@declangmurphy@EveraertsW@piet_ost@shanekronos So … I indeed cannot seem to find a recommendation anymore in favor of PLND in the new guidelines 😮 I must admit I am a bit confused, what should we fight against now 🤷♀️😁
🔬ePLND in #BladderCancer 🏥
😞 More harm. ❌Zero benefit
📚Level I evidence from @SWOG👩⚕️👨⚕️
https://t.co/4sq6jsXkjF
(tnx @KBGinsburg for alway being the first to find the good stuff!) #ASCO23@ASCO
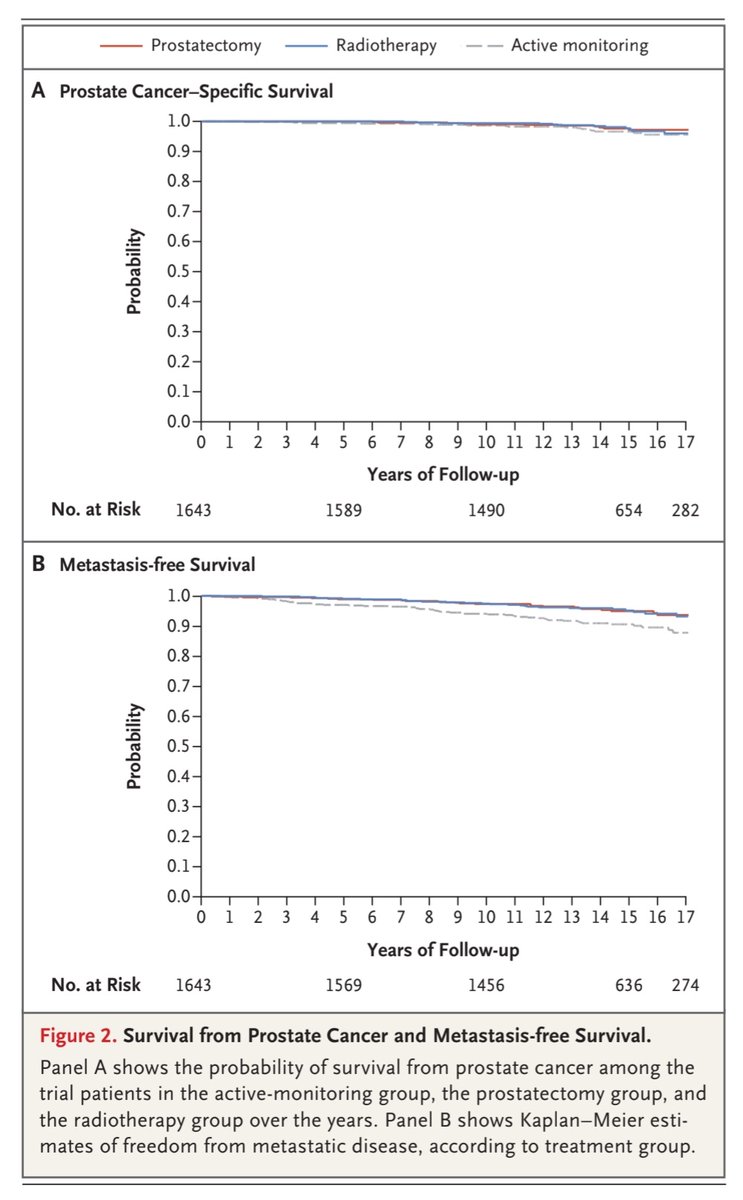
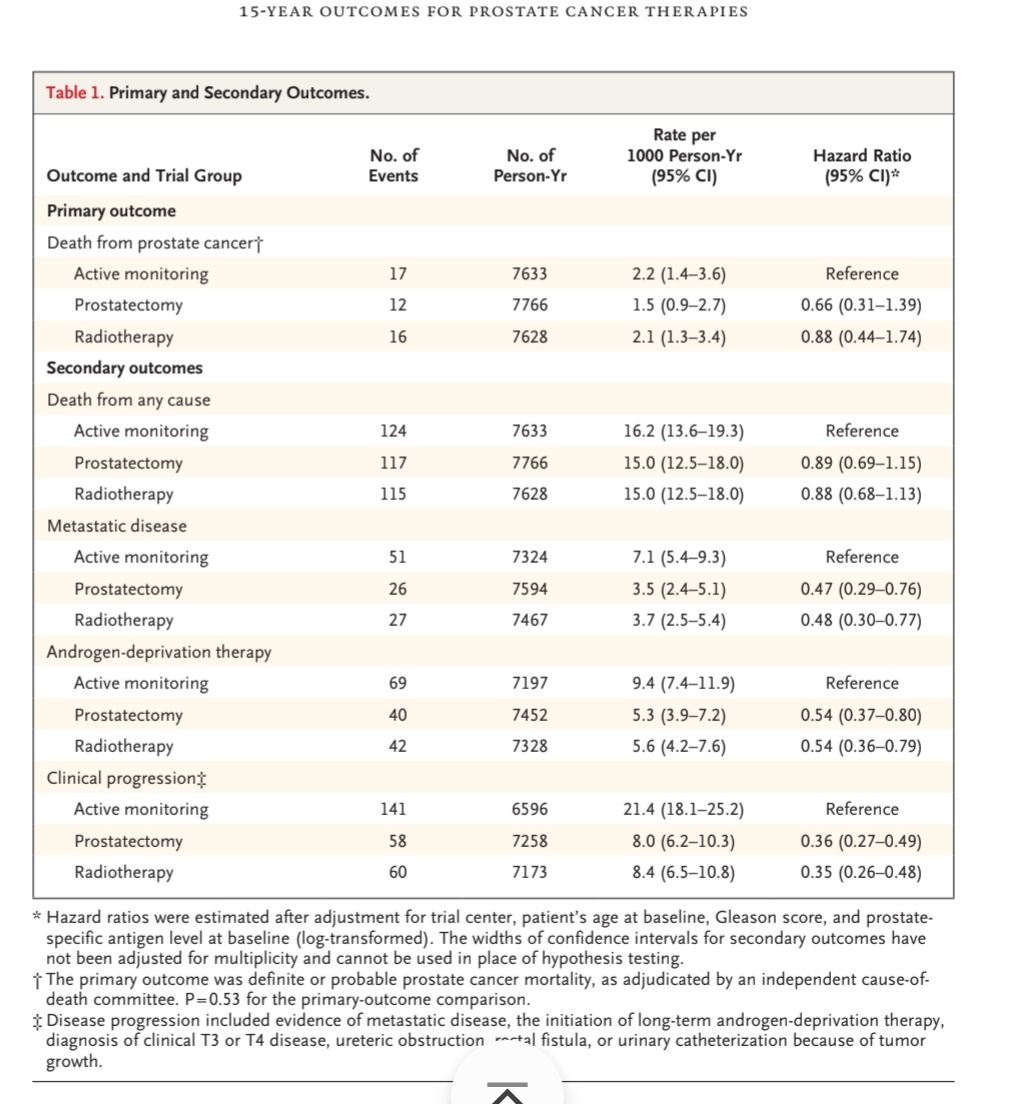
15yr f/u for #ProtecT_Trial just out!
•n=1610
•1/3 IR or HR by NCCN criteria
•n=45 DS deaths (AM17:RP12:RT16)
•n=104 mets (AM51:RP26:RT27)
•n=151 started ADT (AM69:RP40:RT42)
•62% of AS cross over to radical
Surprised? Or no surprises??
#EAU23#Oxford_Urology@BAUSurology
Guess this is key slide from Freddie's talk. It's given me a bit of an existential crisis over past 36hrs
Should we approach all localised #ProstateCancer like we now do salvageRT?
i.e. put EVERYONE on surveillance, then only treat those who 'progress'?? (1/3 were T3!)
#EAU23
Lymphedema after prostate cancer treatment? For many, it remains the forgotten vascular disease.
