Presented at #SVIN25:
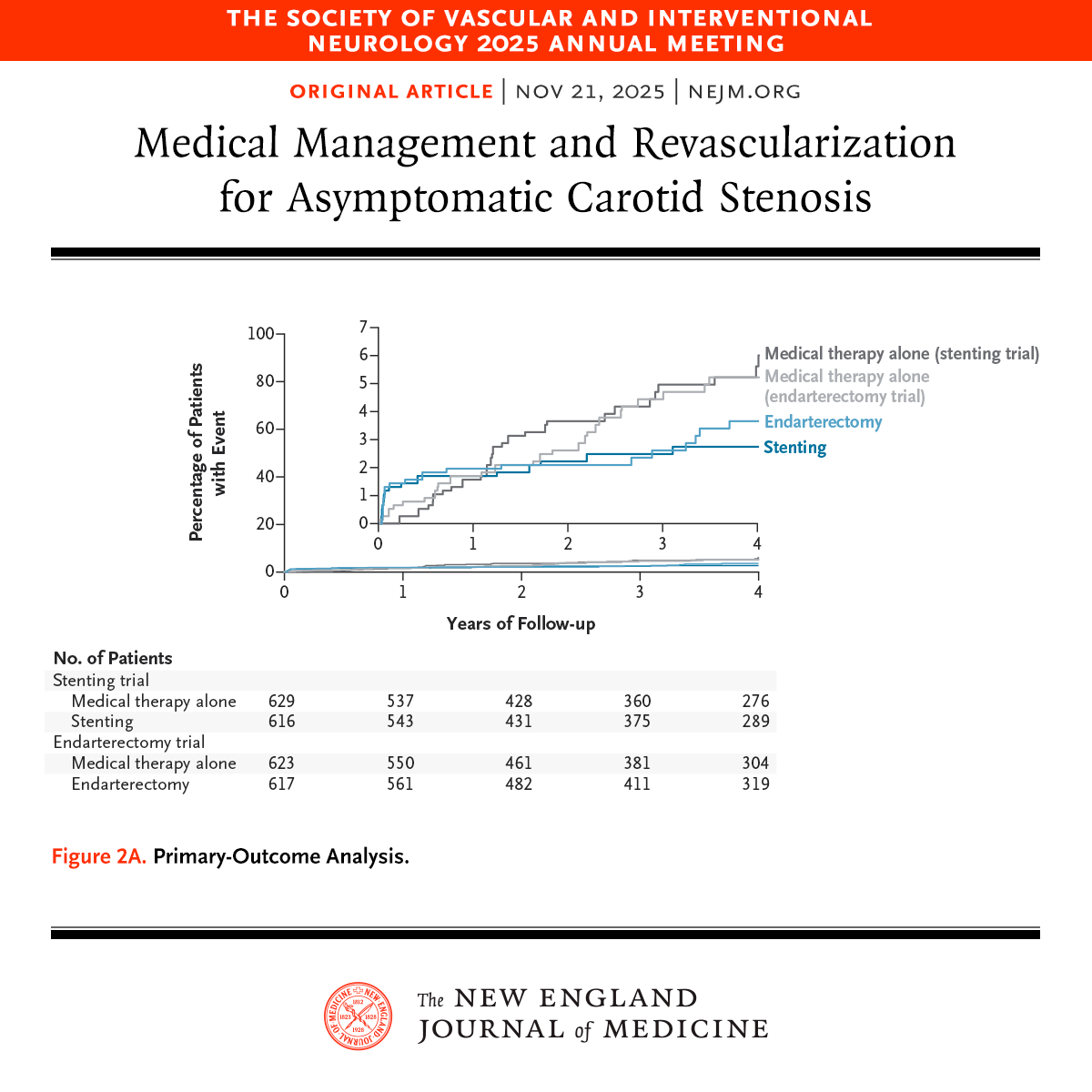
CREST-2: In high-grade asymptomatic carotid stenosis, addition of stenting to medical therapy led to a lower risk of stroke over a 4-year period. Endarterectomy did not lead to a significant benefit. Full results: https://t.co/ojge1CjqiU
Editorial: Managing Asymptomatic Carotid Stenosis https://t.co/D9LH89Edyk
@svinsociety
Considering Prestroke Disability in EVT Candidates: Lessons from the Italian Endovascular Stroke Registry
In this #BloggingStroke post, @JohannaSeidenMD discusses #Stroke article by Naldi et al. #AHAJournals
https://t.co/7RG0OTLxN4
Does trying to memorize inflammatory myelopathies leave you inflamed?
