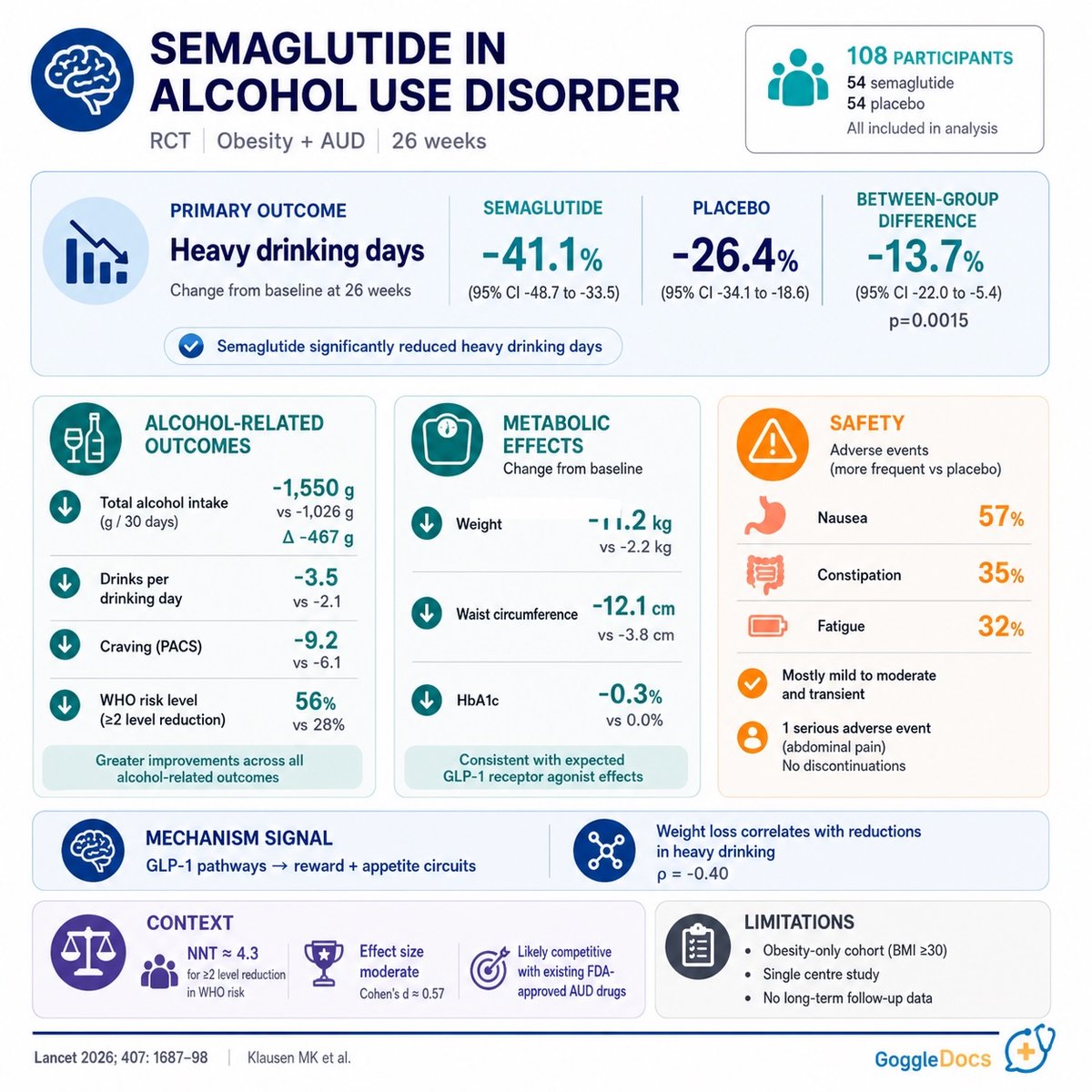
🍷 First RCT of semaglutide 2.4mg in treatment-seeking patients with alcohol use disorder + obesity
n=108
26 weeks
semaglutide + CBT vs placebo + CBT
Primary endpoint (% heavy drinking days):
🔹 Semaglutide: -41.1pp
🔸 Placebo: -26.4pp
🔹 Difference: -13.7pp (p=0.0015)
Secondary endpoints consistent: total alcohol intake, drinks per drinking day, WHO risk level, craving all favoured semaglutide. Phosphatidyl ethanol supported self-report.
Safety: GI AEs higher (nausea 57% vs 7%). 4 vs 1 discontinued for AEs. No pancreatitis.