👉 Find out in our systematic review https://t.co/ETSobktE5O #mdpicancers via @Cancers_MDPI@joniau@EveraertsW@LisaMoris2
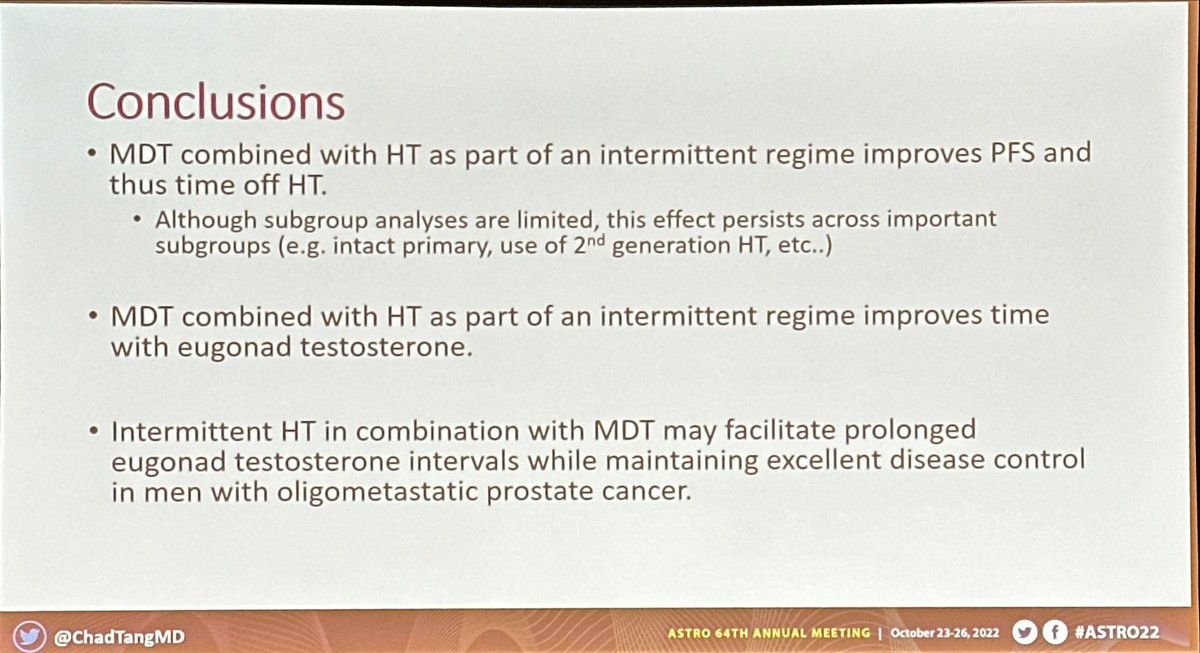
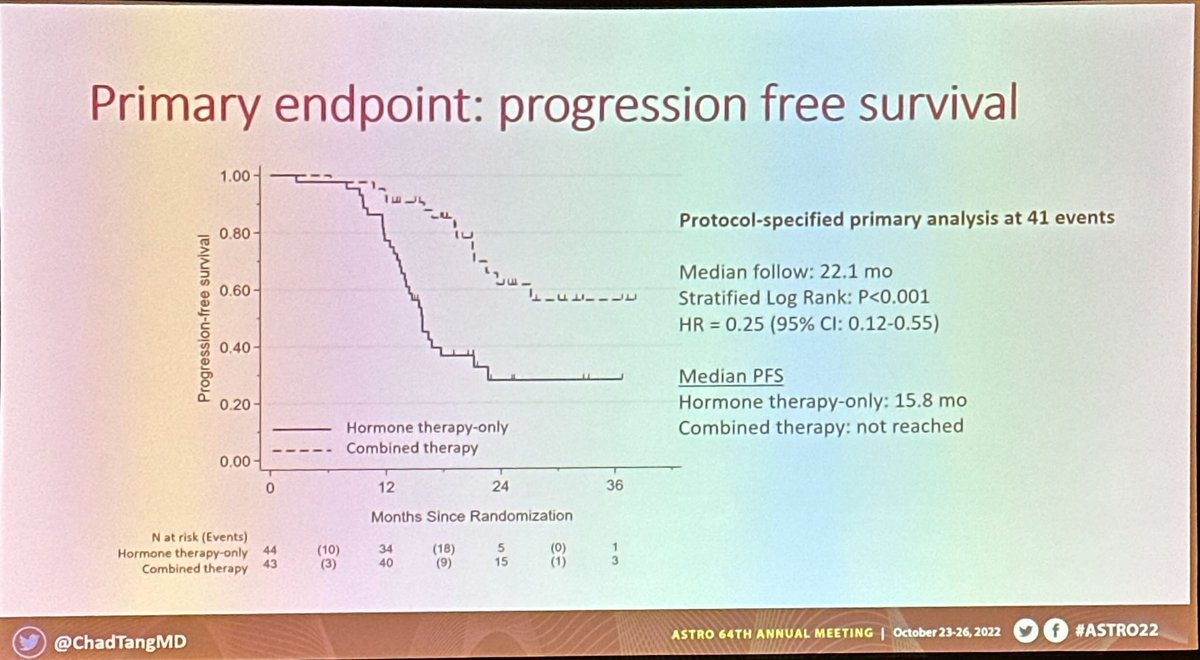
