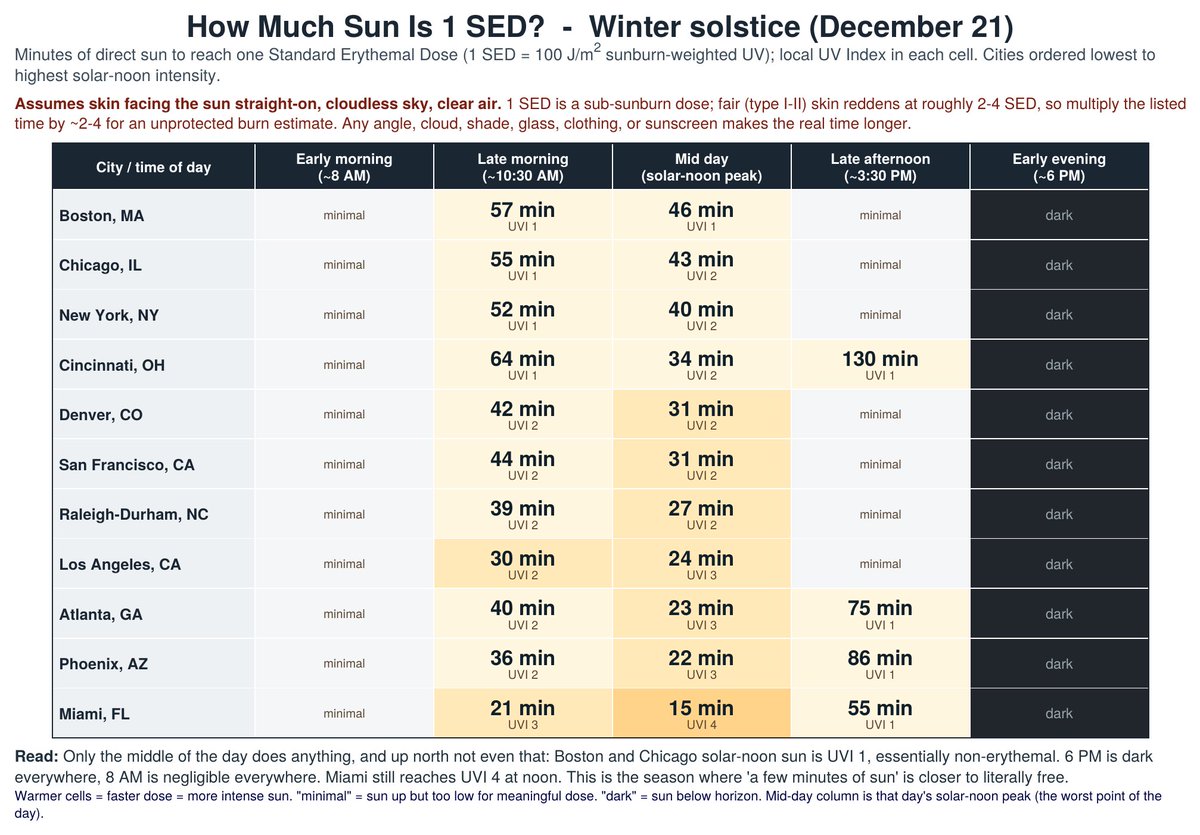
The attached shows how much sun is safe in different cities at different times of year.
What do I mean by ‘safe’?
I mean this: UV causes DNA damage and skin cancer.
But, shockingly, your body repairs that damage. As long as the damage doesn’t outpace repair and start accumulating it shouldn't increase your risk of skin cancer.
Data just came out that tells us how much UV you can get without damage accumulating.
They took the people most susceptible to DNA damage from UV and exposed them to UV, then did skin biopsies to measure the damage, then more skin biopsies to measure the repair, and repeated it daily for 4 days.
At 1.6 ‘Standard Erythemal Dose’ (SED) there was no accumulation of damage.
So, the attached charts show how much sun it takes to get 1 SED in different cities at different times of the year at different times of day.
And there are extra safety margins built in. It assumes a perfectly clear day with zero air pollution and that the sun is hitting your skin perpendicularly. Unless you’re laying flat, most sun is hitting you at an angle, which isn’t nearly as intense.
But a bigger question you might be asking is ‘Why would a dermatologist be telling you to get sun in the first place?’
Because getting sun reduces your risk of death.
Mostly by reducing your risk of heart attacks and strokes. That is very well proven.
But it’s also very likely that sun exposure reduces your risk of autoimmune disease, dementia, cancer and depression. It’s just not as well proven as the protection against heart attacks and strokes.
And before you reply and say ‘just take vitamin D!’, know that it has been ROBUSTLY proven that vitamin D has little (if any) benefit for preventing any of the above. Vitamin D is mostly useful as a marker of if you’re getting enough sun.
What do I do myself and what do I tell my patients?
Get as much unprotected sun exposure as you can without getting a burn.
That’s my GUESS as to what has the best risk/benefit ratio. Dying of skin cancer is actually really rare, especially when compared to the risk of heart attacks, strokes, autoimmune disease, dementia and other cancers.
But I’ll admit it’s not for sure best to get as much sun as possible, since sun does increase the risk of skin cancer and it might be the case the benefits plateau at a low level.
So, if you’re really worried about skin cancer stick to the charts.
The best science I can find says that amount won’t cause skin cancer.
The takeaway?
Sun is good for you, just don’t get a burn.