@LeivaOrly Agree completely. Sometimes get pushback along the lines of "well they're sick and might get a fistula at some point so you shouldn't do anything that could lead to subclavian vein stenosis." Even for a flimsy little triple lumen CVC. Different for a big HD line, obviously
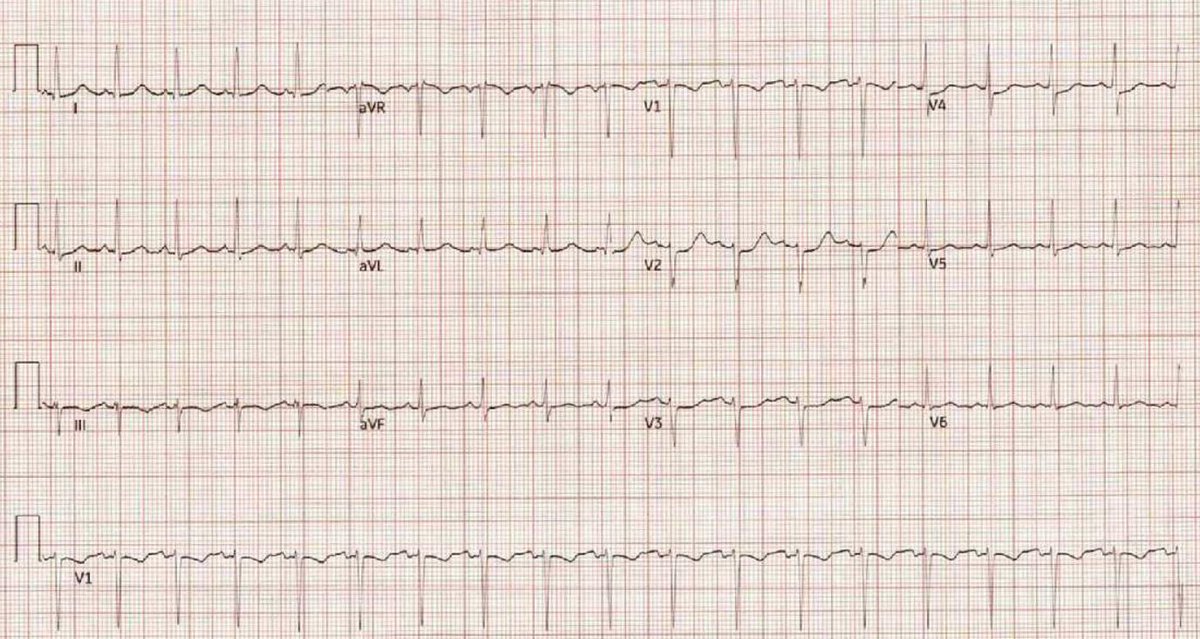
Late 30s female. Few months of chest pain acutely worsened prior to arrival. Pleuritic and worse with supine position but also exertional and alleviated with rest. 2nd ECG has posterior leads and was done 2hr later. Answer in thread #ECG#EKG#medtwitter#cardiotwitter#FOAMEd
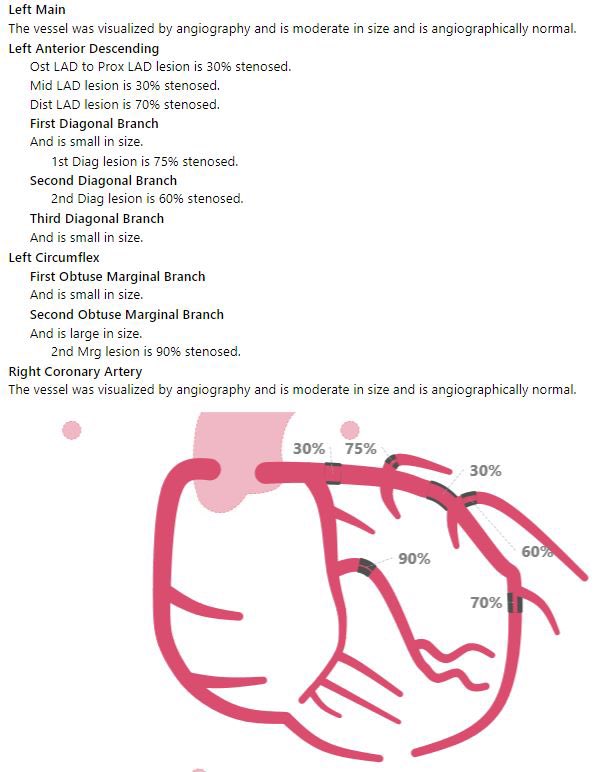
@safwanmsnr@RipDStar Typical anatomy is a posterior descending artery (PDA) that is usually supplied by RCA yes, but some patients (~5-10%) get it from the LCx. This is the idea of right vs left heart dominance. Smaller group are codominant (PDA comes from both sides)
https://t.co/nhkYvjRdfc
@PendellM Peaked at 2,965 about an hour before cath (normal for us is <40)
TTE “inferolateral wall is moderately hypokinetic. The inferior wall is moderately hypokinetic. All other wall segments are normal in function”
@MDtheDO I also think we under-utilize Mg. Works well especially when combined with amio. I also just found this trial in the works, will be interesting to see how it goes: https://t.co/erjLzE7k6L Mg+dig vs amio
@VivPaps @JSinghDO 2/2 They'll work two weeks of 5-6 shifts (the number goes down if the shifts are 12hr) and then will have multiple weeks off in a row every month to travel or spend time with family. It's very job dependent but things like that do exist out there and they allow full happy lives
@VivPaps @JSinghDO 1/2 Tbh I disagree with the original poster, in a lot of ways it is very much a lifestyle specialty. Yes you may have to pick up some extra holidays or weekends but I have friends who recently graduated who now have more time than ever