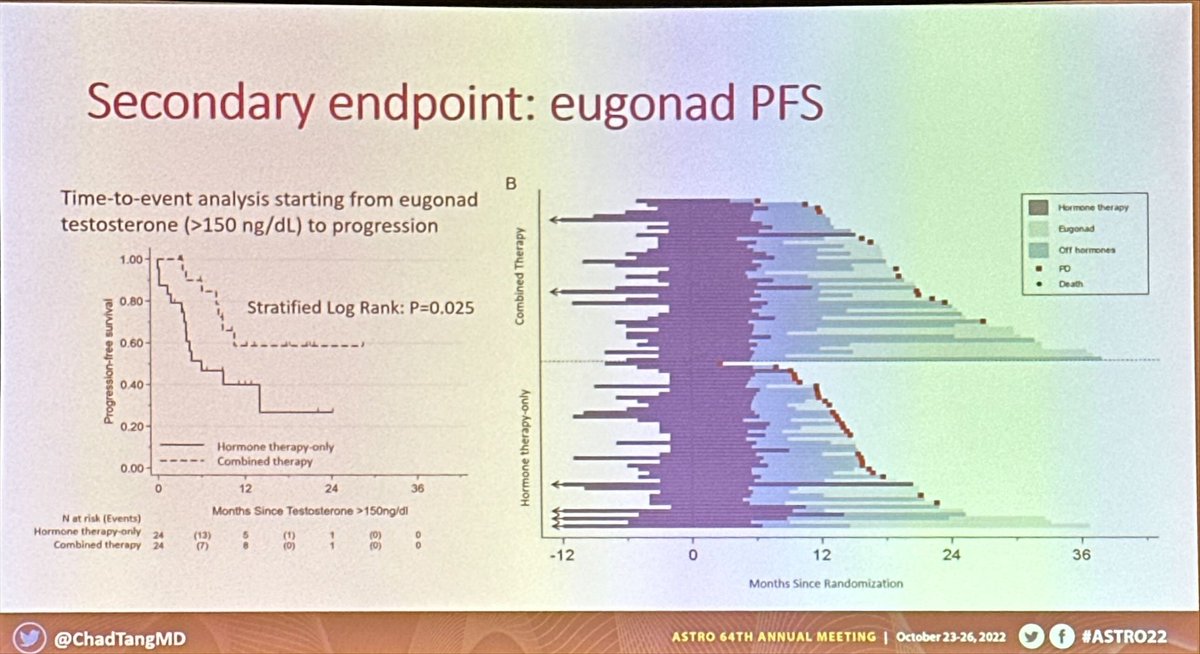
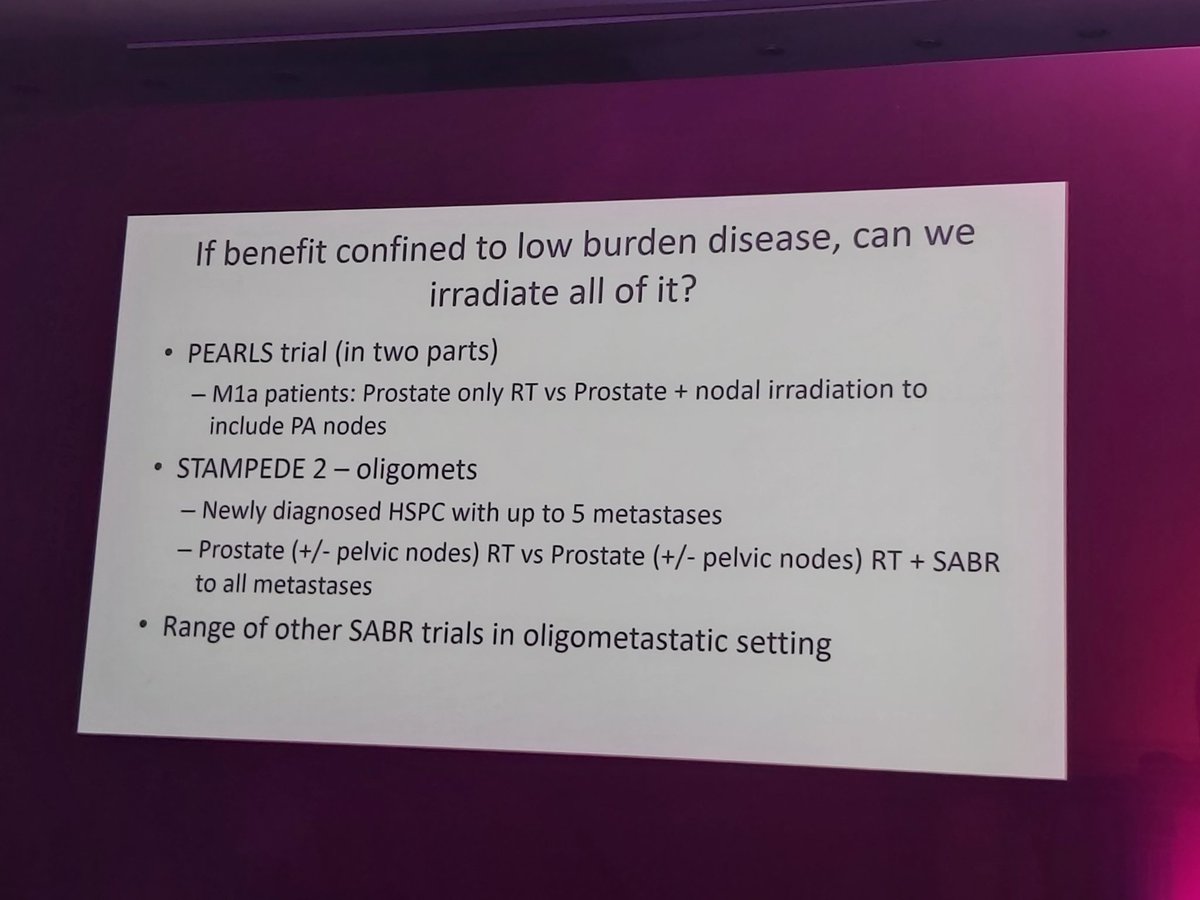
Late breaking abstracts #ASTRO22 - @ChadTangMD EXTEND trial; oligometastatic #prostatecancer. Intermittent ADT + SABR