Do you say “Oh my!” when you see my-elopathy??
Never fear, read on for this month’s @the_AJNR SCANtastic for all you need to know:
https://t.co/1JAbPjZpyp
It is actually easy to remember the different patterns b/c their names tell you everything you need to know:
—MS
= Multiple spots so you see small spot lesions
MS has only 2 letters so lesions are less than 2 vertebral bodies in length!
—NMO
= Nuclear Massive Ouch. Nuclear = involve the gray matter or cord nucleus. Massive ouch
means lesions are extensive in both cross section & length!
NMO has 3 letters so lesions are > 3 vertebrral bodies in length
—MOGAD
Remember MO-PLAID. Has an H shaped appearance that looks like plaid!
Remember MO-Gad, or more gadolinium (it’s lesions can also be long & extensive)
—Sarcoid
Remember Sarcoid-y = Triploidy
Sarcoid has a classic 3-pronged appearance of the trident (central & subpial enhancement)!
—Lupus
Remember that lupus & Leptomeningeal both start w/L!
Lupus can give uniquely give leptomeningeal enhancement
—Paraneoplastic
Paraneoplastic = Parallel, so it parallels specific tracts
Commonly the motor tracts, including the lateral corticospinal tract, or dorsal columns
In this month’s AJNR, Fang et al. found AI accelerated double inversion recovery images could detect lesions in these patients as well as normal scans
Now you can add on a double inversion recovery to see these patterns better w/o adding on significant time!!
But this just scratches the surface. Follow @the_AJNR & check out the article yourself
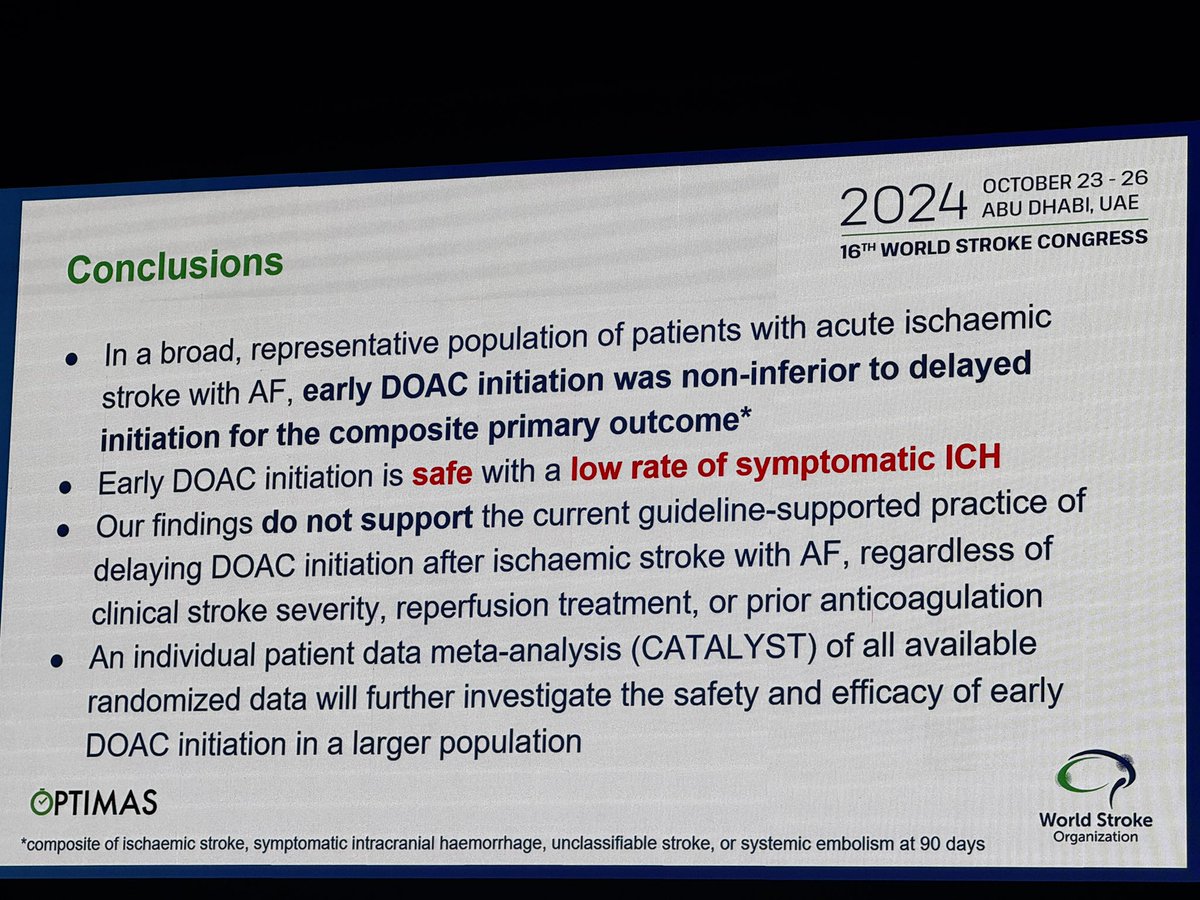
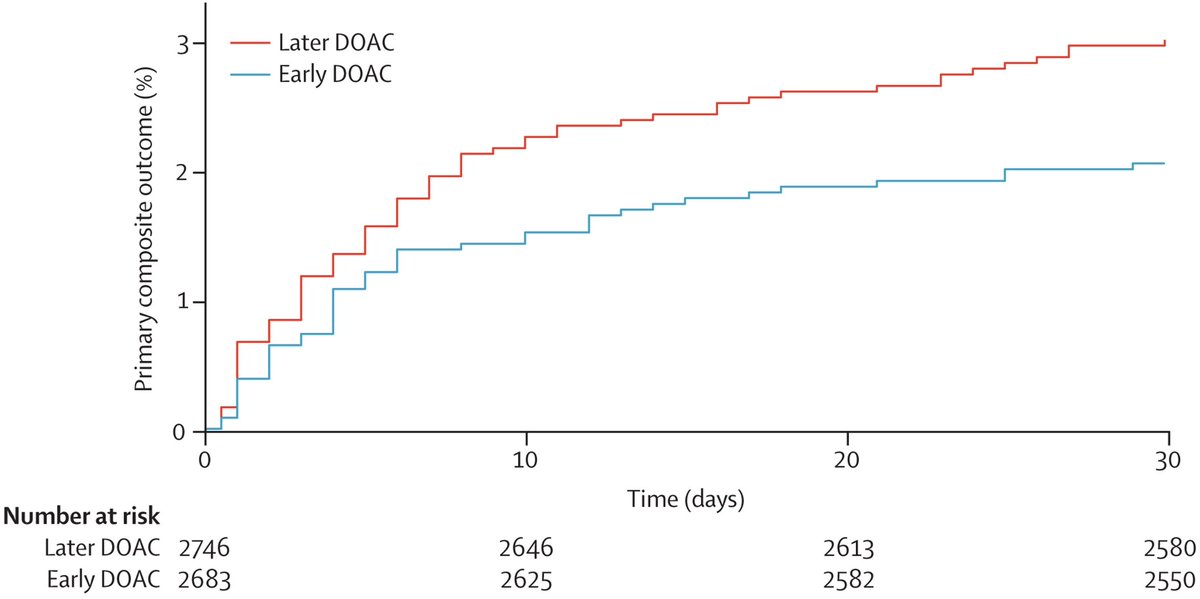
Collaboration on the optimal timing of anticoagulation after ischaemic stroke and atrial fibrillation: a systematic review and prospective individual participant data meta-analysis of randomised controlled trials (CATALYST) - The Lancet https://t.co/j9wHacf9Ql
Where is the evidence on treatments for Parkinson's disease motor fluctuations? How do we choose? Remember – ense et aratro – sometimes we choose the sword, but in Parkinson's, over time the plow is usually the better strategy. de Bie and colleagues do an evidence-based review in the journal Movement Disorders.
Key Points:
-What is a motor fluctuation?