Caveats: BMI ≥30 only, single centre, no post-trial follow-up. Weight loss correlated with drinking reduction (ρ=-0.40).
Moves beyond hypothesis-generating. Replication needed before off-label use.
Heart attacks are often preventable with early risk awareness and lifestyle changes.
Healthcare is evolving, with AI playing a growing role in prevention and care.
#MedTwitter#Cardiology#Prevention#AIinHealthcare
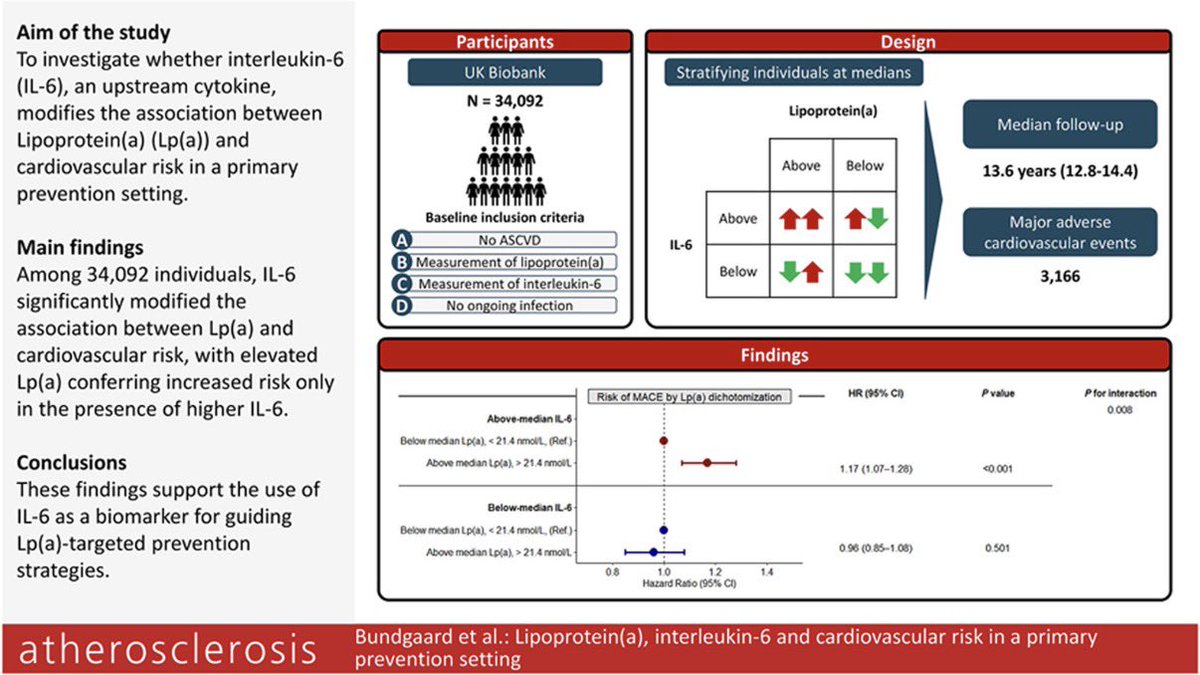
Lipoprotein(a), interleukin-6 and cardiovascular risk in a primary prevention setting
☝️New data from UK Biobank (n=34,092): In primary prevention, the cardiovascular risk associated with elevated Lp(a) was significantly influenced by IL-6, a key upstream inflammatory cytokine.
1️⃣ Higher Lp(a) increased MACE risk only when IL-6 was elevated (HR 1.17; 95% CI 1.07–1.28), while no significant association was seen when IL-6 was below median levels.
2️⃣ Inflammation appears to amplify Lp(a) pathogenicity, supporting the concept that not all elevated Lp(a) carries the same biological risk burden.
3️⃣ hs-CRP did not show the same modifying effect, suggesting IL-6 may be a more informative biomarker than conventional inflammatory markers for Lp(a)-related risk stratification.
4️⃣ Clinical implication: Future Lp(a)-lowering therapies may yield greatest benefit in individuals with concomitant elevated IL-6, enabling more precise preventive targeting.