versus ADR alone extends PFS, but importantly time men enjoy off ADT in the long term (eugonadal PFS). Important patient centric endpoint! 👏🏽⭐️ @OncoAlert#pcsm
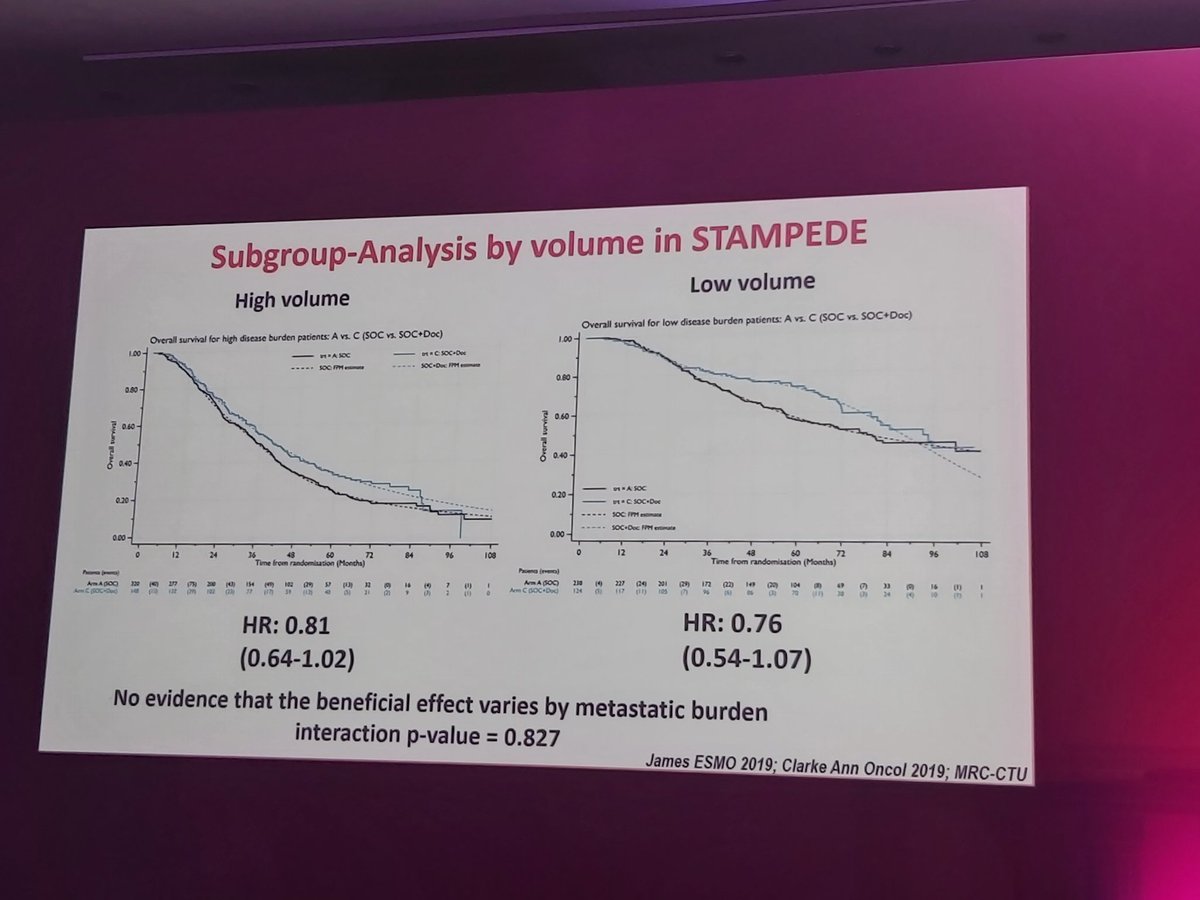
