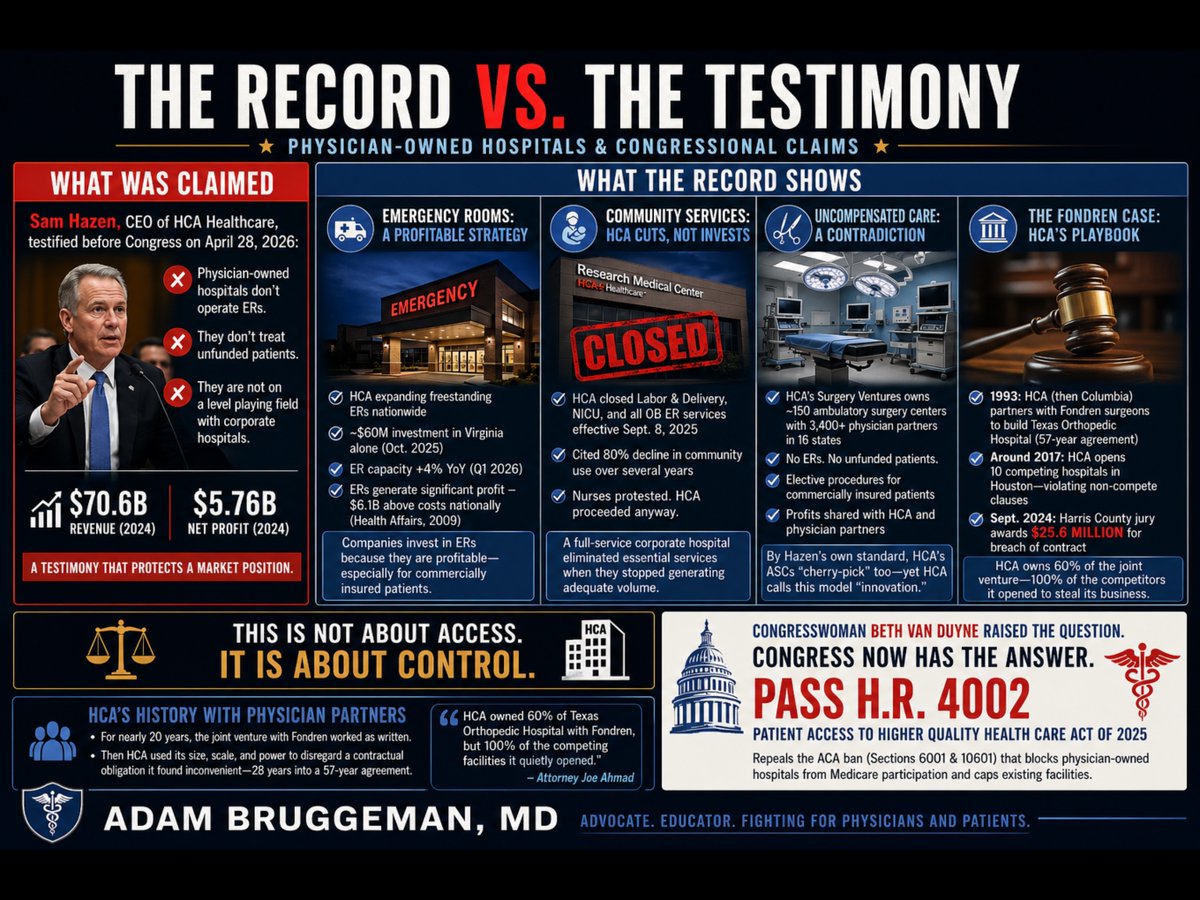
Yesterday, Sam Hazen, CEO of HCA Healthcare, sat before the House Ways and Means Committee and argued that physician-owned hospitals are not on a level playing field with corporate hospitals because they lack functioning emergency rooms and do not treat unfunded patients. Hazen delivered this argument while representing a company that posted $70.6 billion in revenue and $5.76 billion in net profit in 2024. He was not offering a neutral observation about healthcare access. He was protecting a market position.