👉 Elevated Lp(a) appears to confer its greatest cardiovascular hazard in the presence of heightened IL-6–mediated inflammation, supporting a biologically integrated model in which inherited atherothrombotic burden and residual inflammatory risk act synergistically
@ATHjournal@society_eas
🔗 https://t.co/dEWhC0JpAm
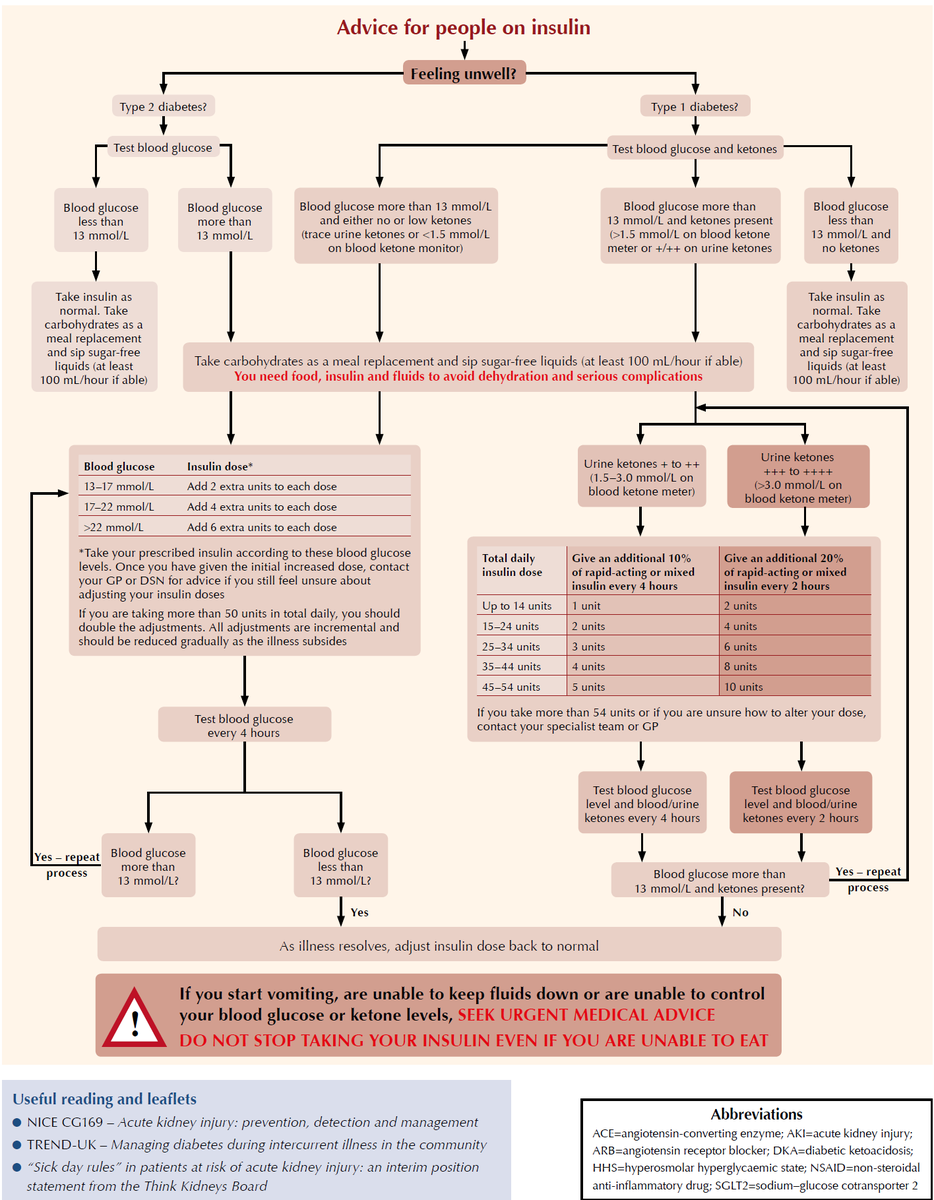
A "sick day" guide for managing blood glucose and insulin doses when you're feeling unwell. It outlines different protocols depending on whether you have Type 1 or Type 2 diabetes.
https://t.co/yTKwGJjOwW
Managing DKA in adults starts with recognizing that the risks have changed.
Experts share why the "frail and elderly" are now a primary concern for recurrent episodes and how to tighten insulin consistency.