- Here is a greatest hits list (7): 1- alternating periods of good movement control referred to as on, and poor movement control referred to as off. 2- wearing-off, 3- sudden shifts between on and off, 4- delayed onset of doses working, 5- dose failure, 6- freezing, and 7-dyskinesia.
- The International Parkinson and Movement Disorder Society (MDS) Evidence Based Medicine in Movement Disorders Committee updated recommendations based on all available research studies.
- 102 studies met criteria.
- Efficacious: levodopa extended release, pramipexole immediate release and extended release, ropinirole immediate release, rotigotine, opicapone, safinamide, and bilateral subthalamic nucleus deep brain stimulation (DBS).
- Likely efficacious: continuous intestinal levodopa infusion, continuous subcutaneous levodopa, continuous subcutaneous apomorphine, ropinirole prolonged release, ropinirole patch, entacapone, rasagiline, istradefylline, amantadine extended release, zonisamide, bilateral globus pallidus DBS, and pallidotomy.
My take: Parkinson's, in my opinion, is the most complex disease in clinical medicine. Though it is nice to see these evidence-based reviews, we should keep our eye on the 'ball.' The ball is dynamic, and in Parkinson's will fluctuate over time, and especially with disease progression. We need to listen carefully to the persons with disease. We need to pay attention to the timing of dosages and realize that more is not always better. We need to choose the 'cocktail of the day' for medications, and realize the mixture will change over time. We need to know when to pull the trigger for DBS, focused ultrasound or pumps, and also to not forget that exercise and multi-disciplinary therapies, as well as diet and sleep, can also help. Zonisamide is not used much in Western countries, and perhaps we should consider this choice more often? Remember, despite where the level of evidence is at the moment, we are pretty sure that GPi DBS is currently the best overall therapy for dyskinesia, and especially for brittle dyskinesia. Remember – ense et aratro – sometimes we choose the sword, but in Parkinson's over time the plow is the better strategy.
https://t.co/RKItYrzLPP #Parkinsons @ParkinsonDotOrg@FixelInstitute@MDJ_Journal
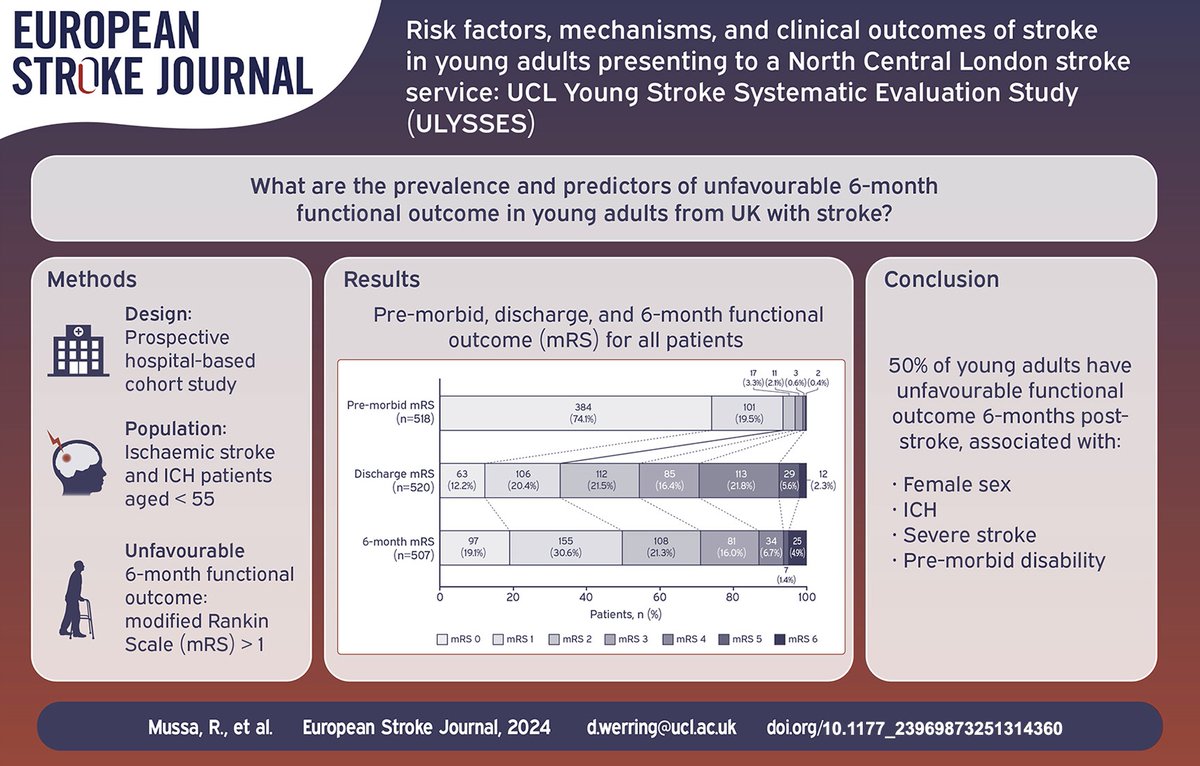
First paper from the UCL Young Stroke Systematic Evaluation Study (ULYSSES) @ESOstroke@raafiahmussa@HOzkan92 Open Access here: https://t.co/NT5erstHpB. We found unfavourable functional outcomes in half of the patients, associated with female sex and #stroke due to haemorrhage.