Congresswoman Van Duyne did not let the testimony pass unchallenged. She pointed directly to HCA's own Research Medical Center in Kansas City, Missouri, which closed its labor and delivery unit, its neonatal intensive care unit, and all associated obstetrics emergency services effective September 8, 2025. HCA cited an 80 percent decline in community use of those services over several years as its justification. Nurses at the facility publicly protested the planned shutdowns and called on HCA to reverse course. HCA proceeded anyway. That is a full-service corporate hospital making a purely financial decision to eliminate essential community services when they stopped generating adequate volume. The same CEO who told Congress that physician-owned hospitals fail community obligations made that decision.
The emergency room argument deserves particular scrutiny. Mr. Hazen's implication is that operating an ER is a financial burden that justifies the premium reimbursement HCA collects across its outpatient system. The capital record contradicts that framing entirely. In January 2024, Hazen personally told HCA investors that the company's freestanding emergency room capacity would "grow consistently" in 2024 and 2025 to meet rising patient demand. In October 2025, HCA committed nearly $60 million to construct three new freestanding emergency rooms in Virginia alone, expanding its footprint there from eight to eleven standalone ER facilities. HCA has simultaneously been opening freestanding ERs in South Carolina, Florida, and throughout its other markets. In the first quarter of 2026, HCA reported that its emergency room capacity grew 4 percent year-over-year. A peer-reviewed analysis published in Health Affairs found that hospital emergency department revenue exceeded costs by $6.1 billion nationally as far back as 2009, a margin of 7.8 percent overall, with privately insured ED patients generating $17 billion in profit. Companies do not invest tens of millions of dollars in freestanding emergency infrastructure because that infrastructure is a burden. They expand aggressively into emergency care because it is profitable, particularly for commercially insured patients. When physician-owned hospitals choose not to operate ERs, they are not avoiding a community obligation. They are declining to compete in HCA's most profitable and most aggressively expanded service line.
The uncompensated care argument carries an equally significant contradiction. Through its Surgery Ventures division, HCA jointly owns and operates approximately 150 ambulatory surgery centers with more than 3,400 physician partners across 16 states. Those ambulatory surgery centers have no emergency rooms. They do not accept unfunded patients. They perform elective procedures on commercially insured patients and return profits to both HCA and its physician co-owners. By the precise standard Mr. Hazen applied to physician-owned hospitals before the Ways and Means Committee, his own company's Surgery Ventures facilities are doing exactly what he described as an unfair advantage. The distinction HCA is actually drawing is not between facilities that serve whole communities and those that do not. It is between facilities that HCA controls and those that it does not. When physicians own a hospital independently, HCA calls it cherry-picking. When HCA installs those same physicians as partners in ASCs under its corporate umbrella, it calls it innovative care delivery.
The history of how HCA treats physician partners outside of its direct control is documented in a Harris County, Texas courtroom. Fondren Orthopedic Ltd., a group of orthopedic surgeons, entered a limited partnership with what was then Columbia Hospital Corporation in 1993 to jointly own and operate Texas Orthopedic Hospital in Houston. The agreement ran for 57 years. For roughly two decades it functioned as written. Around 2017, HCA, which had assumed Columbia's position, began employing orthopedic surgeons at competing facilities across the Houston area, ultimately opening 10 competing hospitals offering the same services as the joint venture, in direct violation of the non-compete provisions of the partnership agreement. Simultaneously, HCA invoked those same non-compete clauses against the Fondren physicians, blocking them from doing what HCA was openly doing. In September 2024, a Harris County jury returned a verdict of $25.6 million against HCA for breach of contract. Lead attorney Joe Ahmad stated publicly that HCA owned 60 percent of Texas Orthopedic Hospital with Fondren, but 100 percent of the competing facilities it quietly opened to redirect patients away from their jointly held hospital. The jury found that HCA had the size, the scale, and the power to disregard a contractual obligation it found inconvenient, approximately 28 years into a 57-year agreement.
The legislative response is already written. H.R. 4002, the Patient Access to Higher Quality Health Care Act of 2025, introduced by Congresswoman Van Duyne and Congressman Henry Cuellar (D-TX-28), would repeal Sections 6001 of the Affordable Care Act, which banned new physician-owned hospitals from Medicare participation in 2010 and capped existing facilities at their March 2010 capacity. That ban was not derived from patient outcome data. It was a lobbying achievement. The evidence accumulated in the 15 years since passage shows that physician-led facilities consistently deliver care at lower cost with higher patient satisfaction than large corporate systems.