Watch the full discussion for more clinical pearls ➡️ https://t.co/0qa4pVFieW
#CME
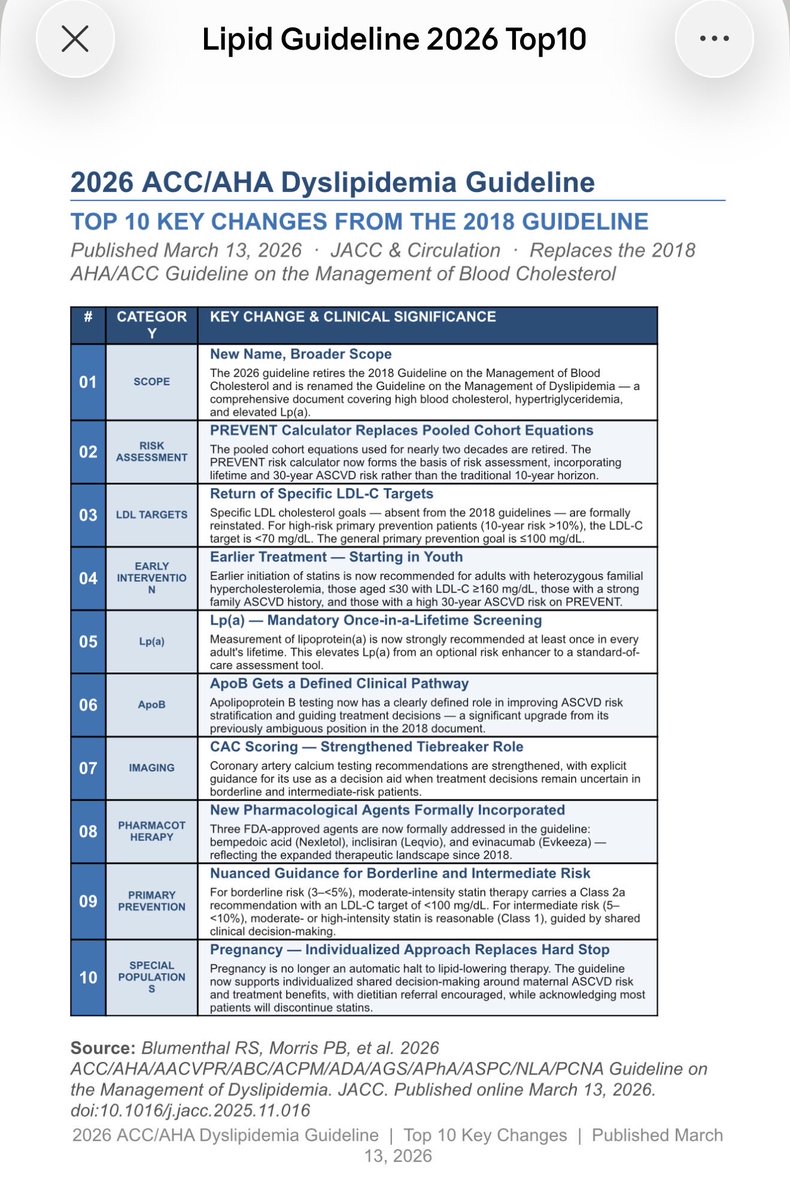
1 minute review for top 10 changes in 2026 lipid guidelines 🫀
Shared decision making always worked for me , patient compliance is great when you give them autonomy and a plan for decade !
@ACCinTouch
