This year (2024) has been a year of remarkable achievements for me during my residency training. It was an honour for me to collaborate with several supervisors in several projects or papers. Learning a lot of things while working on these projects.
...
📝 Narrative Review: #RightVentricle metrics, such as strain, fractional area change, and ejection fraction, offer mechanistic insight in cardiovascular trials but remain underused due to acquisition variability and lack of standardization.
Today's Paper of the Day is:
How I diagnose and treat cardiorespiratory complications of transfusion
https://t.co/JKgcYjlUQ5
Join us to read 1 paper per day and stay up-to-date as we cover the spectrum of critical care across 2026
Bridging the gap: adapting heart failure guidelines for resource-limited settings: A European Journal of Heart Failure expert consensus document
#EJHF@AmrAbdin10@GianluSava@HanCardiomd@GiuseppeGalati_
https://t.co/kJNcyXT1rj
💧 Fluid Management in Heart Failure and Cardiogenic Shock
Preload vs Congestion
This chapter explains that in acute and chronic heart failure, the challenge is not simply “giving or withholding fluids” but balancing preload to support cardiac output against the risk of venous congestion and pulmonary edema. Conventional preload markers (CVP, PAOP) are often misleading in dilated, stiff or ischemic ventricles, so the authors emphasize integrated assessment using echo, blood pressure, urine output and clinical signs of congestion.
Cardiogenic Shock Strategy
In cardiogenic shock, small, carefully tested fluid challenges may be justified early, but ongoing hypotension is usually better addressed with inotropes, vasopressors and mechanical support rather than repetitive fluid boluses. The chapter highlights how positive fluid balance worsens outcomes in decompensated heart failure and advocates early decongestive therapy and, when needed, ultrafiltration as part of a broader deresuscitation plan.
📘 Full chapter in Rational Use of Intravenous Fluids in Critically Ill Patients:
👉 https://t.co/7pvDxZGOUg
🔵 Discussed in depth at IFAD 2026 in Antwerp.
👉Registration: https://t.co/wATwBWBg5M
#HeartFailure #CardiogenicShock #FluidManagement #VEXUS #ICU
𝗦𝘂𝗴𝗴𝗲𝘀𝘁𝗲𝗱 𝗥𝗲𝘃𝗲𝗿𝘀𝗮𝗹 𝗦𝘁𝗿𝗮𝘁𝗲𝗴𝗶𝗲𝘀 𝗼𝗳 𝗢𝗿𝗮𝗹 𝗔𝗻𝘁𝗶𝗰𝗼𝗮𝗴𝘂𝗹𝗮𝗻𝘁 𝗨𝘀𝗲 𝗳𝗼𝗿 𝗠𝗮𝗷𝗼𝗿 𝗕𝗹𝗲𝗲𝗱𝗶𝗻𝗴 𝗮𝗻𝗱 𝗯𝗲𝗳𝗼𝗿𝗲 𝗘𝗺𝗲𝗿𝗴𝗲𝗻𝗰𝘆 𝗦𝘂𝗿𝗴𝗲𝗿𝘆.
As shown in Panel A, reversal management depends on the urgency of surgery or the invasive procedure. Reversal management includes administration of oral or intravenous (IV) vitamin K with or without 4F-PCC, depending on the timing of the procedure (emergency or urgent), baseline international normalized ratio (INR) value, and presence (or absence) of active bleeding. For patients receiving direct oral anticoagulants (DOACs), the decision also depends on time to surgery. Decision making is informed by DOAC type, time since last dose, half-life, presence (or absence) of active bleeding, and renal function tests to estimate residual drug activity.
Panel B shows reversal strategies for patients presenting with major bleeding while receiving an oral anticoagulant. The reversal strategy of vitamin K antagonists includes vitamin K given intravenously or orally, combined with 4F-PCC and INR testing. Management of anticoagulant reversal of direct oral FXaIs is based on four key factors (shown as the 4Ts): type of bleeding, timing of the last dose, thrombotic risk, and need for invasive procedures in the next 48 hours that would result in the administration of UFH. These factors may facilitate the use of specific (e.g., andexanet alfa) or nonspecific (e.g., 4F-PCC) antidotes. The reversal of dabigatran is informed by three clinical variables (shown as the 3Rs) — the type of bleeding, time of the last dose of dabigatran, and preserved renal function.
Learn more in the Review Article “Antidotes for Anticoagulation Reversal” by Bianca Rocca, MD, PhD, and Hugo ten Cate, MD, PhD: https://t.co/XobqwMebfy
NEJM subscribers: Explore this article deeper with AI Companion.
