I spent a bunch of time this week getting my Nvidia DGX Spark working in Ai2's post-training repo (open-instruct) for a local RL debugging machine. It was quite hard due to cuda 13 requirement and not many VLLM wheels.
https://t.co/9MFc4rmKMs
The linked paper is a nice document and summary product, but let's emphasize a few highlights:
1. Statement 16, strong consensus: ctHPVDNA should supplement conventional surveillance tools, rather than reducing or replacing them. Natural corollary: if it is not reducing or replacing surveillance, what is the point?
2. Statement 9, strong consensus: Detectable ctHPVDNA without clinical or radiographic evidence of disease often increases patient distress.
3. Statement 5, strong consensus: Large-scale, prospective randomized controlled trials are necessary to validate ctHPVDNA's role in HPV+ oropharyngeal cancer management. I would change that statement from validate to determine. Validate assumes it has a role today, but as the document states, it doesn't reduce or replace any currently established surveillance tools.
There are so many exciting ways that ctHPVDNA may influence care (screening/diagnosis, de-escalation, non-imaging-based surveillance) but these strategies need to be established in prospective randomized trials.
Mid-career achievement finally passed 5000 citations and 200 published manuscripts. Thankful for our excellent CNS team at OSU and all my worldwide collaborators!!@OhioStateRadOnc
Great to see our CNS/Peds director @joshuapalmermd! Making a huge difference for our patients in the state of Ohio and elsewhere through his prolific work @OhioStateRadOnc
BREAKING NEWS
The Royal Swedish Academy of Sciences has decided to award the 2024 #NobelPrize in Physics to John J. Hopfield and Geoffrey E. Hinton “for foundational discoveries and inventions that enable machine learning with artificial neural networks.”
Great time at brain mets PRO @ASTRO_org w/ @stuxrt and @wgbreen, reviewing prevention/diagnosis/management of radionecrosis and @OhioStateRadOnc experience w/ Boswellia! Thanks to @BeantGill118 and Avani Rao for organizing!
LLM bullshit knife, to cut through bs
RAG -> Provide relevant context
Agentic -> Function calls that work
CoT -> Prompt model to think/plan
FewShot -> Add examples
PromptEng -> Someone w/good written comm skills.
Prompt Optimizer -> For loop to find best examples.
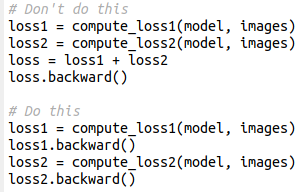
Bonus trick: you can remove the gradient reduction of the first backward (which is useless) by wrapping in no_sync()
Remember to also include the forward pass in the no_sync context, else it does not work
This simple pytorch trick will cut in half your GPU memory use / double your batch size (for real). Instead of adding losses and then computing backward, it's better to compute the backward on each loss (which frees the computational graph). Results will be exactly identical
why would I use a 200MB classifier when I can use a 40GB LLM named psiball-orpo-qdora-the-xplora-70B-int4-swiffer-sweeper-slerp-v0.02-(Taylor's version)
1/Have some confusion about tumor perfusion?
Do you go into a coma looking at scans for glioma?
Never fear!
Read on for this month's @theAJNR SCANtastic for what you need to know on the latest in brain tumor imaging!
https://t.co/FAZbEMZt7t
Tired of stressing whether a brain tumor is progressing?
Wish you had some insurance about calling tumor recurrence?
Here’s the cheat sheet you NEED for the best signs of tumor progression!
Read on for the newest @theAJNR SCANtastic on tumor imaging:
https://t.co/FagsDq18WT
▶️Tumor progression is like tumor escaping treatment.
🔷Just when treatment thinks it’s got tumor trapped at cliff, tumor is able to get away
🔶Think how you would get away if you were chased to a cliff’s edge---these are same signs of tumor progression:
➡️Jump off into the water:
🔸Tumor heads to the water—the ventricular surface
🔸Subependymal enhancement is very specific (93% sensitivity), but it isn’t commonly seen (38% sensitive).
➡️Cross over the rickety bridge:
🔸Tumor crosses over the brain’s main bridge: the corpus callosum
🔸Callosal involvement is only significant if combined w/multiple foci or crossing midline.
➡️Slide down the rocks:
🔸Spectroscopy looks like a slide down: Increased choline is seen w/recurrence—when combined w/low NAA, it looks like a reverse Hunter’s angle
🔸Increased Cho/NAA or Cho/Cre ratios can suggest recurrence
➡️Run fast & get your red blood hot:
🔸Blood volume is hot on perfusion: high rCBV on perfusion
🔸rCBV hotter than the normal contralateral white matter can be used as a gestalt
🔸Quantitatively, rCBV >1.75 is high suggestive of tumor & rCBV > 1.0 is concerning
➡️Try to sneak away when it’s dark:
🔸Tumor looks dark: Low ADC value (dark on T2) is concerning for tumor
🔸Quantitatively ADC value ≤ 1220 × 10-6 mm2/s is 74% sensitive & 89% specific
🔸I joke, “If the ADC is less than 1000 x 10-6, I am 1000% sure it’s tumor!”
Now you know the best signs of tumor recurrence on imaging!
Hopefully now you know when tumor progression should make your impression!