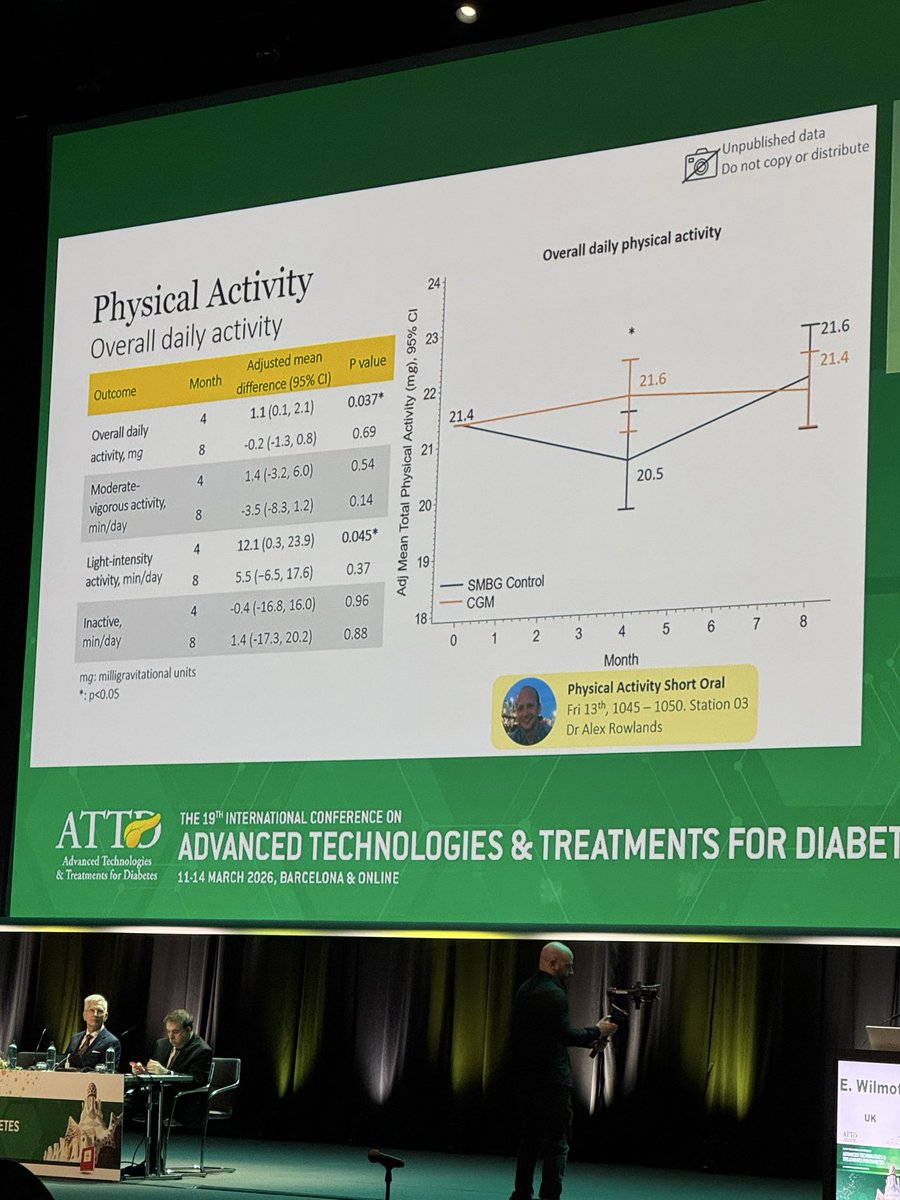
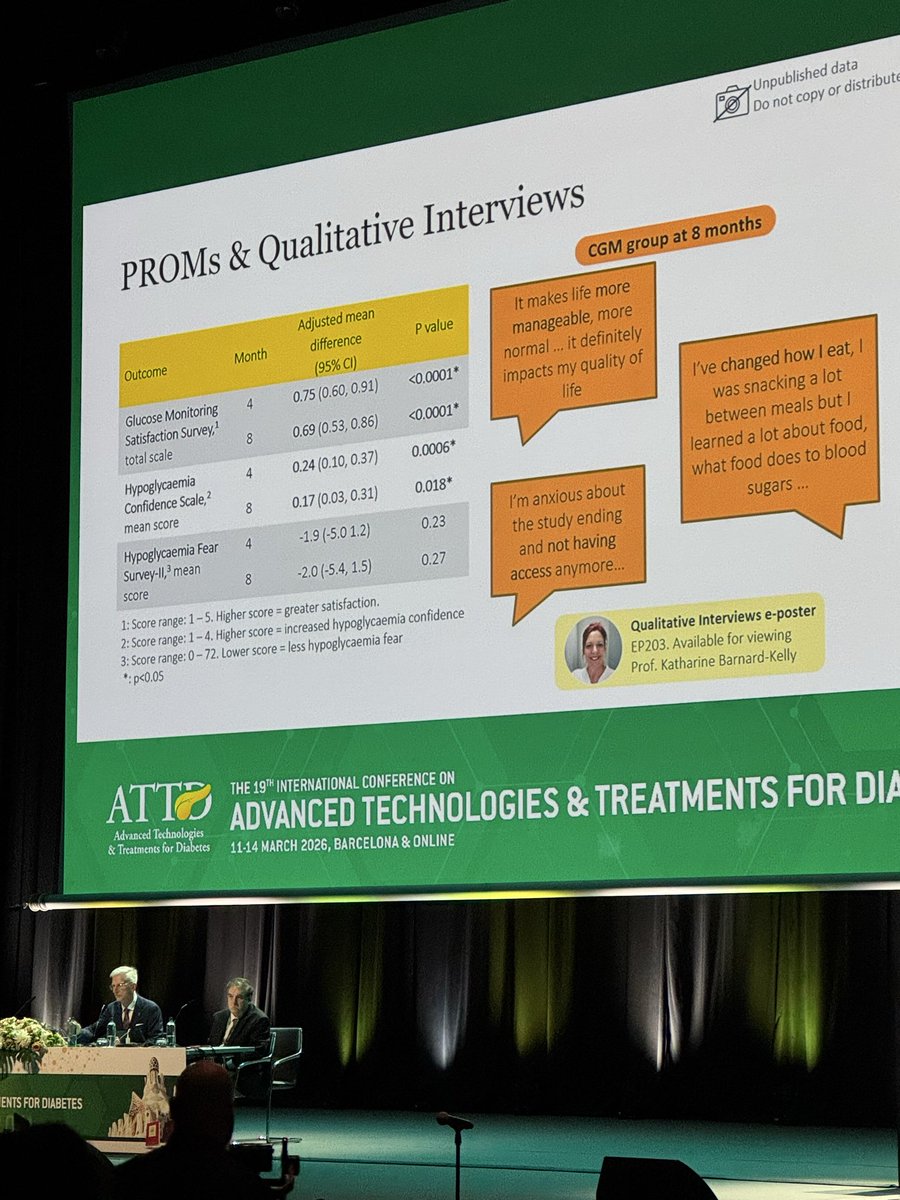
❗️Knowledge (of glycaemia) is power❗️
FREEDOM2 trial presented by @WilmotEmma#ATTD2026@ATTDconf
🔹CGM in those with T2DM on basal
Insulin
🔸⬇️Hba1c at 4 and 8 months
🔹Improved sensor metrics/glycaemic profiles
🔸No increased hypoglycaemia 🚫
🔹No change Total Daily Insulin dosing