🏃♂️⚡ Can exercise stress testing (EST) improve the diagnosis and risk stratification of #BrugadaSyndrome?
A fascinating new state-of-the-art review highlights that exercise testing is much more than a tool for assessing exercise capacity. In Brugada syndrome, the *recovery phase* may be the key moment to uncover concealed disease and identify patients at higher arrhythmic risk.
🔍 Key takeaways:
✅ Type 1 Brugada ECG pattern is rarely unmasked during peak exercise (~1%) but becomes evident in up to 25% of patients during early recovery.
✅ The transition from sympathetic activation to parasympathetic rebound appears to play a crucial role in ECG changes and arrhythmogenesis.
✅ Premature ventricular contractions (PVCs) occurring during early recovery may represent an important marker of future ventricular fibrillation risk.
✅ Exercise-induced malignant arrhythmias are rare, suggesting that EST is generally safe when performed with appropriate monitoring.
✅ Careful ECG monitoring during the first minutes of recovery may provide valuable diagnostic and prognostic information.
💡 The review supports the concept that both *peak exercise* and *early recovery* offer complementary insights into the electrophysiological substrate of Brugada syndrome and may help refine individualized risk assessment.
An important reminder that sometimes the most informative part of a stress test is not the exercise itself—but what happens immediately afterwards.