Rule of thumb for detecting M2 MCA vessel occlusion on CTA: ⤵️
✅ Superior M2 division = territory predominantly ant. to sylvian fissure.
✅ Inferior M2 division = territory predominantly post. to sylvian fissure.
Real time saver on those busy call nights 😉!
1/
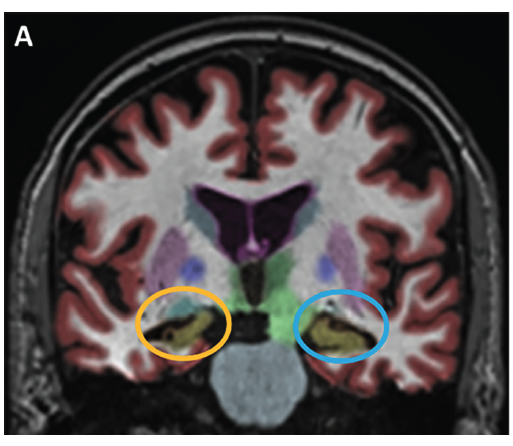
A 78 yo W is seen for 5 years of gradual short-term memory difficulties such as remembering to take her medicine, names, and poor recall of new facts. It seems her deficits are getting worse.
This is Alzheimer Disease, right?
Or… are you LATE in considering a different dx?
Feeling stuck in the middle when it comes to middle cerebral artery infarcts?
It may be only one vessel, but you can get many different infarct patterns & symptoms depending on where it is occluded!
Here’s what you NEED to know:
FIVE MAIN INFARCT PATTERNS:
1. Occlusion of the MCA stem or proximal M1 segment before the lenticulostriate origin
--Involves deep and superficial territories
--Weakness is usually severe. Face, arm, & leg are similarly affected
--Remember: Whole MCA occlusion = Whole hemiparesis
2. Lenticulostriate artery (LSA) Infarcts
--Involves deep territory
--Hemiparesis, hemisensory, aphasia & visual hallucinations
--Remember: LSA stands for Limp (weakness), Sensory deficits, & Aphasia
3. Distal M1 segment occlusion after the LSA origin
--Involves whole superficial MCA territory
--Sometimes weakness in face & arm > leg (brachiofacial hemiparesis)
--Remember: Distal MCA occlusion can somewhat spare the DISTAL most extremity (leg)
4. Superior Division occlusion
--Uncommon bc the superior trunk is so short
--Involves frontal & anterior parietal lobe, including pre- & post-central gyri
--Prominent faciobrachial hemiparesis w/matching hemisensory
--Rarely visual field defect
--Remember: Superior is more = more pronounced motor deficits than inferior division
5. Inferior Division occlusion
--Involves the temporal gyri & superior/inferior parietal lobule
--Facial brachial weakness is more mild than w/superior division
--Common visual field defect (homonymous hemianopia or upper quadrantopia)
--Remember: Inferior is less, so motor deficits are less pronounced
--Remember: Inferior starts w/the letter “I” = “eye” so visual field deficits
Hopefully now your reports won’t middling when it comes to middle cerebral artery infarcts!
The VYALEV™ (foscarbidopa and foslevodopa) subcutaneous pump has finally been approved by the @US_FDA. What do you need to know if you live in the United States and are considering this under the skin pump option?