🔹Interesting patient reported outcomes and dietary/exercise data
@AmarPut@drpatrickholmes@kamleshkhunti@TBattelino
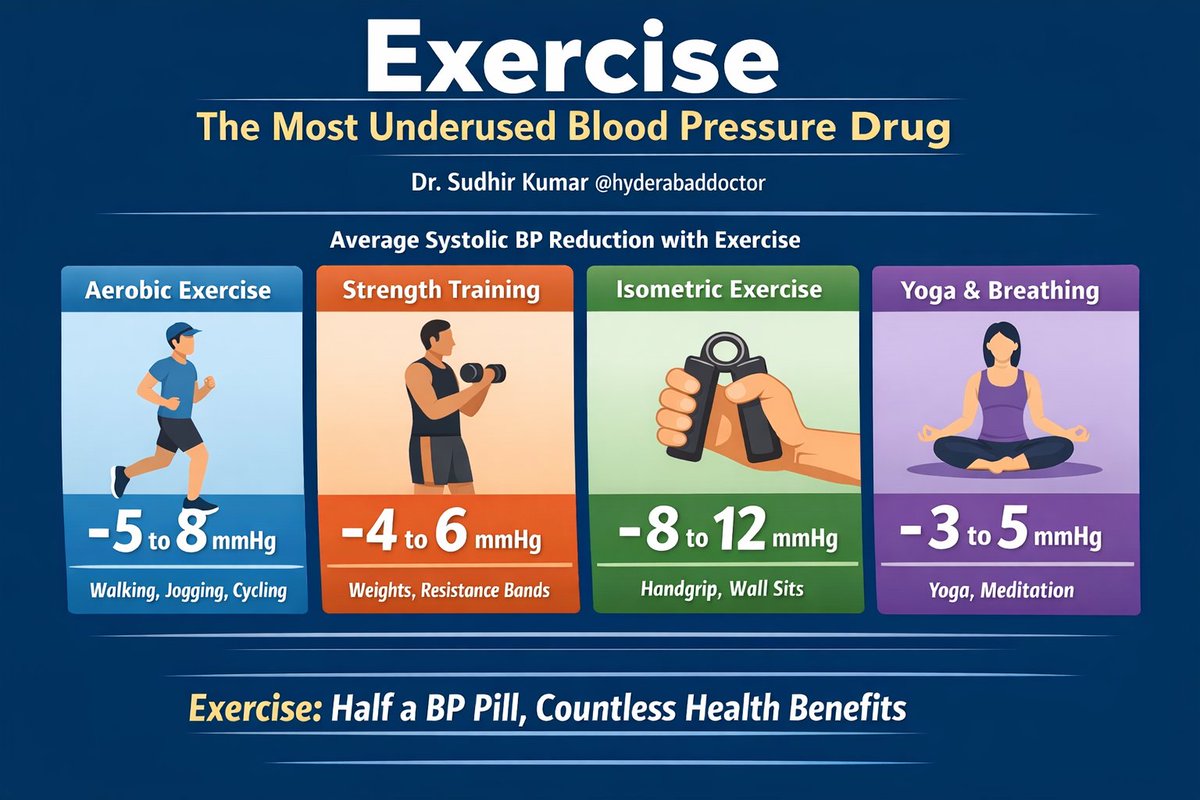
Exercise: The Most Underused Blood Pressure Drug
As a neurologist, I often tell patients this:
If exercise were a pill, it would be one of the most widely prescribed drugs in the world.