#BrugadaSyndrome #Electrophysiology #Cardiology #InheritedCardiacConditions #SuddenCardiacDeath #Arrhythmias #SportsCardiology #ExerciseTesting #ECG #RiskStratification #PrecisionMedicine #JACCAsia
@MAbdullah58266 Thanks for sharing Doc! I've got the similar case last week. Biventricular circumferential hypertrophy, pericardial effusion, thickening AV valve and pleural effusion.
🚨Cardiac Intensive Care Unit appropriate patient selection and triage
This is a MUST read for everyone working on Intensive Care ! 🤩
Kudos to the authors for such an outstanding work 🙌🏻 @AdrianaCLuk@carlosalviar@AnnGageMD@seanvandiepen@AHAScience
Full article here: https://t.co/61OesJPp7Z
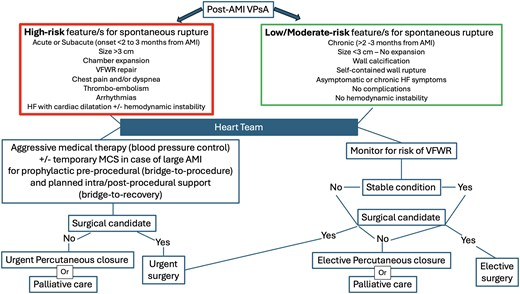
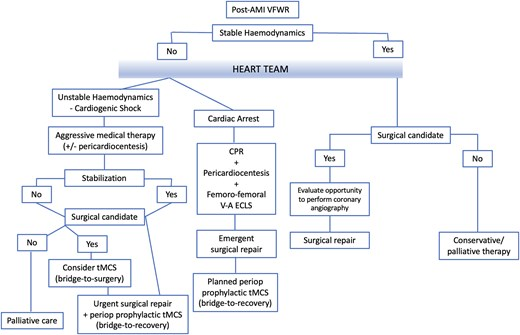
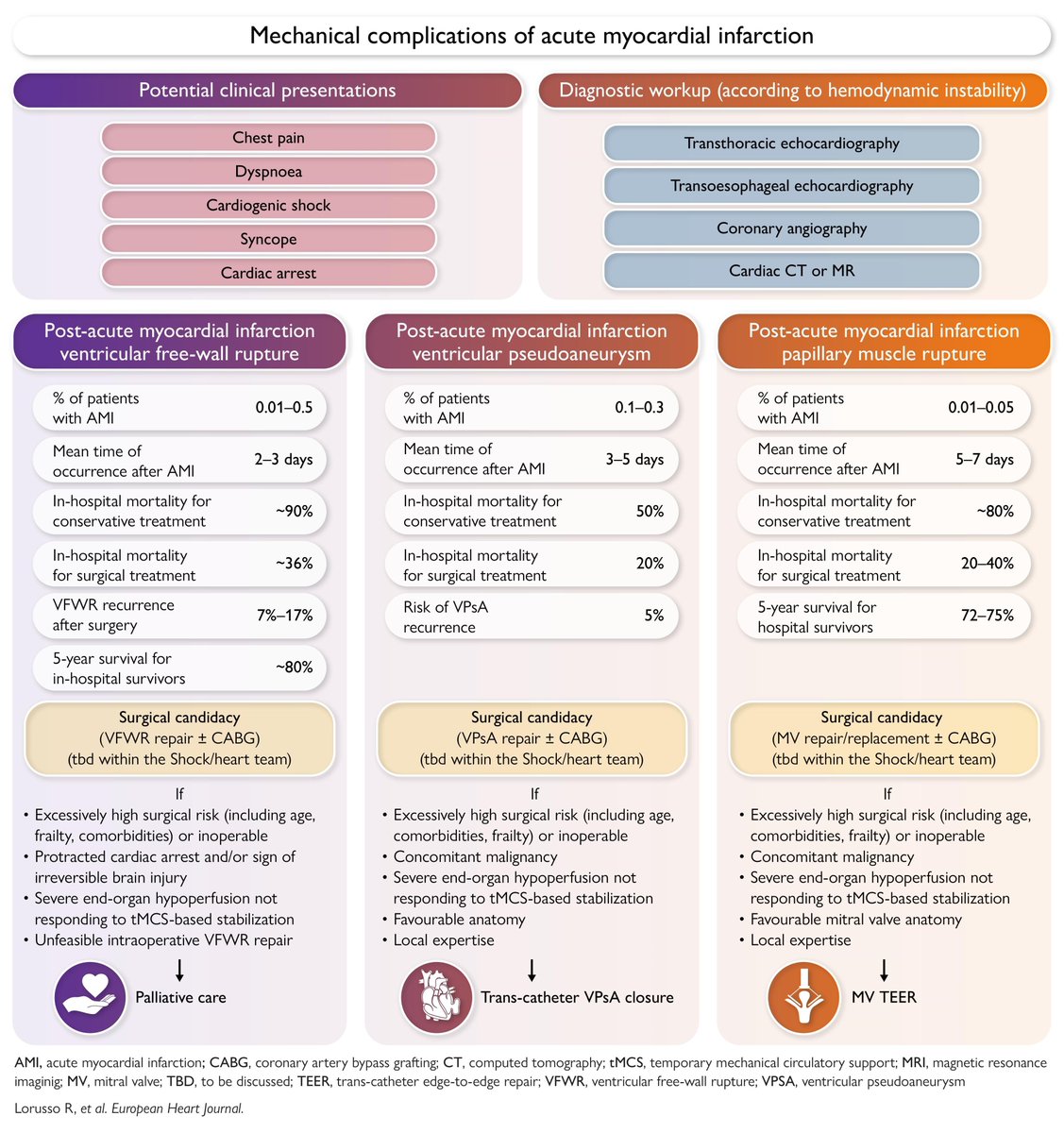
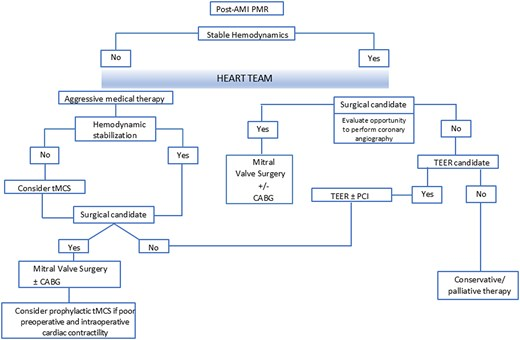
📌Ventricular free-wall rupture, ventricular pseudoaneurysm & papillary muscle rupture complicating acute myocardial infarction
A clinical consensus statement of the @escardio & @EACTS#PositionPaper#MechanicalComplications#MI
Open access books can be downloaded using this QR code. Content also appears weekly in @JACCJournals Thank you to @HRSonline for making this a special annual component of HRS for all EP’s.
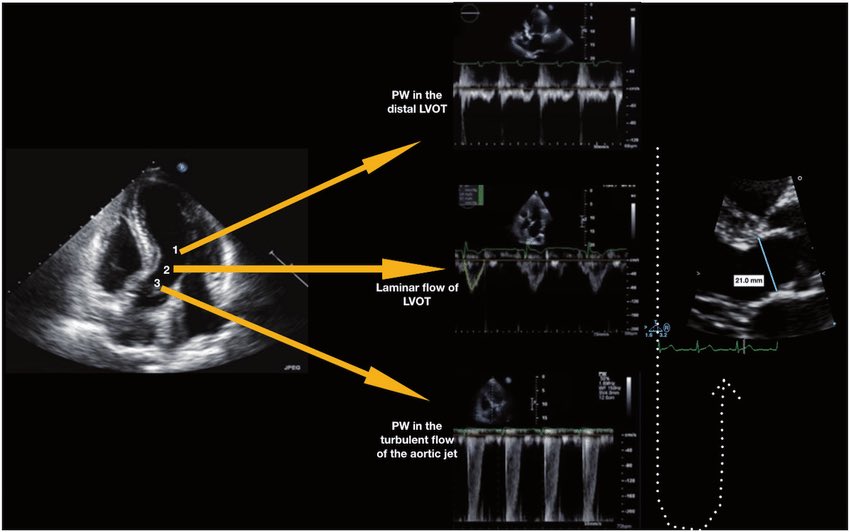
🫀 Did you know where the recommendation to place the pulsed wave Doppler sample volume 0.5–1 cm from the aortic valve to measure LVOT VTI comes from?