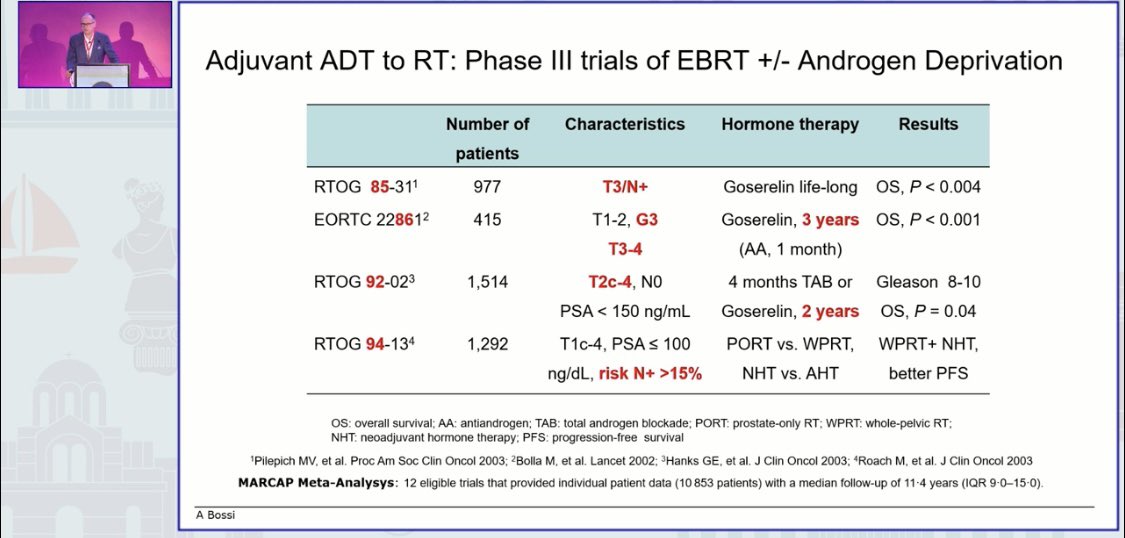
Some Stampede high risk patients might be cured with surgery alone instead of ‘suffering’ 2 years of intensified hormonal treatment. #PROSCA22@joniau excellent talk