Thank you @RepBethVanDuyne for being a champion for patients, physicians, and communities!
@CharlesTe@drjohnm This is my go to. No one knows about costplus. I use it regularly. Interestingly, when I tell patients about this option vs continuing eliquis because of it's better safety and efficacy profile, most patients choose to stay on eliquis.
At Northwell since 2015:
105K strokes, 32% diagnosed with Afib at some point
The “reverse”:
655K patients with Afib diagnosis, 7,4% had a stoke
Afib ablation:
2,293 patients with Afib ablation
3.5 years follow up
21 (0.9%) had a stroke
13 (62%) while on anticoagulation
Some of this data published, the rest under publication
https://t.co/INde4bHHcP
Hospitals are putting hard caps on physician compensation, sometimes as low as the 75th percentile, and calling it fraud and abuse protection.
Think about what that means. If earning above the 90th percentile is inherently suspicious, then 10 percent of every physician in every specialty must be breaking the law. At the 75th percentile, 25 percent of all physicians are apparently committing fraud. That logic falls apart the moment you say it out loud.
Health law attorney Dennis Hursh has been reviewing these clauses for years, and he says they are showing up in the majority of physician employment contracts now. Some contracts say compensation "may be reviewed" if it exceeds the threshold. Others are blunt: under no circumstances will your total compensation exceed this number.
So if you are the most productive physician in your specialty in the entire country, your pay is frozen. Every dollar you produce above that cap flows to the institution. And as Hursh puts it, the CEO's bonus is not capped.
It gets worse. Most hospitals are not giving physicians clear, timely productivity data. You might be told you produced 9,500 WRVUs, but without access to the actual benchmarks, you have no idea whether you are approaching the cap. You are flying blind while working at a pace that funds someone else's compensation growth.
There is also a downstream effect that hurts the entire profession. Compensation surveys from MGMA and SullivanCotter use reported salary and productivity data. When the highest producers have their pay artificially suppressed, it pulls benchmark numbers down for every physician in that specialty the following year. The cap does not just limit one doctor. It compresses pay across the board.
Hursh says physicians need to review contracts for this language, demand regular and transparent productivity reports, and push for independent third-party compensation reviews when they are producing at the top of their field. The hospital should not be the one deciding whether the cap is justified.
The physicians most hurt by this are exactly the ones hospitals cannot afford to lose.
Listen to the full conversation on The Podcast by KevinMD. Link in the replies.
Have you seen this cap in your own contract? #ThePodcastbyKevinMD
@aniwacked@Hieronymou88829@soonerbrian91@imthewalruz@constans The average neurosurgeon was the top <1% of all medical students. If you're comparing, then the top 1% of front office finance should equate to the average neurosurgeon, but it seems that even then finance wins out.
I’m a physician who got rich from other things and quit medicine.
People are not understanding what the doctors in this thread are saying.
When doctors say “I’m in it for the money” it means they wouldn’t have gone into the profession if it didn’t pay well, not that they don’t care about saving lives.
Nobody in their right mind would become a physician in America if it didn’t pay well. It’s a hurculean, soul crushing endeavor where you sacrifice the prime of your life. Friends are lost, relationships ruined, health deteriorates as you study endlessly and work like a dog in high stakes situations while getting financially decimated.
The fat paycheck at the end of the tunnel when you’re 30+, burnt out, and in six figure debt is the only thing that makes the whole thing feasible in the real world (not all these larpers saying it should only and primarily be done from the goodness of the heart)
There is a lot wrong with today’s medical system and practice but it’s not the physician paychecks.
The ventricular insertion of the concealed nodoventricular pathway—once completely unknown❤️🔥
We finally mapped it and successfully ablated it🔥🔥
Collaboration with Drs. Tachi and Kaneko
Now expanding this ventricular insertion mapping—Looking for collaborators 🔥
#EPUniversity
#concealedNodoventricularPathway
CHAMPION-AF: My thoughts, especially in the context of CLOSURE-AF.