Because the effect of exercise on blood pressure is real, measurable, and surprisingly large.
Let us look at what the evidence shows.
▶️How much can exercise lower BP?
Different forms of exercise lower blood pressure to different degrees.
1. Aerobic exercise (brisk walking, jogging, cycling, swimming)
• Average reduction: 5–8 mmHg systolic
• Works in both hypertensive and normotensive individuals
• 30–45 minutes, most days of the week
Even a 5 mmHg drop reduces stroke risk by about 14%.
2. Resistance training (weight training, resistance bands)
• Reduction: 4–6 mmHg systolic
• Also improves insulin sensitivity and metabolic health
Best when done 2–3 times per week along with aerobic exercise.
3. Isometric exercise (wall sits, handgrip exercises)
Surprisingly powerful.
• Reduction: 8–12 mmHg systolic in some studies
• One of the largest BP reductions seen with exercise
Example: handgrip exercise for 2 minutes × 4 sets, several days per week.
4. Yoga / slow breathing / pranayama
• Reduction: 3–5 mmHg on average
• Helpful particularly in stress-related hypertension
Works best as an adjunct, not a replacement.
✅When is exercise alone enough?
Exercise alone may control BP in:
• High-normal BP (130–139 / 85–89)
• Stage 1 hypertension without other risk factors
• Younger individuals with sedentary lifestyle
In these cases, 3–6 months of lifestyle therapy may normalize BP without drugs.
▶️When exercise must be combined with medicines?
Lifestyle alone is usually not enough when:
• BP ≥160/100 mmHg
• Diabetes, kidney disease, or prior stroke
• Multiple cardiovascular risk factors
• Long-standing hypertension
Here, exercise becomes a powerful add-on therapy, often allowing lower drug doses.
✅A useful perspective
Typical BP reduction with:
• One antihypertensive drug: ~10 mmHg systolic
• Regular exercise: ~5–8 mmHg
So exercise is roughly half a BP pill, but with dozens of additional health benefits.
✅Bottom line
The most effective “exercise prescription” for BP:
• 150 minutes/week aerobic exercise
• 2–3 sessions/week resistance training
• Add isometric exercises or yoga
Dr Sudhir Kumar
@hyderabaddoctor