The answer is more interesting than it seems. It doesn’t come from a single study or an experiment designed for that purpose. It comes from a historical chain spanning nearly 40 years:
🔬 1982–1984 — The physical foundation
Pasipoularides and Murgo demonstrated using invasive catheters and mathematical models that in aortic stenosis there is a real zone of flow acceleration in the LVOT, just proximal to the valve, without any second anatomic obstruction. Pure hemodynamics — no Doppler yet.
👉 Bird et al. Circulation 1982 → https://t.co/oCXGNgWsPF
👉 Pasipoularides et al. Am J Physiol 1984 → https://t.co/cfvNMpEgzG
📐 1984 — The apical 5-chamber view
Lewis, Kuo and Quinones were the first to validate cardiac output measurement using pulsed wave Doppler from the cardiac apex. They described placing the sample volume “immediately proximal to the aortic valve leaflets” — but without specifying any distance in centimeters.
👉 Lewis et al. Circulation 1984 → https://t.co/lRVjLuYMEs
📏 1985 — The first numerical distance
Skjaerpe, Hegrenaes and Hatle (the Norwegian group) were the first to quantify this in Doppler: they empirically observed that flow acceleration began 0.5 to 1.5 cm proximal to the valve, and placed the sample volume just proximal to that zone. They directly cited Pasipoularides as supporting evidence. This was the first time a numerical distance appeared in the technique.
👉 Skjaerpe et al. Circulation 1985 → https://t.co/rf7l2FQUs4
📊 1986–1988 — Practical consolidation
Otto et al. used ~1.0 cm. Oh, Tajik and the Mayo Clinic group explicitly established the range of 0.5 to 1.0 cm in 100 patients, justifying it as necessary to avoid the subvalvular acceleration zone. This is the figure we all recognize today.
👉 Otto et al. JACC 1986 → https://t.co/avke1qOy4x
👉 Zoghbi et al. Circulation 1986 → https://t.co/KFiChfBNuc
👉 Oh et al. JACC 1988 → https://t.co/1C8sHRSMPq
📋 2002 — It becomes “official”
Quinones, Otto, Zoghbi and colleagues codified it in the ASE guidelines as “~5 mm proximal to the aortic valve”… but without citing any specific study to support it. It had already become expert consensus.
👉 Quiñones et al. JASE 2002 → https://t.co/U3hXFns4jx
⚔️ 2017 — The debate reopens
Baumgartner et al. (EACVI/ASE) maintained the 0.5–1 cm recommendation. However, Hahn and Pibarot responded with a critical letter pointing out that the original articles from the 1980s measured at the aortic annulus, not 0.5–1 cm below it, and that moving away from the annulus introduces errors due to the elliptical and irregular shape of the subannular LVOT.
👉 Baumgartner et al. Eur Heart J Cardiovasc Imaging 2017 → https://t.co/iu07xBTwQS
👉 Hahn & Pibarot. JASE 2017 → https://t.co/uqgcv8kzO7
💡 Bottom line:
The 0.5–1 cm figure was never experimentally validated as the optimal distance. It emerged from empirical observations in the 1980s aimed at avoiding a flow acceleration zone that had been demonstrated with invasive catheters. It was adopted through accumulated clinical practice and later elevated to a formal recommendation by consensus. The debate over whether to measure at the annulus or 0.5–1 cm below it remains open to this day.
One of those recommendations we all follow but few know where it actually came from 🙂
Dr Benigno Valderrábano Salas
@MDBeni@JaeKOh2@ottoecho@WilliamZoghbi@ASE360@EACVIPresident@NephroP@iamritu@PPibarot@hahn_rt@MAecocardio@SISIACOficial@SONECOM_AC@VazyurVasquez@Cardiotweets83@HEARTof_echo@echobasics
GOODBYE POWERPOINT. 🚨
Claude can now create a full presentation in just 120 seconds.
No slides. No stress.
Use these 6 prompts and watch the magic happen.