Key Points:
- This is a pump that is similar to those used in diabetes and in cancer and the drug is infused under the skin (subcutaneous).
- This is a different option when compared to pumps that are inserted into the stomach or deep brain stimulation devices where electricity is delivered directly to the brain. This is also different from focused ultrasound (FUS) which makes a lesion in the brain.
- The data suggests that this therapy will be very useful for folks with 'off time' and who fluctuate between 'on' and 'off' medication and may or may not have dyskinesia.
My take: It is always a good day when we have more options for folks with Parkinson's disease. I suspect this will be a useful approach for select folks having trouble with off time or motor fluctuations/dyskinesia despite attempts by clinicians to change medication type, dose and frequency. The therapy is less powerful than DBS, and does come w/ possible side effects such as skin irritation, hallucinations and dyskinesia. Everyone should understand that there is no reason why you cannot eventually combine therapies and for example start with a pump and move later to a DBS. For those folks waiting a long time to try the therapy remember that reimbursements will vary from insurance company to insurance company and that Medicare will not likely kick in for reimbursement until well into 2025. Here is a key paper @TheLancetNeuro supporting the FDA approval (2022 publication of the phase 3 trial results):
https://t.co/F6NwCaOlIu
Press release from Abbvie on the FDA's approval yesterday.
https://t.co/Ts0M9imCwy #Parkinsons #dyskinesia #deepbrainstimulation @Abbvie@ParkinsonDotOrg
Pondering how to remember pontine syndromes?
Don’t become despondent about syndromes of the pons!
Here’s an easy way remember the basic parts of pontine syndromes:
Pontine lesions are usually vascular and are either from an infarct in the AICA territory (lateral) or paramedian branches of the basilar artery (medial)
Lateral & medial pontine syndromes can be remembered by the easy mnemonic THE PONS, w/ “THE” representing lateral syndromes & “PONS” representing medial syndromes
LATERAL SYNDROMES:
T = Temperature (spinothalamic = loss of pain & temp contralateral body, trigeminal nucleus = ipsilat face)
H = Horner’s (sympathetic pathway)
E = Equilibrium problems (spinocerebellar = ataxia of ipsilateral arm & leg)
MEDIAL SYNDROMES:
P = Proprioception (medial lemniscus = loss of contralateral vibration & proprioception)
O = Ophthalmoplegia (MLF = internuclear ophthalmoplegia)
N = Nonmobile (corticospinal tract = weakness of contralateral body)
S = Sixth nerve (Sixth nerve nucleus = loss of ipsilateral CN 6)
There are many different syndromes that vary by what exact structures are involved, but if you always remember THE PONS, you can easily pontificate about pontine syndromes!
Today marks an important milestone, and the first phase of the multi-phase journey is achieved. Our teams are committed to developing & implementing Welsh FLS model that truly benefit Welsh people. Next step is to meet all expected @RoyalOsteoSoc standards
https://t.co/F13J7Qyv1l
A summary of DECOMPRESS2 on decompressive surgery for patients with severe cerebral venous thrombosis (CVT):
1. 🧠 Decompressive Surgery Saves Lives: Decompressive surgery is a life-saving treatment for severe CVT, especially for patients with brain herniation risk, with two-thirds of patients surviving after one year.
2. 🛏️ Significant Disability Risk: Despite surgery, 39% of patients faced death or severe disability (Rankin scale 5-6) after 12 months, but 34% regained functional independence (Rankin scale 0-2).
3. ⏳ Early Surgery is Crucial: Most surgeries were performed within one day of diagnosis, underscoring the importance of quick intervention to prevent neurological worsening.
4. 🌍 Global Study: This study included 118 patients from 15 centers across 10 countries, making it one of the most comprehensive international studies on decompressive surgery for CVT.
5. 😊 Patient and Caregiver Satisfaction: Four out of five patients and caregivers expressed satisfaction with the surgery, even among those with incomplete recovery.
Source: Aaron S, Ferreira JM, Coutinho JM, et al. Outcomes of Decompressive Surgery for Patients With Severe Cerebral Venous Thrombosis: DECOMPRESS2 Observational Study. Stroke. 2024;55(5):1218-1226. doi:10.1161/STROKEAHA.123.045051.