A quick summary of the trial and main findings:
1. 3000 patients randomized in 1:1 DOAC vs Watchman Fix, mean age 71, avg CV2 3.5.
2. Primary efficacy endpoint composite of CVD, stroke/SE
What to make of CLOSURE-AF? As an implanter of LAAO devices and clinical investigator in PREVAIL, CHAMPION-AF, and CATALYST, I'm a proponent of perc LAAO for appropriate patients and I am circumspect who should consider the procedure. I've advised against
Last month, a multidisciplinary heart care team at Sutter’s California Pacific Medical Center delivered a new option for patients with severe mitral valve disease.
Led by cardiologist Dr. David Daniels, structural heart section chief for Sutter Health’s Advanced Heart & Vascular Service Line, the team performed one of the first commercial transcatheter mitral valve replacement (TMVR) procedures in the United States using Edwards Lifesciences’ SAPIEN M3™ system.
“To witness the evolution of this therapy and to help bring forward what’s possible in cardiac care is an immense honor.” - Dr. Daniels
Read more on the huge impact this therapy will have on patients: https://t.co/qjcEGZnmUw.
#SutterProud
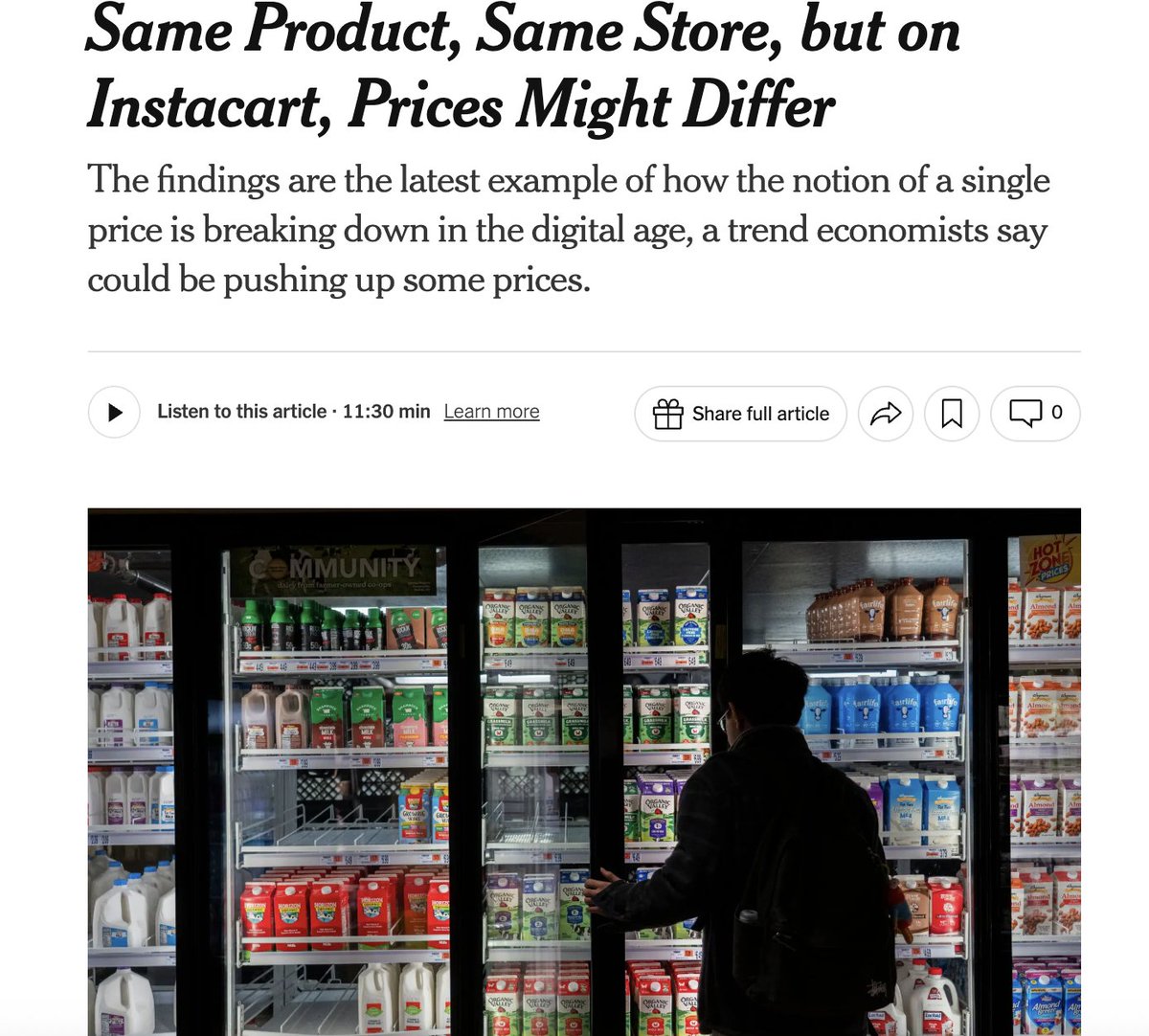
Right now, Instacart is quietly running experiments on millions of us while we shop for groceries online. They are trying to figure out exactly how much they can get away with charging you for breakfast cereal, lunch meat, pasta, and everything in between. How do I know? 1/9
The Number
72 of 100 U.S. senators took $10,000+ from pharma and health product PACs in 2024.