Nice article in The Print discussing emerging evidence that GLP-1 drugs used for diabetes and obesity may also help reduce addiction to alcohol and smoking by influencing the brain’s reward pathways. Thank you Sneha Richhariya for quoting me in this.
https://t.co/AcxyH309vP
@ThePrintIndia@RichhariyaSneha
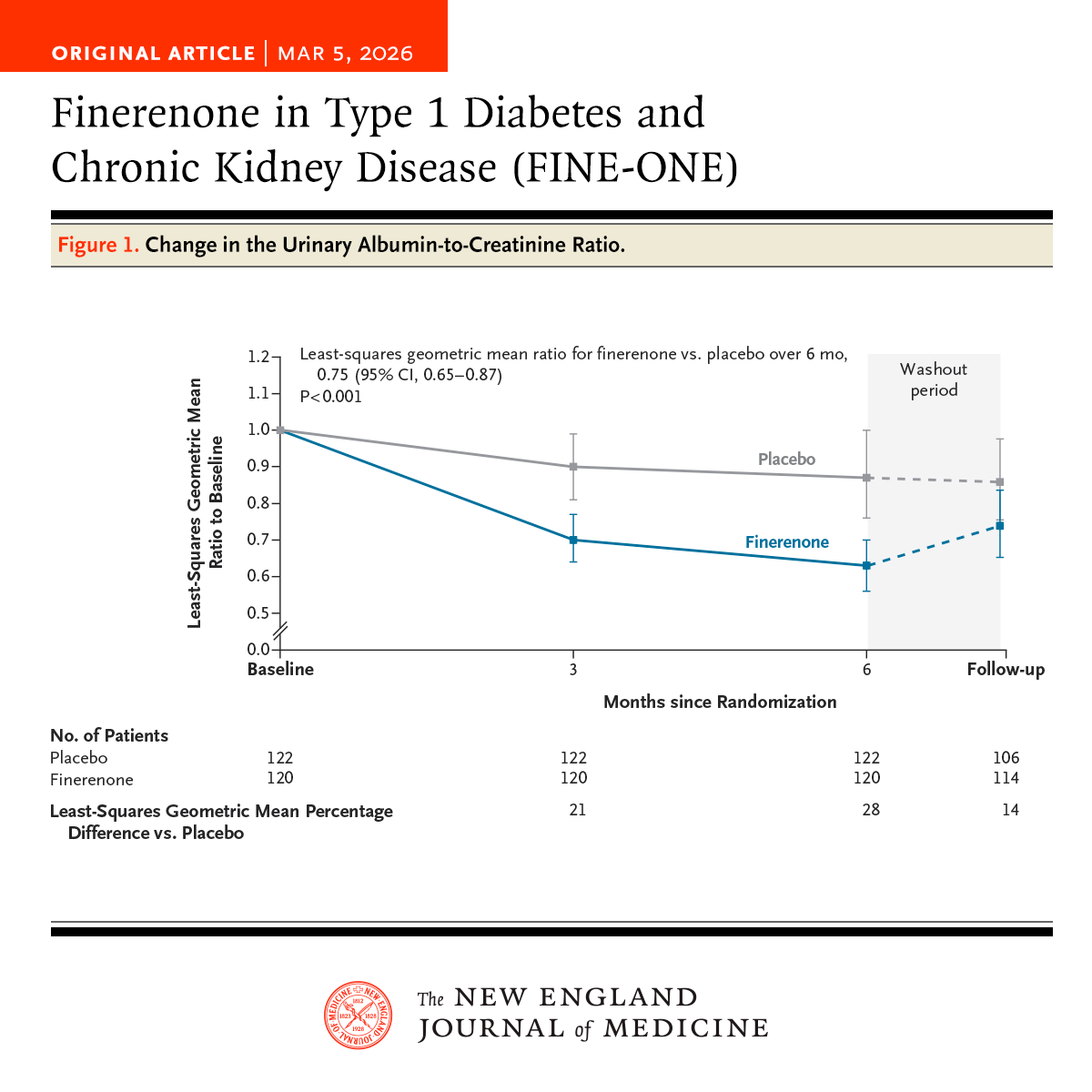
In adults with type 1 diabetes and chronic kidney disease with albuminuria, the decrease in the urinary albumin-to-creatinine ratio was significantly greater with finerenone than with placebo. Full phase 3 FINE-ONE trial results: https://t.co/E2ThxUUtfX
Editorial: Finerenone for Diabetic Kidney Disease in Type 1 Diabetes — A Fine Answer? https://t.co/xUQ07dMJwt
"Just stop taking it and keep the weight off."
That's not how chronic disease works.
I just published the most comprehensive breakdown of what actually happens — hormonally, metabolically, neurologically — when you stop GLP-1 therapy.
48 studies. 9,000+ patients. 3 meta-analyses.
Here's what the data show:
→ 60% of lost weight returns within 1 year
→ Regain starts within weeks — not months
→ Your hormones fight you for YEARS after weight loss
→ But the regain curve decelerates. ~25% of the benefit may persist.
→ And reduced-dose maintenance strategies are showing real promise.
This isn't a willpower problem. It's a biology problem. And the science is not ambiguous.
Full article:
https://t.co/j1Djn3McMZ
↪️ https://t.co/pAVWtSE5PV
#SubstanceOverNoise #GLP1 #ObesityMedicine
BELIEVE phase 2 trial with #bimagrumab, an antibody that blocks activin type II receptors to reduce fat mass, prevent #sarcopenia and promote skeletal muscle growth, plus semaglutide 2.4 mg produced 22% weight loss at 48–72 weeks, with ~93% of loss from fat mass and preserved/increased lean mass.
https://t.co/UXws88VPb4
New study finds a sweet spot of 7 hours 18 minutes of sleep a night for lowest insulin resistance risk. Too little or too much sleep raises risk, and big weekend “catch-up” sleep may actually worsen glucose metabolism if you already get enough during the week.
https://t.co/mouKX5TjM0
Useful 👇👇👍👍
Joint TOS/OMA/OAC Expert Guidance Statement on the Pharmacological Management of United States Adults With Overweight or Obesity Using the GRADE Approach - Alexander - Obesity - Wiley Online Library https://t.co/LKYFaK90ub