35 of those seats are on the ballot next November.
They voted to keep the physician ownership ban.
They killed site-neutral payment reform.
They defended CON laws.
The list is in the pinned post.
I am shocked and horrified by what I witnessed at a New York City hospital yesterday.
Suffering patients packed like sardines in the emergency room hallways.
A severely exhausted woman vomiting violently, with other patients just inches away from her.
She stayed there for hours, undergoing her full exams in front of everyone.
A patient with blunt trauma to the face, swollen and in pain, lying in a gurney at the edge of the hallway as people rushed back and forth past them.
An injured woman in her 90s, dazed, confused - being examined by doctors while surrounded on all sides by strangers and sick people.
Nurses and doctors with no choice but to have people’s most private conversations right there in the open.
We all learned about one man’s Crohn’s disease, and exactly where on his body he had rashes. We heard a woman’s entire history of neurological issues. A man discussed his STDs out loud.
Patients were told they needed to be admitted, but there were no available rooms.
Not today. Hopefully tomorrow.
So they stayed in that overcrowded room, packed in as far as you could see, forced to suffer in that environment with no idea how many more hours they’d be there, many trying to sleep sitting upright in a chair, with no bed.
Dignity?
Nowhere to be found.
And then something happened that I will never forget for the rest of my life.
A doctor approached a woman who was having cognitive issues and told her that her imaging had revealed a tumor in her brain. “I believe in being very truthful, and to let the prayers and the planning with your doctors begin as soon as possible."
I was standing three feet away, and turned away as I started to cry.
That woman did not deserve to have a room full of strangers witness the worst moment of her life.
Yet amid absolutely inhuman chaos, the shining light was the doctors, nurses, and hospital staff.
Overworked, exhausted, stretched past anything reasonable - yet still taking their time to make each patient feel as dignified and cared for as possible in an impossible scene.
I know they themselves are shocked by the situation they’ve been forced into, but you’d never know it.
The level of love they showed, the professionalism, the humanity in the middle of all that suffering…
These men and women are the best of America -
and we’ve put them in environments that are truly incomprehensible.
I kept thinking about how we possibly got here. How has this become the norm in America?
I kept thinking about how many freedoms we’re afforded in this country.
How many luxuries we’ve built.
How good life can be here.
And yet when it comes to what matters most, our healthcare, the thing we absolutely need to be there for us at our most vulnerable, it feels broken beyond repair.
I don’t know whose fault this is, and I don’t know what the solution might be, or if there is even one at this point.
On this particular day, I was just accompanying someone, only five hours in that environment.
But to the doctors, nurses, hospital workers, and the patients who have to live this reality, all I can say is:
I’m sorry.
You deserve better.
We all deserve better.
@DrDiGiorgio As an EP, I'd disagree that AC is over treatment. There is real morbidity (not even counting mortality) w ischemic CVA, and pts >80 are at higher risk for everything. If pt has h/o many falls, consider LAAO. I don't believe that no therapy is better than either therapy.